
Abstract
Abstract
Background:
Invasive mucormycosis or aspergillosis is a life-threatening infection. The disease typically occurs in immunocompromised patients (e.g., those with diabetes mellitus or burns) but is rarely serious in otherwise-healthy young trauma patients.
Methods:
Case report and literature review.
Results:
A previously-healthy 22-year-old United States Marine who sustained large soft tissue injuries in support of Operation Enduring Freedom underwent multiple operations in theater to stabilize his wounds. He was evacuated first to Landstuhl Regional Medical Center in Germany and thence to the National Naval Medical Center in Maryland, where appropriate antifungal therapies were initiated and wide débridements were undertaken without success. His clinical status deteriorated, and he died. Tissue examination revealed systemic invasive mucormycosis and aspergillosis.
Conclusion:
The suspicion of invasive fungal infections must be tested early if intervention is to be curative.
Case Report
A 22-year-old United States Marine was wounded in Afghanistan in support of Operation Enduring Freedom after stepping on a buried pressure-plate mine while on dismounted patrol. He sustained catastrophic injuries, including traumatic right and left below-knee amputations, right inferior/superior open pubic ramus fractures, right open acetabular fracture, right sacroiliac disruption, perineal destruction with traumatic left orchiectomy, urethral transection, extraperitoneal bladder rupture, sigmoid colon transection, a right hand fracture and soft tissue injuries, left tympanic membrane perforation, and bilateral hemetympanum.
One hour after injury, he presented downrange to the Combat Support Hospital in cardiac arrest and recovered after a right thoracotomy and cardiac massage. His right leg was revised to a hip disarticulation, and negative pressure dressings were applied to his lower extremities and perineum. His abdomen was explored, and portions of the colon were resected and left in discontinuity. He was resuscitated with 34 units of packed red blood cells, 29 units of fresh frozen plasma, 4 six-packs of platelets, and three units of whole blood while in theater. The following day, he was evacuated to Landstuhl Regional Medical Center (LRMC), Landstuhl, Germany with an open abdomen.
While at LRMC, he underwent serial explorations of his abdomen as well as débridements of his lower extremities and pelvis. His massive muscular injuries led to rhabdomyolysis, causing acute kidney injury necessitating dialysis treatments. He was started on meropenem and amikacin for broad-spectrum coverage and doxycycline for routine anti-malarial prophylaxis.
For further definitive care, he was evacuated to the National Naval Medical Center (NNMC) five days after his injury. On arrival he was febrile, tachycardic, and normotensive. In the operating room, he was assessed and débrided by orthopedic, urology, and trauma surgery teams. Following surgery, the patient had a Glasgow Coma Scale score of 11 points and could answer simple yes/no questions. He was started on broad-spectrum antimicrobials including meropenem, vancomycin, and doxycycline (for malaria prophylaxis per routine) in addition to empiric initiation of fluconazole.
He was taken to the operating room every 48 h for wound exploration and débridement. Eventually, he underwent a revision of his left below-knee amputation, his abdomen was closed, his remaining testicle was removed, his right hip was revised to a hemi-pelvectomy, his left hand was pinned, a left posterior compartment fasciotomy disarticulation was performed, and his suprapubic tube was exchanged. He continued to require dialysis and received multiple transfusions of red blood cell concentrates and fresh frozen plasma. Clinically, he remained tachycardic into the range of >120 beats/min and was febrile intermittently with persistent leukocytosis. His neurologic status deteriorated steadily from a peak of 11 after his initial surgery at NNMC to non-responsiveness.
Nine days after his injury, blood cultures returned positive for Candida albicans, and his empiric fluconazole was changed to caspofungin. As part of his continuing evaluation, a non-contrast computed tomography image of his chest was obtained, which revealed bibasilar consolidation. Bronchoalveolar lavage was performed, revealing several areas of necrotic scar tissue in his trachea. A series of respiratory cultures were obtained and became positive for multiple types of mold, identified eventually as Aspergillus niger, A. terreus, A. flavus, and a mucor Cunninghamella species.
During the patient's second operative exploration, necrotic tissue consistent with previous blast injuries could be débrided back easily to viable tissue. However, by the third exploration, 15 days after injury, previously bleeding and healthy tissue was dusky with scant blood loss on transection. Tissue samples were sent for histopathologic examination. When the left leg posterior compartment fasciotomy was performed, the muscles that emerged were pink and healthy. However, within 48 h these, too, were necrotic. Similar necrosis was noted in his pelvis, anterior abdominal wall, and tissue flaps closed previously. Large lower-extremity vessels were transected during débridements with minimal or no bleeding.
Tissue examination of his right testicle, returned 15 days after his injury, revealed at least two species of fungus on routine, Grocott's methamine silver, and periodic acid-Schiff stains. These organisms appeared to be angio-invasive, with one of the species being consistent morphologically with mucormycosis. In addition, angio-invasive fungal organisms were noted from both his right rectus muscle and his right innominate bone. A tissue galactomannan assay was positive as well. Because of the overwhelming evidence of simultaneous invasive mucormycosis and aspergillosis, his anti-fungal regimen was changed to include both liposomal amphotericin B and enteric posaconazole, with a single loading dose of intravenous voriconazole. Of note, bacterial cultures of his innominate bone also yielded Stenotrophomonas maltophilia and Acinetobacter calcoaceticus-baumannii complex.
His wounds were too extensive for negative-pressure dressings to be re-applied, and thus were packed with gauze before he was transferred back to the intensive care unit. A meeting was held with his family, during which the patient's grim prognosis was discussed. The following morning, his dressings were removed at the bedside, and he was re-packed with Dakin solution-soaked gauze. He continued to deteriorate, necessitating the use of multiple vasopressors in addition to the aforementioned management. The decision was made to continue with comfort measures only. The patient died shortly after vasopressor support was halted.
Post-mortem examination revealed invasive mucormycosis and aspergillosis in many tissues, including the lung and pericardium. Examples are shown in Figures 1 and 2.

Mucor found on post-mortem examination. (
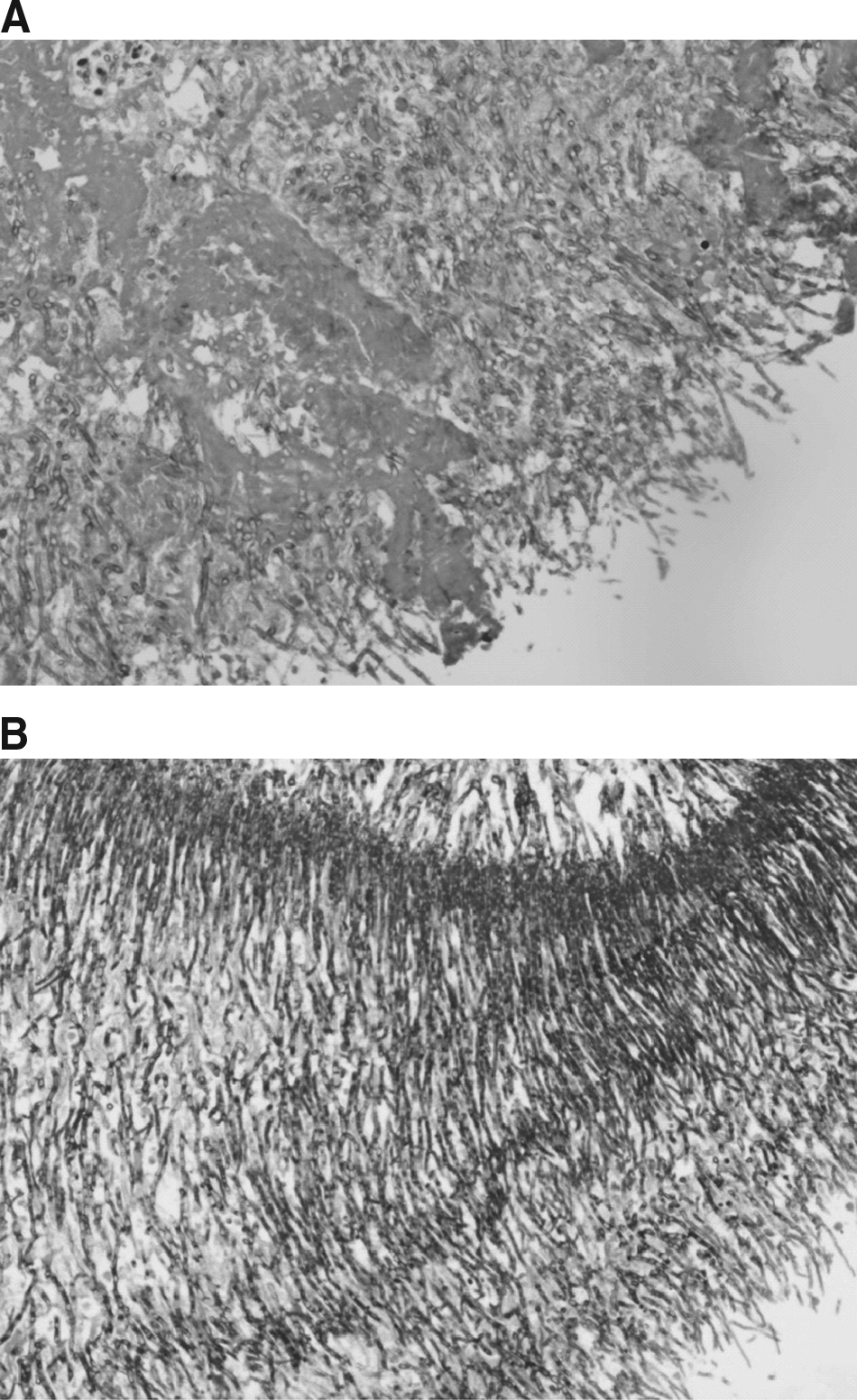
Aspergillus found on post-mortem examination.
Discussion
Invasive mucormycosis and aspergillosis have been described in trauma patients (primarily burn patients), but this patient's multiple fungal isolates, as well as the extent of dissemination, make this an unusual case. Generally, there is an underlying immunodeficiency in cases of invasive mucormycosis, whether that is from a baseline disease process such as diabetes mellitus or from an acquired source such as burns. However, cutaneous mucormycosis can result from direct spore inoculation of skin compromised by extensive trauma, even in immunocompetent individuals [1]. The mechanism through which this occurs is introduction of plant matter into wounds, as is observed commonly in farming injuries as well as in burns or massive abrasions in which the patient lies in soil [2–4]. Inoculation also has been described secondary to enterotomies in patients who had recently eaten food containing the offending fungus [5].
In addition to appropriate systemic anti-fungal therapy the optimal treatment for such an infection is wide débridement back to healthy tissue, which often includes amputation [6,7]. Anti-fungal agent selection was complicated in our patient by his multiple fungal isolates. Voriconazole is now recommended by the Infectious Diseases Society of America as the primary treatment for virtually all forms of invasive aspergillosis [8]. On the other hand, the various amphotericin B formulations remain the cornerstone of therapy for mucormycosis. Amphotericin B–based agents also are useful against Aspergillus isolates with the exception of A. terreus, which can demonstrate resistance and which our patient grew from respiratory cultures. In addition, oral posaconazole has been utilized as salvage therapy in patients with disseminated mucormycosis, although its role in primary therapy has not been established [9]. Of course, the key to effective treatment is early diagnosis. Given the rarity of this disease process, diagnosis often is delayed, to the detriment of the patient.
Among 11 trauma patients with invasive mucormycosis observed at The University of Texas Medical Center, none was found to have immunosuppression, although seven were in hypovolemic shock on admission, seven developed gangrenous cellulitis, and all received multiple blood transfusions and had open contaminated wounds. Four of these patients died from disseminated infection [7]. Mucormycotic necrotizing fasciitis was also described in a case series of 18 predominantly immunocompetent patients from India [10]. A larger review of the epidemiology of mucormycosis analyzed 929 cases, of which 176 had skin or soft tissue involvement. Penetrating trauma was present in 34% of the patients, with extension to tendon, muscle, or bone in 24%. Again, the majority of these patients had no underlying predisposing medical condition. Of the 35 patients with dissemination from skin to organ, 33 died, representing a 96% mortality rate. Interestingly, in the multivariable analysis both isolation of Cunninghamella species as well as the presence of renal failure were risk factors associated with a significantly higher mortality rate [11]. In another retrospective review, filamentous fungal infections carried a 25% mortality rate despite aggressive debridement and medical therapy. Patients with multiple trauma experienced a 46% mortality rate compared with 14% for those with single-extremity involvement [4].
Our patient was injured by a pressure-plated mine buried in the soil. The blast from this device provides an efficient vector for soil to penetrate deeply into tissue, as well as to produce possible inhalation injury and pulmonary inoculation. His extensive transfusions would also have depressed his immune system and left him susceptible to disseminated fungal disease. Ventilator dependency is another risk factor for immune dysfunction, and in combat environments, the ventilators themselves can be contaminated with soil, especially from rotary-engine aircraft during evacuations. Confusing this presentation and delaying the diagnosis of dissemination was our patient's apparent improvement after his initial two operations at our center. Unfortunately, the most important therapy, débridement, became untenable, as the diseased tissue extended into his proximal pelvis and the full thickness of his abdominal wall.
The mechanism of such extensive tissue necrosis is the angio-invasion of the fungal elements themselves. These mycotic thrombi effectively block the distal perforating vessels and eventually occlude the major vessels, as evidenced in our patient during his final débridement. With the antifungal medications unable to reach the distal tissues secondary to poor vascular supply, extensive necrosis followed, with resulting overwhelming invasion of the tissue [12].
In conclusion, this was a devastating injury to a previously healthy young man. The presence of both invasive mucormycosis and aspergillosis speaks to the vast insult to this patient's body and immune system. These infectious processes should be considered in the differential diagnosis of necrotizing skin and soft tissue processes in trauma patients regardless of their pre-injury immune status, especially in those with inoculation injuries and shock necessitating multiple blood transfusions. Early empiric treatment with azoles and amphotericin, while awaiting fungal culture results, should be considered in similar situations in the future. It also should be acknowledged that it was an incredible feat to move this patient from the battlefields of Afghanistan, through Germany, and to the United States to allow his family to spend his last days with him. This was attributable to the heroic efforts of the entire military medical system, including Navy, Army, and Air Force resources and personnel.
Footnotes
Author Disclosure Statement
No conflicting financial interests exist.
Acknowledgment
There was no financial support involved with this paper. We certify that all individuals who qualify as authors have been listed; each has participated in the conception and design of this work, the analysis of data (when applicable), the writing of the document, and the approval of the submission of this version; that the document represents valid work; that if we used information derived from another source, we obtained all necessary approvals to use it and made appropriate acknowledgements in the document; and that each takes public responsibility for it. Nothing in the presentation implies any Federal/DOD/DON endorsement.
We acknowledge Kristen Natale, DO for her assistance in procuring and photographing the excellent pathology slides included in this manuscript.