
Abstract
Abstract
Background:
Suppurative kidney infections (SKIs) have potentially lethal implications and a high incidence of treatment-related morbidity and death. Until this point, there has been no study that has derived a prognostic model for adverse early outcomes in SKI. Therefore, our aim was to derive and validate a simple scoring system of early treatment failure in SKI.
Methods:
Logistic regression and bootstrap methods were used to create an integer score for estimating the risk of early treatment failure using patient characteristics, severity of disease, bacterial etiology, type of pathology, initial antibiotic therapy, and early urologic procedures.
Results:
This study included 92 adult patients with 104 SKIs. Early treatment failure was observed in 57 patients (54.8%). The length of the hospital stay and the treatment complications were significantly longer and more common, respectively, in patients with early treatment failure. The factors associated most strongly with early treatment outcome were whether there had been an early complete urologic procedure, the adequacy of early antibiotic therapy, and the presence or absence of sepsis syndrome. The total possible score ranged from 0 to 22 points, with a cut-off value of 5 points. A score of ≤ 5 points identified early success correctly in 85.3% of patients, whereas a score > 5 points correctly identified early failure in 93.2%. The scoring system retained its predictive ability on the validation set.
Conclusion:
A scoring system was created to predict early treatment failure for a given patient with SKI. Although the system has good performance characteristics and provides a possible intervention measure, further studies should be performed before widespread implementation.
The distinction between early and late treatment failure was first made in community-acquired pneumonia (CAP) [6], which showed that initial appropriate treatment correlated with a favorable clinical response. These studies have enabled the identification of risk factors for treatment failure and the design of different strategies for these patients [7,8]. Moreover, early treatment failure increases the need for microbiological and diagnostic tests, with a resulting longer hospital stay and higher cost.
Several tools have been developed for severity stratification in infectious diseases. They include biochemical markers, imaging methods, and prognostic models or complex scoring systems, all of which aim at early detection of severe infections. For most infectious diseases, prognostic estimates of clinical outcome have been studied most extensively because they have a profound impact on diagnostic work-up, site of care, and optimization of monitoring and treatment of patients as early as possible [9]. Therefore, similar efforts to optimize the healthcare process for patients with SKI are warranted. Until this point, there has been no study that has derived or validated a prognostic model that stratifies patient risk for adverse early outcomes after urinary tract infection.
Against this background, the aim of this study was to identify relevant prognostic factors and to generate and validate a simple scoring system for early treatment failure in patients with SKI that could stratify patients accurately by their risk, and provide a possible intervention measure.
Patients and Methods
We reviewed retrospectively the medical records from the Clinic of Urology and Nephrology at Kragujevac for the ten years from January 2000 through December 2009. We included only patients who had a final discharge diagnosis of SKI (renal or perirenal abscess, pyonephrosis, or xanthogranulomatous or emphysematous pyelonephritis). There were a total of 106 SKI encounters, of which drainage or surgical procedures were performed in 104 (98.1%); these cases were used in the study.
Outcome measure
The patients were assessed throughout the duration of hospitalization. However, for the purpose of the scoring system, two cross-sectional assessments were crucial: At the initial presentation, and at early outcome. We used early clinical failure as the primary endpoint. The mode and success of early treatment was defined as described previously [5]. Initial (early) treatment failure was diagnosed if there was persistence of symptoms or signs of infection beyond four days of hospitalization, regardless of the initial treatment mode. We did not include late end points (length of hospital stay, early recurrence, death) in an effort to simplify the score and maximize its predictive value for the primary outcome measure, but we did use these data in the secondary analysis.
Predictor variables
The following predictor variables were chosen a priori for the defined outcome: Demographic data (age, gender), laboratory data (leukocyte [WBC] count, hemoglobin concentration [Hgb], serum creatinine concentration), predisposing medical conditions, severity of disease, bacterial etiology, type of pathology, initial antibiotic therapy, and early urologic procedures.
The following conditions were considered in the evaluation of the patients' previous health: Diabetes mellitus, chronic renal failure, congestive heart failure, cirrhosis of the liver, malignancy, site of acquisition (e.g., community or nosocomial), immunosuppression, severe neurologic impairment, and treatment outside the urology department.
For the purpose of the analysis, all purulent infections were categorized into three main types. Type one was a unilocular abscess of the kidney or its extension to the perirenal space, or a dominant solitary perirenal collection. Type two was defined by the presence of pyonephrosis or xanthogranulomatous pyelonephritis only. Type three was renal infection extending into adjacent tissue or serous membranes, gas-forming infections, and bilateral or multiple collections.
Sepsis syndrome was defined on initial presentation, before the decision time-point of early treatment failure, as the presence of the systemic inflammatory response syndrome along with a systolic blood pressure of < 90 mm Hg or a reduction of > 40 mm Hg from baseline, organ dysfunction, hypoperfusion and perfusion abnormalities or hypotension despite adequate fluid resuscitation, extension of infection to the peritoneum or pleura, or serious remote infection.
Microbiological samples included purulent discharges taken directly during urologic procedures, urine, and blood. All specimens were tested in the local microbiology laboratory of the Public Health Institute. The analysis included culture and identification of aerobic bacteria and sensitivity testing of the isolate against a range of antibiotics.
Initial empiric antibiotic therapy was classified as appropriate if all isolates were sensitive to at least one of the antibiotics administered. Patients with negative or no culture results were considered to have had appropriate empiric therapy if the regimen administered had followed local guidelines for antibiotic treatment in urinary tract infections [10] (modified from 11).
Urologic procedures were considered adequate (complete drainage or adequate source control) if nephrectomy had been performed or if all purulent collections had been drained, exept in the cases of small renal or perirenal abscess, according to the principles of successful outcomes of larger abscesses [12,13].
Derivation and validation sets
The patients were randomized into a derivation set (three-fourths of patients) and a validation set (one-fourth of patients). The validation set was not used until after the multiple logistic regression model and the scoring system had been created.
Statistical analyses
Univariable analysis was carried out initially to search for the factors associated significantly with possible risk factors for early clinical failure. Only variables that showed a statistically significant association (p < 0.05) were included in the multivariable model. Multiple logistic regression analysis was used (with Backward–Wald stepwise regression) to adjust for potential confounders and to identify and quantify the independent predictors of treatment failure. The results of regressions were expressed in odds ratios (ORs) with 95% confidence intervals (CIs). The Hosmer-Lemeshow goodness-of-fit test was performed. Non-significant p values on this test imply good fit. Next, logistic R-square was determined as a measure of effect size. To examine the stability of the model's effect estimates and check for over-fitting, we used bootstrapping methods to generate 1,000 samples; the medians of the resultant beta coefficients for each variable were reported. The median beta coefficients were used to develop an integer-based weighted point system for early treatment failure. The coefficient for each variable was multiplied by 20 and rounded off to the nearest integer. Individual scores were assigned to each patient-discharge record by summing the individual risk factor points. The cut-off points for predicting early treatment failure were identified as the score giving the best Youden index (sensitivity + specificity - 1) for each scoring system with the best discriminating power.
Finally, the validation set was used to test the rule. Validation of a prognostic model means establishing that it works satisfactorily for patients other than those from whose data the model was derived. It includes comparison of observed and predicted event rates for groups of patients (calibration) and measures that distinguish between patients who experience the event of interest and those who do not (discrimination) [14], and was quantified by the areas under receiver operating characteristic (ROC) curves. The sensitivity, specificity, overall correctness of prediction, and positive and negative predictive values for scoring systems were determined. In order to judge the risk score's calibration, comparison tables were constructed to assess the observed vs. expected early treatment failure rates by percentages in both the development and validation sets. All analyses were performed using SPSS version 13.0 (SPSS Inc., Chicago, IL).
Results
Patient characteristics
This retrospective cohort study design included 92 patients with 104 SKIs, four (4.3%) being recurrent infections (median and interquartile [IQR] range 14.5 and 20 mos; range 12–37 mos after the initial infection) and four (4.3%) with infections on the opposite side (9.5, 48.7, 1, and 65 months, respectively). The age range was 21–80 years, with a mean age of 55.9 ± 13.6 years. Males constituted 41.3% (43) of the study patients.
The underlying medical disorders were diabetes mellitus (20; 19.2%), chronic kidney disease (15; 14.4%), malignant disease (15; 14.4%), nosocomial origin of infections (22; 21.2%), congestive heart failure (6; 5.8%), treatment outside the urology department (35; 33.7%), neurologic impairment (4; 3.8%), immunosuppression (2; 1.9%), and cirrhosis of the liver (1; 1%). In 37 (35.6%) of the patients, no underling disorders were discovered.
Twenty-one patients (20.2%) were critically ill at presentation, of whom seven (6.7%) had acute kidney injury treated by haemodialysis, six (5.8%) peritonitis, two (1.9%) empyema of pleura, two (1.9%) septic shock, and four (3.8%) hypotension. Purulent meningitis, deep venous thrombosis of upper leg, lethargy, and liver failure with jaundice was present in one patient each (1%). Five patients had two complications.
Microbiology findings
Microbiologic samples were obtained from 23 patients (22.1%). From the total of 138 microbiological specimens, there were 78 positive findings (56.5%). Cultures of purulent material were carried out in 64 patients (61.5%), of which 13 (20.3%) were sterile. Urine cultures were carried out in 47 patients (45.2%), of which 23 (48.9%) had pathogens isolated. Finally, blood cultures were positive in four (14.8%) of 27 patients. Overall, 79 bacteria were recovered in samples taken from 59 patients (56.7%). Enterobacteriaceae were isolated in 49 patients (47.1%), whereas non-Enterobacteriaceae were isolated from 19 patients (18.3%). In nine patients, there were Enterobacteriaceae and non-Enterobacteriaceae together. The most frequent species recovered from the 79 bacterial cultures was Escherichia coli (22; 27.8%), followed by Proteus spp. (19; 24%), Pseudomonas spp. (17; 21.5%), Klebsiella spp. (12; 15.2%), Staphylococcus aureus (2; 2.5%), Acinetobacter spp. (2; 2.5%), Enterobacter spp. (2; 2.5%), and one instance each (1.3%) of Enterococcus faecalis, Corynebacterium spp., and Providencia rettgerii. For further statistical analysis, the study sample was divided according to the presence of Enterobacteriaceae and non-Enterobacteriaceae isolates only (Tables 1 and 2).
Other co-morbidities not analyzed as separate variables.
See text for explanation.
SD = standard deviation; IQR = interquartile range; WBC = white blood cell.
Only factors with statistically significant influence on outcome.
CI = confidence interval; OR = odds ratio.
Pathological findings
The first type of purulent collections appeared in 24 subjects (23.1%) and included five unilocular intrarenal abscesses, four renal/perirenal suppurations, and 15 solitary perirenal collections, of which one had radiologic features of a gas-containing infection. The second type of collection appeared in 44 subjects (42.3%) in whom pyonephrosis (39) and xanthogranulomatous pyelonephritis (5) were detected. Type 3 infection was observed in 36 patients (34.6%). Twenty-eight patients had pyonephrosis or xanthogranulomatous pyelonephritis (5) with perirenal abscesses (26) or solitary (2) or multiple (3) renal abscesses, whereas eight patients had multiple perirenal abscesses. There were 11 psoas abscesses, nine suppurations had an emphysematous character, and eight had extended to the serous membranes.
Early antibiotic treatment
No patient was without antimicrobial therapy, and many received multiple agents, but appropriate empiric antimicrobial therapy was begun in 57 patients (54.7%), of which about one-half (31; 54.4%) was determined according to the bacterial sensitivity pattern. The adequate initial antibiotics were third-generation cephalosporins in 38 patients (57.6%), aminoglycosides in eight (12.1%), antipseudomonal cephalosporins in six (9.1%), carbapenems in four (6%), glycopeptides in four (6%), and others in six (9.1%), taking into account that nine subjects (13.6%) initially received combination therapy.
Urologic procedures
A total of 154 urologic interventions were performed, in most cases once (62 patients; 59.6%), less frequently twice (35; 33.7%), and rarely thrice (6; 5.8%) or four times (1; 1%). The average number of procedures was 1.48 ± 0.65. During the early course of illness in 60 patients (57.7%), 65 urologic procedures were performed, which included 11 percutaneous (PC) drainages, five lumbar drainages, 14 PC nephrostomies, 11 retrograde stent placements, 21 nephrectomies, and three laparotomy drainages, taking into account that three subjects and one, respectively, had two or three urologic procedures. Initiation of urologic procedures was performed at 3.6 ± 2.2 days, with a range of the first to the seventh day of hospitalization. However, in nine patients, drainage procedures were considered incomplete, because not all purulent collections were drained. During all treatment courses, in 59 patients (56.7%) nephrectomies were performed. There were seven (6.7%) early abscess recurrences, and five (4.8%) late (after 12 mos) recurrences. The length of hospital stay of the patients who survived and who were followed up for at least six months (97; 93.3%) was significantly longer (p = 0.00) in the early failure group (median and IQR 33 and 23 days, respectively) than in the early successes (25 and 14.5 days). The in-hospital mortality rate was 4.8% (5), and four patients (3.8%) died within the one-year follow-up period, giving an overall mortality rate of 8.6%. Treatment complications (early recurrences and in-hospital death) were seen more commonly in patients with early treatment failure than in those with early success (19.3% vs. 0; p = 0.001).
Prediction and scoring system of early treatment failure
Early treatment failure was observed in 57 patients (54.8%). The group was divided randomly into a derivation set (three-fourths or 78 patients) and a validation set (one-fourth or 26 patients). The derivation and validation groups were similar with respect to demographic characteristics, laboratory data, predisposing conditions, type of purulent collections, positive cultures, adequate early antibiotic treatment, early applied urologic procedures, and percentage of early treatment failure (see Table 1).
In a univariable analysis, seven risk factors displayed significant correlation with early treatment failure (see Table 2). During multivariable analysis that included these seven parameters as covariables, three sustained their prognostic significance (Table 2). The analysis demonstrated that early complete urologic procedures, inadequate early antibiotic therapy, and sepsis syndrome have strong prognostic value in predicting the early outcome (Table 2). All variables maintained significance in the bootstrap model (Table 2); thus, the model was considered to be reliable and not over-fit. The Hosmer-Lemeshow goodness-of-fit test statistic was p = 0.437 for the derivation set, thereby demonstrating good fit. The C-statistic for the model and validation set was 0.897 and 0.922, respectively, demonstrating that the model performed well in identifying patients with early treatment failure. A coefficient of reliability (Cronbach's alpha) was −0.7056, which is considered acceptable.
Next, a total score was calculated by summing the points from each variable for each patient. The resultant total possible score ranged from 0 to 22 within both the development and the validation set, with a cut-off value of 5 points. The areas under the ROC curves for the model and validation set score were 0.944 (95% CI 0.867-0.983) and 0.973 (95% CI 0.82-0.991), respectively, showing the score to have good discriminatory ability, and it retained its predictive ability on this separate population of patient encounters (Fig. 1). Because of the small number of patients in the validation set, the ROC curve graphic was considered inappropriate. The sensitivity was 89.13% (95% CI 76.4-96.3%) in the derivation set and 90.9% (58.7-98.5%) in the validation set. The specificity was 90.6% (75-97.9%) and 93.3% (68.0-98.9%), respectively. The positive predictive value was 93.2% in the derivation set and 90.9% in the validation set, whereas the negative predictive value was 85.3% and 93.3%, respectively. In other words, a score of ≤ 5 points identified early success correctly in 29 of 34 patients (85.3%) in the derivation group and 14 of 15 patients (93.3%) in the validation set, whereas a score of > 5 points identified early failure correctly in 41 of 44 patients (93.2%) in the derivation set and 10 of 11 (90.9%) in the validation group. Graphic assessments of score calibration are presented in Figure 2 for the development set and Figure 3 for the validation set. The model shows excellent calibration.

Receiver operating characteristic curve analysis for predicted outcome in derivation set by score.
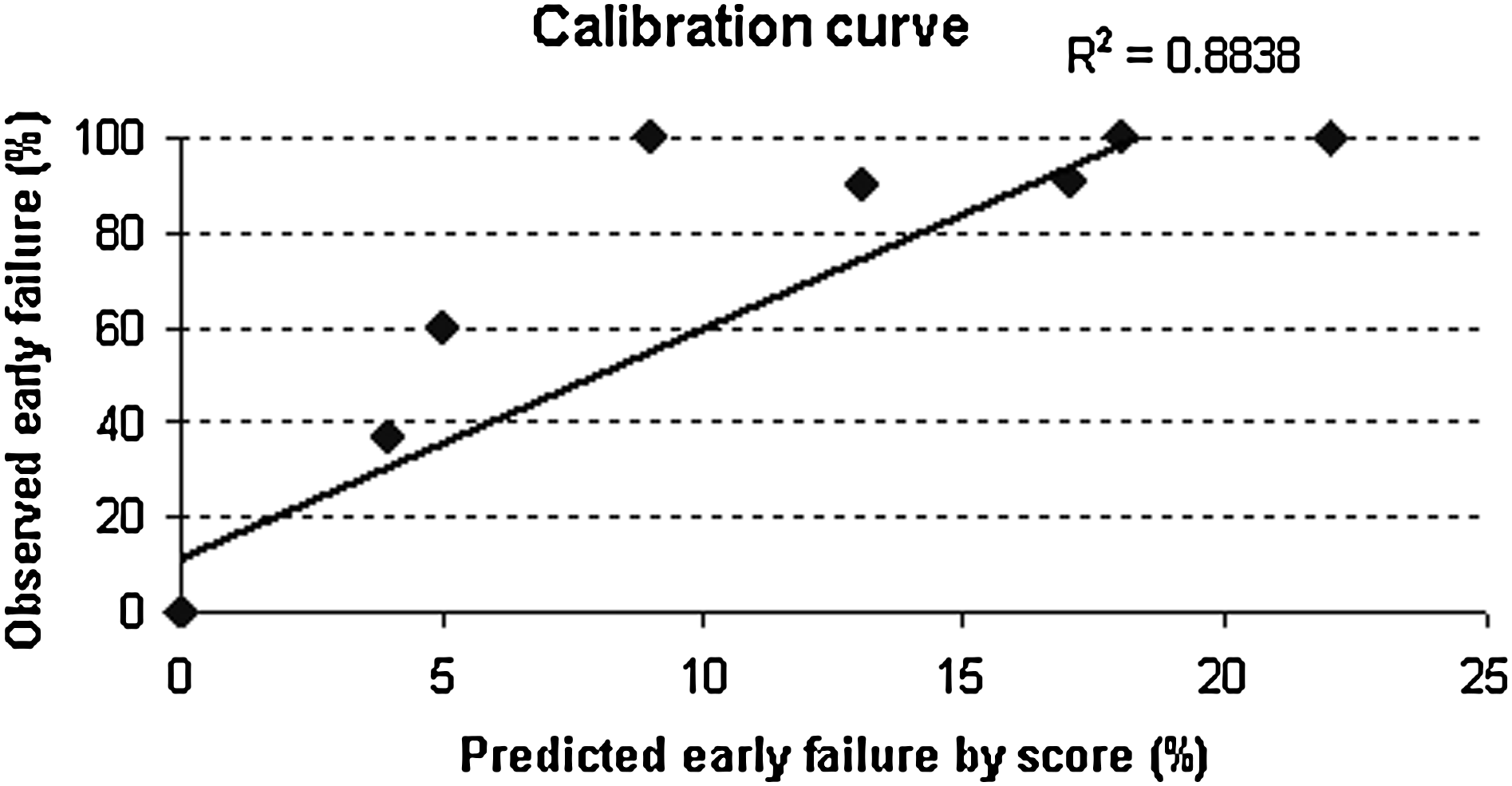
Observed vs. predicted early failure in derivation set by score.

Observed vs. predicted early failure in validation set by score.
Discussion
In this study, we derived and validated a new prognostic model and scoring system that predicted early treatment outcome in SKI. The factors associated most strongly with early treatment failure were early complete urologic procedures, inadequate early antibiotic, and sepsis syndrome. These variables can easily be identified during initial patient evaluation. This relatively simple model, a bedside tool, could help a physician to predict more confidently the early outcome of the illness after initial therapeutic measures and, consequently, introduce more appropriate subsequent interventions.
Several research groups have already identified all of the predictors revealed in our study as the most important prognostic factors for the outcomes in SKI [5,12,13]. Previous studies have shown that a variety of patient characteristics [3,15,16], underlying conditions [17], bacterial factors, pathology type [3], severe clinical course [4,15,18], and method of treatment [1,2] are crucial to the final outcome in renal infections. However, the validity of such findings could be questioned because some tested factors are not related directly to early or final outcome. Moreover, in some studies [4,16], the final model did not include adequate antimicrobial therapy. In accord with previous reports, in patients with acute pyelonephritis [18], the presence of sepsis syndrome (septic shock) at presentation correlated independently with early treatment failure, but that proposed model has been evaluated only in the patients from whom it was derived. The main contribution of our study is that it has integrated all these predictors into a model and, at the same time, predicted early treatment failure fairly well.
The main reason for the good predictive power of our tool probably originates from the fact that it includes the factors crucial for the core of pathological events and excludes the confounders. For example, there is strong evidence that early inadequate antibiotic treatment of nosocomial infections represents an independent factor for a higher hospital mortality rate [19] and that de-escalating antibiotic therapy is a beneficial practice [20]. Furthermore, our final model does not include the bacterial species, which is in concordance with findings that the identity of the infecting organism is of little consequence for most patients with severe infections provided appropriate antimicrobial therapy is administered promptly [20]. However, the results of our study of antimicrobial therapy and causative pathogens should be interpreted carefully, taking into account inherent difficulties arising from issues concerning temporal trends [21], difficulty in obtaining a microbial diagnosis [4,22], and regional [23] or institutional [24] differences.
The main difficulty in elaborating a risk score for SKI is related to the complexity and heterogeneity of the disease. We believed that the introduction of rigorous statistical computation, which, as a rule, have not been applied in similar urologic studies, has enabled us to select and quantify adequately the variables and might be helpful in reducing clinical variability, improving the prognostic model and its predictive accuracy [25]. We have focused on a wide, heterogeneous patient population because SKIs are rare and diverse. On the other hand, other studies have focused on certain subgroups of patients [2,3,26], the presence or absence of an associated urologic abnormality [3,27], micro-organisms [28], microbial differences [29], the relation to specific treatments [1,12,26], or long-term outcomes [4,22]. Nevertheless, this prognostic model is accurate enough to be reproducible and validated in a group of patients separate from the population from which it was derived, with high predictive power. In addition, we consider our proposed scoring system to be user-friendly, easily distinguishing low-risk from high-risk patients and simply ascertaining the predictive variables in a timely and practical manner useful for a busy clinical practice. Finally, the prognostic estimate should actually influence subsequent treatment of the patient or improve modifiable conditions (e.g., choice of therapy and site of care).
The limitations of our study are several. First, we performed a retrospective observational study, so there may be some unmeasured covariates, and attempts to control for these differences cannot eliminate the possibility that patient groups may differ in ways that cannot be discerned. Second, the study involved a heterogeneous, unselected population of patients (e.g., ten patients with emphysematous pyelonephritis) with various combinations of different degrees of severity in a large number of cases of co-morbidity, with distinct prognoses, which may limit its predictive accuracy in particular subsets of individuals. In addition, for some variables, such as pathology types, there are no universally accepted classifications; in such cases, we had to form our criteria according to proposed severity of the infection course on the basis of both literature data and clinical experience. Hence, it may be preferable to identify the subgroups in which the prognosis can be improved by including additional variables. We have focused on early disease outcome because early treatment failure, not studied before in urologic infections, was associated with more complications (early recurrences and in-hospital death) and a longer stay in the hospital, as for a variety of common infectious diseases [8], which have their own prognostic models [9,25,30]. However, other clinical outcomes (e.g., death, quality of life, and cost) may be more important to patients and clinical decision makers and would be important end points worthy of study. Finally, this was a single-center, small prognostic study, which limits its generalizability.
Conclusion
A new weighted scoring system, based on a logistic function, was created to predict early treatment failure for a given patient with SKI. Although our system has good performance characteristics, and the data required by the predictive model can be obtained easily and provide a possible intervention measure, further studies in different settings and a large multi-center study should be performed before widespread implementation.
Footnotes
Acknowledgment
This study was conducted within the internal research project of basic research No. 09/09, Medical Faculty Kragujevac, Republic of Serbia.
Author Disclosure Statement
No conflicting financial interests exist.