
Abstract
Abstract
Background:
Submucosal abscesses are rare in the gastrointestinal tract. Although they have been reported throughout the tract, occurrence within the appendix has not been described.
Methods:
Case report and review of the current literature.
Results:
We present the case of a patient with a periappendiceal mass found incidentally on workup for anemia. An ileocecectomy was performed for presumed cecal neoplasm. Histologic examination showed a submucosal periappendiceal abscess with no evidence of malignancy.
Conclusion:
This case is unique because although appendiceal abscesses often occur as a result of acute appendicitis, our patient presented with an incidental periappendiceal submucosal abscess, not preceded by any gastrointestinal infection or surgery. Periappendiceal submucosal abscess should be included in the differential diagnosis of masses found on colonoscopy.
Case Report
A Hawaiian woman in her fifth decade was found to have normocytic, normochromic anemia (hemoglobin 9.4 g/dL) on routine laboratory analysis. Further questioning elicited reports of fatigue, occasional dyspnea on exertion, and menorrhagia. Her medical history was remarkable for breast cancer, which was treated with a mastectomy and reconstruction with a traverse rectus abdominis muscle flap. The patient's history of menorrhagia was considered the likely etiology of her anemia, and she was subsequently referred to the gynecology service, where she was found to have uterine fibroids. Simultaneously, she was referred to the gastroenterology department to rule out an enteric source of the anemia.
The gastroenterologist performed upper and lower tract endoscopy. The esophagogastroduodenoscopy was normal. The colonoscopy was remarkable for what was interpreted as extrinsic compression of the cecum (Fig. 1). Given the interpretation of this condition as external compression, no biopsy was performed. A computed tomography (CT) scan was obtained of the abdomen and pelvis to define the source of extrinsic compression and demonstrated a 1.3×1.0-cm mass at the appendiceal orifice (Fig. 2). She was referred to a colorectal surgeon for evaluation.
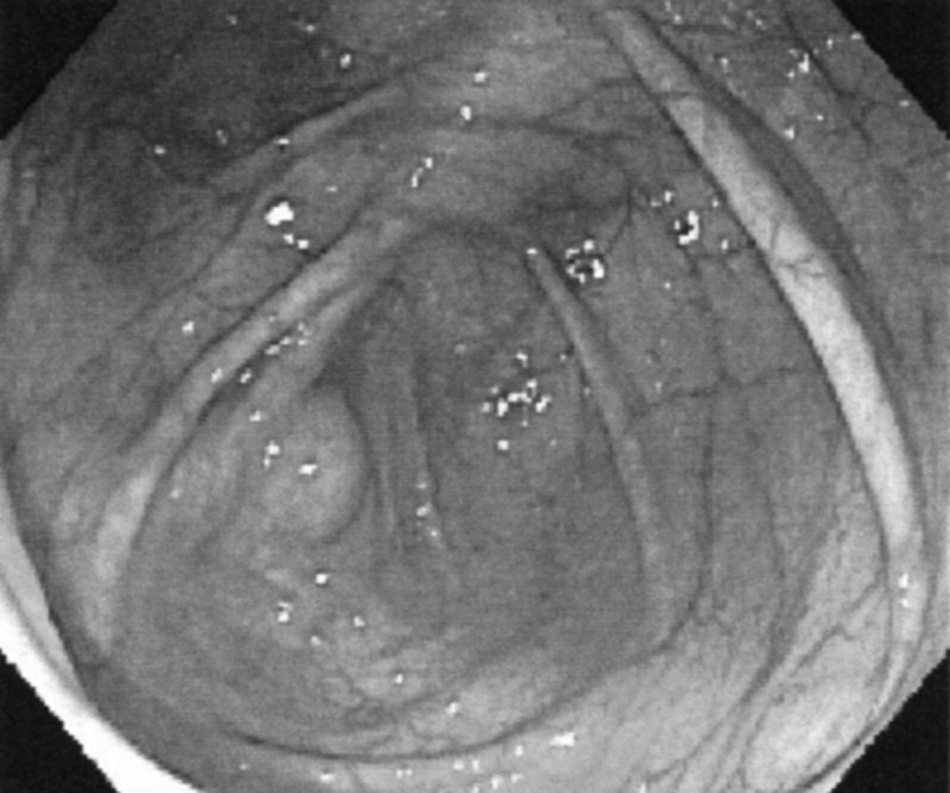
Colonoscopy demonstrating external compression of appendiceal orifice.

Computed tomography scan demonstrating 1.3×1.0-cm low-density filling defect at appendiceal orifice.
After the CT scan, the patient began to complain of occasional ill-defined right lower-quadrant abdominal pain. She denied having any fever, chills, diarrhea, melena, or bright red blood in her stool. She did not have a history of appendicitis, but did have a history of multiple axillary abscesses. It was recommended that she undergo resection of the mass in order to obtain a diagnosis, and she was counseled on the options of open vs. laparoscopic resection. She ultimately elected to undergo an open resection.
She was taken to the operating room, where an open ileocectomy was performed through an 8-cm Rocky-Davis-style incision centered over her transverse rectus abdominis muscle flap scar. Intra-operatively, a 1.5-cm soft, mobile mass was found at the base of the appendix and removed en bloc with the terminal ileum and cecum. Subsequent histologic examination demonstrated the mass to be a 1.5×1.5 cm submucosal abscess at the base of a 6.1×0.4 cm appendix. The appendix was otherwise normal. There was no evidence of malignancy.
The patient is now one year out from her surgery and has recovered fully without recurrence of her pain. She continues to have a normocytic, normochromic anemia and was offered hysterectomy to stop the menorrhagia; however, she has declined the operation.
Discussion
Gastrointestinal submucosal abscesses have been described in the esophagus, stomach, small bowel, and colon [1–4]. Despite the wide variety of locations, reports in the English-language literature are limited, suggesting that the incidence is low. However, if the reported cases are representative of the incidence in general, the stomach is the most common site of involvement, followed by the proximal small bowel.
No unifying mechanism of genesis of submucosal abscesses has been identified. Instead, several distinct sources have been suggested, including direct invasion of bacteria through intact mucosa, foreign-body ingestion, tumor necrosis, localized inflammatory processes, or hematogenous spread from distant infections [2–8]. In the case presented herein, the patient had no immediate precipitating factors for the development of this appendiceal abscess. Specifically, she had no history of appendicitis, enteric malignancy, or recent infection. Possible etiologies of this insidious abscess are hematogenous spread from her axillary abscesses or chronic subclinical appendicitis; however, this remains purely speculative.
The absence of signs of inflammation and infection in this patient is similar to what has been reported previously [6,7,9]. Furthermore, having these abscesses present as a mass suggesting malignancy is not uncommon. In separate reports by Chen et al. and Kim et al., isolated submucosal abscesses of the stomach presented as possible gastric malignancies [6,9]. In each case, the patient underwent a subtotal gastrectomy, and the final pathology report described the mass as an abscess. Pre-operative diagnosis in this setting can be difficult, and seems possible only when an endoscopic biopsy is accompanied by the immediate finding of purulent material draining from the biopsy site [10,11]. Barring this scenario, most patients will ultimately undergo a resection.
The finding of an appendiceal mass can present a diagnostic dilemma in the absence of other symptoms. Most masses are either infectious or neoplastic in origin. Among the infectious sources, masses secondary to an episode of acute appendicitis predominate, with most being either a periappendiceal abscess or a phlegmon. These often can be diagnosed from a thorough history and a CT scan with findings demonstrating surrounding inflammatory changes. Appendiceal infectious masses not associated with appendicitis often can be treated with drainage and antibiotics alone. If the mass is limited to the submucosa, as in our patient, internal drainage through an endoscopic approach can be sufficient. When the mass accompanies an episode of appendicitis, the traditional dictum has been to perform either emergency appendectomy or drainage followed by an interval appendectomy. Several recent reports have questioned this advice, citing a low recurrence rate and a not-insignificant risk of complications associated with surgery [12]. Accordingly, until definitive research is completed, we recommend a thorough discussion with the patient of the risk of a recurrent episode of appendicitis vs. surgical intervention and tailoring the recommendations to the individual patient.
Non-infectious appendiceal masses are most frequently adenocarcinoma, mucosa-associated lymphoid tumors, carcinoids, or mucoceles [13]. These masses should be evaluated with endoscopy and CT scanning. Endoscopic examination should include a biopsy of the mass, and if the surgeon is uncertain as to the origin of the mass (if accessible endoscopically), consideration should be given to a bite-on-bite technique. This technique is especially useful for masses believed to be arising from the submucosa or deeper. If this biopsy proves to be non-diagnostic, consideration should be given to en bloc resection for both diagnosis and definitive therapy. On the other hand, if a cause of the mass is determined, the type of resection should be tailored to the location of the mass in relation to the appendiceal orifice and its size [14].
In conclusion, this case was unique in that the patient had a submucosal abscess located in the appendix, without a preceding acute appendicitis or other infectious process. Periappendiceal submucosal abscess should be considered in the differential diagnosis of a presumed cecal or appendiceal neoplasm.
Author Disclosure Statement
The views expressed in this manuscript are those of the authors and do not reflect the official policy or position of the Department of the Army, Department of Defense, or the U.S. Government.