
Abstract
Abstract
Background:
Ventilator-associated pneumonia (VAP) secondary to Acinetobacter spp. in critically ill trauma patients has increased. More importantly, the incidence of multi-drug–resistant (MDR) Acinetobacter VAP has increased. The risk factors for this increase in resistance have yet to be elucidated. The purpose of this study was to evaluate the change in Acinetobacter sensitivity over time and determine which risk factors predict resistance in trauma patients.
Methods:
Patients surviving >5 days post-injury who had Acinetobacter VAP (≥105 colony-forming units/mL in bronchoalveolar lavage fluid) who were seen over five years were divided according to pathogen sensitivity (sensitive [SEN] vs. MDR) and stratified by age, severity of shock (base excess, number of blood transfusions), injury severity (Injury Severity Score [ISS], admission Glasgow Coma Scale [GCS] score, chest and extremity Abbreviated Injury Scale score [AIS]), and year. Prophylactic (Pro), empiric (Emp), Pro + Emp, and total antibiotic days, ventilator days, and mortality rate were compared. Multivariable logistic regression (MLR) was performed to determine which risk factors were independent predictors of resistance.
Results:
Ninety-six patients (81% male) were identified: 62 SEN and 34 MDR. The groups were clinically similar in terms of age, extent of shock, and injury severity with the exception of extremity AIS. Antibiotic exposure was greater in the MDR group. Over the period of the study, the incidence of MDR Acinetobacter VAP increased from zero to 66% (p < 0.0001). Multiple logistic regression identified Pro antibiotic days as an independent predictor of MDR after adjusting for age and chest AIS (p < 0.0001).
Conclusions:
The incidence of MDR Acinetobacter VAP has increased over time. More severe extremity injuries, as measured by the AIS, may contribute to prolonged antibiotic exposure in those patients with MDR Acinetobacter VAP. Multiple logistic regression identified Pro antibiotic days as an independent risk factor for MDR Acinetobacter VAP in trauma patients.
Multi-drug-resistant (MDR) strains of this pathogen have been emerging at an alarming rate. Approximately 30–40% of Acinetobacter spp. associated with VAP now are resistant to carbapenems [3]. Thus, with worsening resistance patterns and the limited availability of effective antimicrobials, prevention of pneumonia caused by this organism is paramount. Although a great deal of work has gone into identifying risk factors for pneumonia, such as higher Injury Severity Score (ISS), head injury, and, particularly, blood transfusions, little is known regarding the risk factors that lead to worsening resistance patterns of Acinetobacter pneumonia [4].
Given the recent increase in Acinetobacter VAP and the rapid development of MDR strains, the purpose of this study was to evaluate the change in Acinetobacter spp. sensitivity over time and to determine which risk factors predict resistant organisms in trauma patients with VAP.
Patients and Methods
Identification of patients
Patients admitted to the trauma ICU at the Presley Regional Trauma Center in Memphis, TN, from January 1, 2003, to January 1, 2008, who had Acinetobacter VAP diagnosed by bronchoalveolar lavage (BAL)(≥105 colony-forming units [CFU]/mL in the effluent) were identified from a prospectively maintained VAP database. Data were merged with additional patient information in the trauma registry (NTRACS version 3.5; Digital Innovation, Inc., Forest Hill, MD) to compile the database for this study.
Diagnosis and management of VAP
Ventilator-associated pneumonia was identified by quantitative culture of BAL fluid obtained by fiberoptic flexible bronchoscopic examination (Fig. 1). The clinical triggers for bronchoscopy with BAL sampling included any three of the following: (1) A new or changing infiltrate on chest radiograph; (2) abnormal temperature (>38° C or <36° C); (3) abnormal white blood cell count (>10,000/mm3 or <4,000/mm3); or (4) grossly purulent sputum.
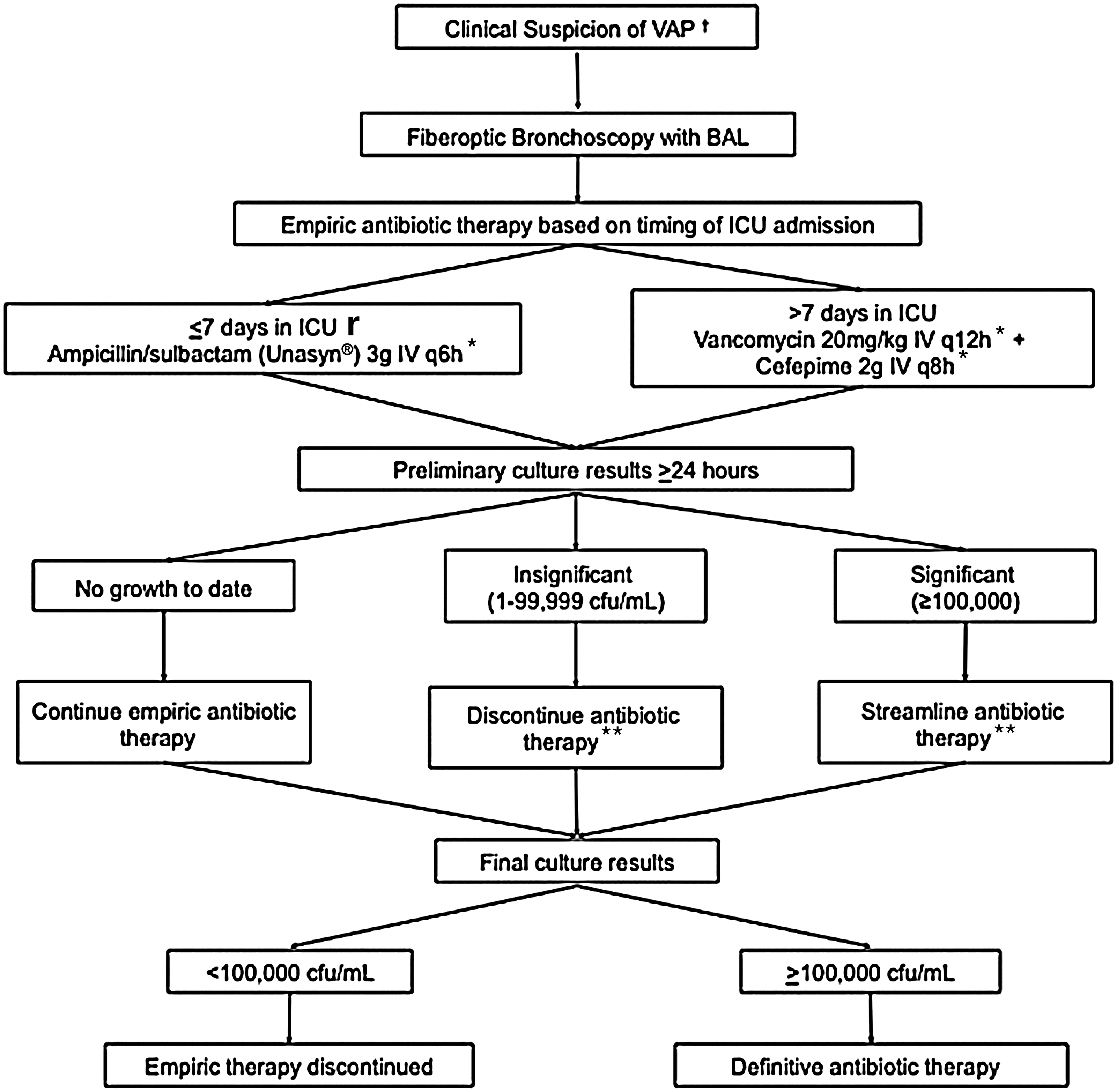
Clinical pathway for diagnosis and empiric management of ventilator-associated pneumonia, defined as any three of the following: (1) Appearance of a new or changing infiltrate on chest radiograph; (2) abnormal temperature (>38°C or <36°C); (3) abnormal white blood cell count (>10,000/mm3 or <4,000/mm3 or the presence of >10% immature bands); or (4) macroscopically purulent sputum. If patient has severe beta-lactam allergy, change ampicillin/sulbactam to moxifloxacin 400 mg intravenously (IV) q 24 h and cefepime to ciprofloxacin 400 mg IV q 8 h; dosage adjustment may be necessary if renal function is below normal. **Continue to monitor for changes in final culture results. BAL, bronchoalveolar lavage; ICU, intensive care unit; IV, intravenous; VAP, ventilator associated pneumonia.
All BAL procedures were performed in a uniform manner by the trauma ICU staff as described previously [5]. Briefly, following blind endotracheal suctioning through the ventilator circuit (performed twice to remove upper-airway secretions), the bronchoscope was advanced into the lung segment where the radiographic changes had been seen. When the bronchoscope was in the appropriate segment, 100 mL of non-bacteriostatic saline was instilled into the airway in 20-mL increments. The effluent was pooled and sent to the microbiology laboratory for gram stain and quantitative aerobic and anaerobic culture and sensitivity studies. Ventilator-associated pneumonia was confirmed at a threshold of ≥105 CFU/mL [5].
After the sample had been sent to the laboratory, all patients received empiric antibiotics according to the duration of the ICU stay using a unit-specific pathway [6]. Patients in the ICU for seven days or fewer were started on 3 g of ampicillin-sulbactam intravenously every 6 h (or equivalent alternative in penicillin-allergic patients), whereas patients in the ICU longer than seven days received vancomycin 20 mg/kg intravenously every 12 h (dose adjusted to maintain a steady-state peak serum concentration of 35 to 45 mg/L and a trough concentration of 15 to 20 mg/L) and 2 g of cefepime intravenously every 8 h. Antibiotic therapy was later tailored to the culture and sensitivity results in a timely manner.
Once a patient had been on adequate antimicrobial therapy for four days in the setting of late pneumonia pathogens according to the sensitivity patterns of the BAL specimen, a protocol bronchoscopy was performed, and another BAL specimen was obtained. If there were <104 CFU/mL of the initial organism, antibiotics were continued to a total treatment course of seven days. If there were >104 CFU/mL of the initial organism, antibiotics were continued to provide a 10- to 14-day treatment course, depending on the clinical response.
In our institution, patients with sensitive strains of Acinetobacter VAP are treated with ampicillin-sulbactam. If there is resistance to broad-spectrum penicillins, imipenem-cilastatin is the drug of choice. Carbapenem resistance is treated with colistimethate sodium. Lastly, those patients with Acinetobacter VAP resistant to all classes of antibiotics receive inhaled amikacin. All patients are treated using this protocol.
Patients surviving more than five days post-injury and having Acinetobacter VAP had their charts reviewed for age, severity of shock (as evidenced by base deficit and blood transfusions), injury severity (as evidenced by ISS, admission Glasgow Coma Scale (GCS) score, chest Abbreviated Injury Score [AIS] and extremity AIS) and year of diagnosis.
Outcomes
Outcomes, including ventilator days, ICU length of stay, antibiotic exposure, and mortality rates, were compared. Total antibiotic days were differentiated into empiric (Emp), prophylactic (Pro), and organism-specific (therapeutic) antibiotics. Prophylactic and Emp antibiotics were then classified together (Pro + Emp) as non-therapeutic.
The antibiotic sensitivity patterns were analyzed using the U.S. Centers for Disease Control and Prevention (CDC) definition of MDR [7]. In essence, Acinetobacter spp. resistant to two or more classes of antibiotics were designated MDR, and those resistant to no more than one class were labeled sensitive (SEN). Multivariable logistic regression was performed to determine which risk factors were independent predictors of resistant strains. Data also were examined to ascertain any relation between the year of VAP diagnosis and the percent of MDR organisms. Comparisons between the MDR and SEN groups were performed using the Student t-test and chi-square analysis as appropriate.
Results
Over the study period, 96 patients were identified as having Acinetobacter VAP. These patients ranged in age from 16 to 81 years and included 78 men (81%). A total of 62 patients had Acinetobacter baumanii strains resistant to a maximum of one class of antibiotics and comprised the SEN group, whereas 34 patients had strains resistant to two or more classes of antibiotics and formed the MDR group. The majority of patients (72
The SEN and MDR groups were clinically similar in terms of age, severity of shock (admission base excess and 24-h transfusion requirements), and injury severity (ISS, admission GCS, and chest AIS) (Table 1). The mean duration of pneumonia treatment was 8.2 days for the SEN group and 12.3 days for the MDR group (p < 0.001) with only 9% of the infections being secondary VAP. Interestingly, patients in the MDR group had significantly higher extremity AIS than those in the SEN group (2.2 vs. 1.4; p = 0.01). The characteristics of all study patients are summarized in Table 1.
AIS = Abbreviated Injury Score; NS = not significant (p > 0.05).
Outcomes, including ventilator support days, ICU length of stay, and death, were not statistically different in the two groups (Table 2). Interestingly, the incidence of bacteremia was not significantly higher in patients with MDR Acinetobacter VAP than in the SEN group.
NS = not significant (P > 0.05).
Not surprisingly, total antibiotic exposure, including total Pro antibiotic days, was significantly greater in the MDR group than in the SEN group (26 vs. 15 days; p < 0.001) (Table 2). Interestingly, total days of Emp antibiotics were not different in the two groups (2.5 vs. 1.8; p < 0.052)(Table 2).
The yearly incidence of MDR and SEN Acinetobacter VAP was examined. Despite relatively unchanged incidences of SEN infections, the incidence of MDR infections increased significantly over the study period, from 0 to 66% (p < 0.0001) with the greatest increase over the last two years of the study period (Fig. 2).

Significant increase in multi-drug-resistant Acinetobacter ventilator-associated pneumonia (VAP; black bars) compared with relatively unchanged levels of sensitive Acinetobacter VAP (white bars), 2003–2008. Number of patients with VAP is represented along the vertical axis; year of diagnosis is represented along the horizontal axis. *p < 0.001 vs. first study year (2003).
In an attempt to uncover a reason for this increase, antibiotic exposure (antibiotic days per patient [ADPP]) was examined by year and by sensitivity group. Total antibiotic exposure by year was evaluated according to the average non-therapeutic antibiotic days (Pro + Emp) and average therapeutic antibiotic days (Table 3). Interestingly, the total number of non-therapeutic ADPP remained relatively stable in the SEN group (range 3.4–4.7), whereas the ADPP in the MDR group was 1.5- to 3-fold higher than in the respective SEN groups.
Emp = empiric antibiotics; Pro = prophylactic antibiotics.
A logistic regression model was then developed using the database to predict development of MDR Acinetobacter VAP. The final resistance model included the independent variables Pro + Emp, age, chest AIS, and year of VAP. For this model, the odds ratios (ORs) are shown in Table 4. Both Pro antibiotic days (OR 1.87; p < 0.0001) and year of VAP (OR 3.208; p < 0.0022) were independent predictors of MDR Acinetobacter VAP. Extremity AIS was not an independent predictor (OR 1.23; p = 0.57) when added to the model, although Pro + Emp antibiotic days and year of VAP remained predictive.
Emp = empiric; Pro = prophylactic; NS = not significant (p > 0.05).
Discussion
The burden of nosocomial pneumonia is impressive, leading to more ventilator support days and ICU days and higher costs and mortality rates. Gram-negative pneumonias have greater virulence than pneumonia caused by gram-positive organisms [8]. In the past, Pseudomonas aeruginosa was the primary nosocomial pathogen of concern for ventilated patients. More recently, however, the emergence of Acinetobacter spp. has become a significant problem in VAP [9]. Unlike P. aeruginosa, few empiric treatment pathways for VAP include coverage of Acinetobacter spp. Even more problematic is the rise in MDR variants of this organism.
Over the study course, the total number of Acinetobacter VAP cases increased dramatically (from 0% to 66%). Interestingly, the total number of non-therapeutic (P + E) ADPP remained relatively stable in the SEN group (range 3.4–4.7) over the same period (see Table 3). The total number of yearly SEN VAPs has remained relatively stable despite comprising a smaller fraction of the total Acinetobacter VAP burden.
This has not been the case in the MDR group. In 2003, there were no patients with MDR Acinetobacter VAP, whereas in 2007, 23 patients had MDR VAP. In fact, the majority (88%) of the MDR VAP occurred in the last two years of the study. Multivariable logistic regression points to non-therapeutic (P + E) antibiotic days as a potential reason for this increase.
Recent data from the CDC show that Acinetobacter accounts for 8.4% of all reported VAP [3]. This figure is consistent with data from the current study in which Acinetobacter spp. were responsible for 8.7% of the total VAP cases. From 2003–2004, only 7% of Acinetobacter VAP was MDR; 2003–2005 showed only 10% MDR strains. These percentages are in sharp contrast to the entire time course of the study, which shows that 35% of Acinetobacter VAP involved MDR strains. These data are concordant with national statistics showing an increase in carbapenem resistance from 9% to 40% between 1995 and 2004. These data are alarming, as Acinetobacter pneumonia has become an international problem [10].
The reason for the relation between antibiotic administration and the development of MDR VAP lies in the intrinsic resistance mechanisms of A. baumannii, including β-lactamases, drug efflux pumps, and cell-surface modifications. These mechanisms are a major problem with A. baumannii infection, and particularly during VAP treatment. Strains resistant to a plethora of antimicrobial agents have been found, including broad-spectrum beta-lactams, carbapenems, aminoglycosides, fluoroquinolones, and, more recently, polymyxin [11].
Nevertheless, carbapenems remain drugs of choice for the treatment of A. baumannii infection, although their efficacy can be compromised by the spread of novel class D carbapenemases [12]. As a result, carbapenem-intermediate or -resistant A. baumannii isolates are becoming increasingly prevalent. Colistin, an antibiotic from the polymyxin group, is effective against MDR A. baumannii isolates, but resistance has been seen occasionally [13].
Other antimicrobial agents such as tigecycline, which is in the tetracycline class, have been effective against A. baumannii infections, including those resistant to carbapenems. Still, resistance to tigecycline has been identified [14], and mere exposure to this antibiotic may facilitate the development of resistant strains [15]. Although no patients were treated with tigecycline in this study, it is possible that similar mechanisms for increased resistance occur with antibiotic overuse, as is the case with certain quinolones and cephalosporins [16].
When MDR isolates correlate with the total number of antibiotic days, as in this study, it is possible that mutations leading to resistance occur within weeks. On a broader scale, work by Villers et al. showed that fluoroquinolone therapy was responsible for the persistence and epidemic spread of MDR A. baumannii clones for at least five years [17].
Infections with early strains of Acinetobacter were treated with broad-spectrum penicillins such as ampicillin-sulbactam, but in the past decade, resistance to these drugs has grown dramatically. Not only has this led to the use of stronger agents such as carbapenems, but resistance to carbapenems has led to usage of colistin. In the last few years, a number of reports have documented resistance to this antibiotic as well. The end result has been an attempt to alter and modify the delivery of agents. One such example is the use of inhaled antibiotic, with some promising results [18,19].
Nevertheless, the rapid development of resistant strains creates worries that these newer agents also may become ineffective. This possibility underscores the importance of identifying risk factors that may be modified to decrease resistance. In the current study, multi-drug resistance increased from 0% to 66% over a five-year period. Clearly, patient characteristics played little, if any, role, as the groups were clinically similar over the study period. More likely, the development of multi-drug resistance is related to antibiotic exposure. Furthermore, the absence of differences in ISS, ventilator support days, and ICU length of stay highlights the finding that patients with MDR infections do not have a higher burden of disease than the SEN group. There is, however, a trend toward longer ICU stays, with the 2007 VAP data showing a significant increase in the length of stay in the MDR group compared with the SEN group, although this difference was not seen in any other year.
The reasons for greater antibiotic exposure also may relate to higher extremity AIS (1.4 SEN vs. 2.2 MDR). This may be attributable to antibiotic administration over long periods of time secondary to open fractures. One can surmise that early fixation or any non-essential delays contribute to increased resistance patterns secondary to a need for antibiotics in the open fracture setting. This becomes most apparent when looking at the logistic regression analysis: Although extremity AIS correlated highly with MDR Acinetobacter VAP, it is not an independent predictor. Clearly, total antibiotic days play a more important role.
At present, patients with open fractures are treated with cefazolin and gentamicin, which are continued until definitive fixation. Although no explicit change occurred over the course of the study in the treatment of these fractures, it is possible that decreased availability of subspecialty support and stricter criteria for preoperative clearance are responsible in part for delays in fixation and, ultimately, in the increase in non-therapeutic use of antibiotics over time.
Furthermore, delays in mobilization may contribute to more ventilator days, longer ICU stays, and greater exposure to potentially virulent organisms. Although there was a trend toward increased ISS, ventilator support days, 24-h blood transfusions, bacteremia, and mortality rate, there was no significant difference between the MDR and SEN groups. It is possible, however, that patients in the latter part of the study had more severe injuries.
This result demonstrates the need for effective diagnostic techniques so that adequate therapy may be initiated [20]. Prevention of VAP in less severely injured trauma patients should increase survival. Finding risk factors that lead to the development of VAP are the key to improving outcomes. There is a great deal of data showing the value of ventilator bundles [21] and appropriate transfusion triggers in reducing VAP rates [22]. Although this is true for VAP in general, work still needs to be done with regard to decreasing antibiotic resistance. One may infer from this study that judicious use of antibiotics may decrease the likelihood of infections with MDR strains of Acinetobacter spp.
Author Disclosure Statement
No conflicting financial interests exist.
Footnotes
Presented at the Thirtieth Annual Meeting of the Surgical Infection Society, Las Vegas, Nevada, April 17–20, 2010.