
Abstract
Abstract
Background:
Six hours from injury to washout is considered the gold standard in the treatment of open traumatic fractures. Despite this being our hospital policy, the rural nature of our Level I trauma center causes delays in discovery and transport, creating a unique randomization of time to washout. We hypothesized that orthopedic complications after open fractures are related to the severity of the fractures, not the timing of the washout.
Methods:
Patients and fractures were reviewed retrospectively over 6.3 years, evaluating for demographics, injury severity, location of fracture, mechanism of injury, Gustilo fracture grade, and time from injury to initial washout. Orthopedic wound complication rates were compared using logistic regression.
Results:
A total of 1,487 open fractures in 1,278 patients were reviewed. Time from injury to washout was 26 to 4,749 min (mean, 510 min), with 48 patients having no washout. Overall, 8.2% of fractures (n=122) had an orthopedic complication, rates of which increased with severity (Injury Severity Score, Abbreviated Injury Score [AIS], and Gustilo class) and blunt injuries but were not related to time to washout. Penetrating injuries showed no difference in complication rates according to time to washout. Lower extremity fractures had a higher rate of complications than those of the upper extremity (odds ratio 2.2), likely because of differences in fracture grade. By multivariable logistic regression, only fracture grade, Revised Trauma Score (RTS), and male gender were independent predictors of wound complications; penetrating trauma was predictive of low risk. Time to washout was not an independent predictor of wound complications.
Conclusions:
Although grossly contaminated fractures should not be left unattended, the degree of initial injury, as judged by fracture grade and physiology (RTS), was predictive of orthopedic wound complications, whereas time to washout was not. Hence, there is little benefit of washout in Gustilo grade 1/AIS 1 fractures or penetrating injuries, regardless of grade, and adherence to a specific time to washout is not beneficial.
Until the mid-19th Century, the treatment of open fractures was amputation; in 1842, this measure was proved to reduce the mortality rate [1]. It was only when Carl Reyher, in 1887, combined Lister's concept of antiseptic technique with Desault's concept of surgical debridement that a further reduction in the mortality rate was demonstrated [1]. After World War I, the military led the way in adopting washout, debridement, and withholding primary closure if 8 h had elapsed since injury. Only then did we as surgeons, both traumatologists and orthopedists, turn our attention to reducing infection and complication rates rather than accepting death and amputations. Six hours has been accepted as the maximum time from injury to washout on the basis of Friedrich's description of his experiments in 1898, in which he demonstrated 6 h to be the crucial time when bacteria replicate enough to be detected in guinea pigs [1]. Interestingly, there is a paucity of literature challenging this time-honored, nationally accepted standard.
Our Level I trauma center serves 29 counties with a combined population of approximately 1.5 million persons. Four metropolitan areas contain 17% of the population. Scene transport times average 1 h, whereas time from injury to definitive care with transfer from an outlying hospital averages 3.6 h [2]. Because of the rural nature of eastern North Carolina, we frequently observe gross contamination and substantial delays in time to discovery, presenting a unique environmental randomization of time from injury to washout. Additionally, as the only trauma center in the area, we have a high followup rate (95%; unpublished data), with essentially all patients with complications being referred to our center. With little data supporting the historical standard of 6 h, we reviewed, our experience in light of our unique environment. We hypothesized that there are no data to support the time to washout standard of 6 h.
Patients and Methods
Patient Selection
After obtaining approval from the Biomedical Institutional Review Board, the National Trauma Registry of the American College of Surgeons (NTRACS) was queried for a 6.3-year period (March 2000–July 2007) to identify all patients (aged 1.2 to 89.3 years) admitted to our rural Level I trauma center with an International Classification of Diseases (ICD), 9th Revision, Clinical Modification code for open fracture. Data in the NTRACS are entered prospectively during the patient's hospital stay. Abstracted from the database were demographics, injury severity using the Revised Trauma Score (RTS) and Abbreviated Injury Score (AIS), location of the open fracture(s), mechanism of injury (penetrating vs. blunt), Gustilo fracture grade, and time from injury to initial washout in minutes. Grade of fracture was assigned according to the Gustilo class regardless of the location of the fracture, although the Gustilo system is designed only for tibial fractures [3–5]. Paired broken bones at a single site were considered one fracture; for example, a fractured tibia and fibula at a single site with a single open wound was considered one fracture. However, a single bone counted as two fractures if there were two open wounds resulting from two separate fractures such as a proximal and a distal femoral fracture.
Time from injury to washout was designated from the time the injury was first documented (actual time of injury if known, time of ambulance dispatch, or time at initial outside hospital triage) to time of washout. Washout was defined as specific irrigation of the wound, typically in the operating room, although occasionally in the emergency department or intensive care bedside, as clinically indicated. Hence, the recorded time from injury to washout likely underestimates the true times. Washout was performed by either the orthopedist or the traumatologist, and use of antibiotic irrigant was a matter of personal preference. Our trauma center standards indicate that all open fractures are to be washed out within 6 h of arrival at our institution. Patients were excluded if their initial orthopedic injury management was started at another institution, if they were transferred from our center for completion of their orthopedic care, or if they died within one week of arrival, as orthopedic complications would not have had time to become manifest.
Orthopedic complications were defined as local cellulitis, wound infections, infections documented by delayed wound culture, osteomyelitis, non-union or malunion, and secondary amputation. Infections of primary amputation sites were included, whereas infections of pin sites remote from the wounds were excluded. Orthopedic injuries were collected on the basis of concurrent performance improvement (PI) tracking of all patients admitted or readmitted with a trauma-related ICD 9 code via the trauma PI database.
Statistical Analysis
Abstracted data are presented with appropriate descriptive statistics where available. Categorical data were analyzed using Pearson chi-square analysis or the Fisher exact test and scale/ordinal variables using the Student t-test or Mann-Whitney test where appropriate. All analyses were performed using PASW 17.0 (SPSS, Inc, Chicago, IL).
After univariable analysis, significant variables were selected for multivariable analysis of orthopedic complications using a forward stepwise logistic regression model. Significant alterations of the likelihood ratio (p<0.05) were used as entry criteria. Exit criteria were a change in the likelihood ratio with a p value>0.10. Goodness-of-fit and discriminatory ability were evaluated with Hosmer-Lemeshow chi-square and receiver operating characteristic (ROC) curves, respectively.
Results
During the 6.3-year period of the review, 1,357 patients with open orthopedic injuries were admitted to our trauma center. Sixty-seven patients (4.9%) were excluded because of death within one week, which did not allow time for orthopedic complications to develop. One of these patients died of pelvic sepsis from an open pelvic fracture with rectal injury; for the remaining 66 patients, the cause of death was not related to the orthopedic injuries. Five patients were excluded because of transfer for orthopedic/reimplantation care at another facility. Seven patients were excluded because their initial orthopedic care was provided at another institution prior to transfer to our facility. This resulted in a population of 1,278 patients (94.1% of the original series) with 1,487 open fractures (one to five per patient). The time from injury to washout was 26 to 4,749 min (mean 510 min), with 48 patients having no washout.
Overall, 8.2% of fractures (122) had an orthopedic complication. The majority of these were wound infections (98 fractures), with osteomyelitis (21 fractures) and non-union or malunion (12 fractures) being less common; some patients had more than one orthopedic complication. The majority of these complications were managed during the initial hospital admission; only 11 patients (0.9%) required readmission for further orthopedic care.
Orthopedic complications were more common with blunt injuries (Fig. 1), higher ISS, higher Gustilo grades (Fig. 2), and lower RTS. Male patients were more likely to have complications (Table 1). Time to washout was not different in the various groups according to univariable analysis. Lower extremity fractures had a higher rate of complications (odds ratio [OR] 2.1; p<0.001), likely because of their tendency to being of higher grade (Table 2). On multivariable regression analysis, only fracture grade, RTS, and male gender were independent predictors of wound complications; penetrating trauma was predictive of low risk (Table 3). Time to washout was not an independent predictor of wound complications (p=0.293).

Complications according to time to washout by injury mechanism. Time points are weighted by number of patients at that point.
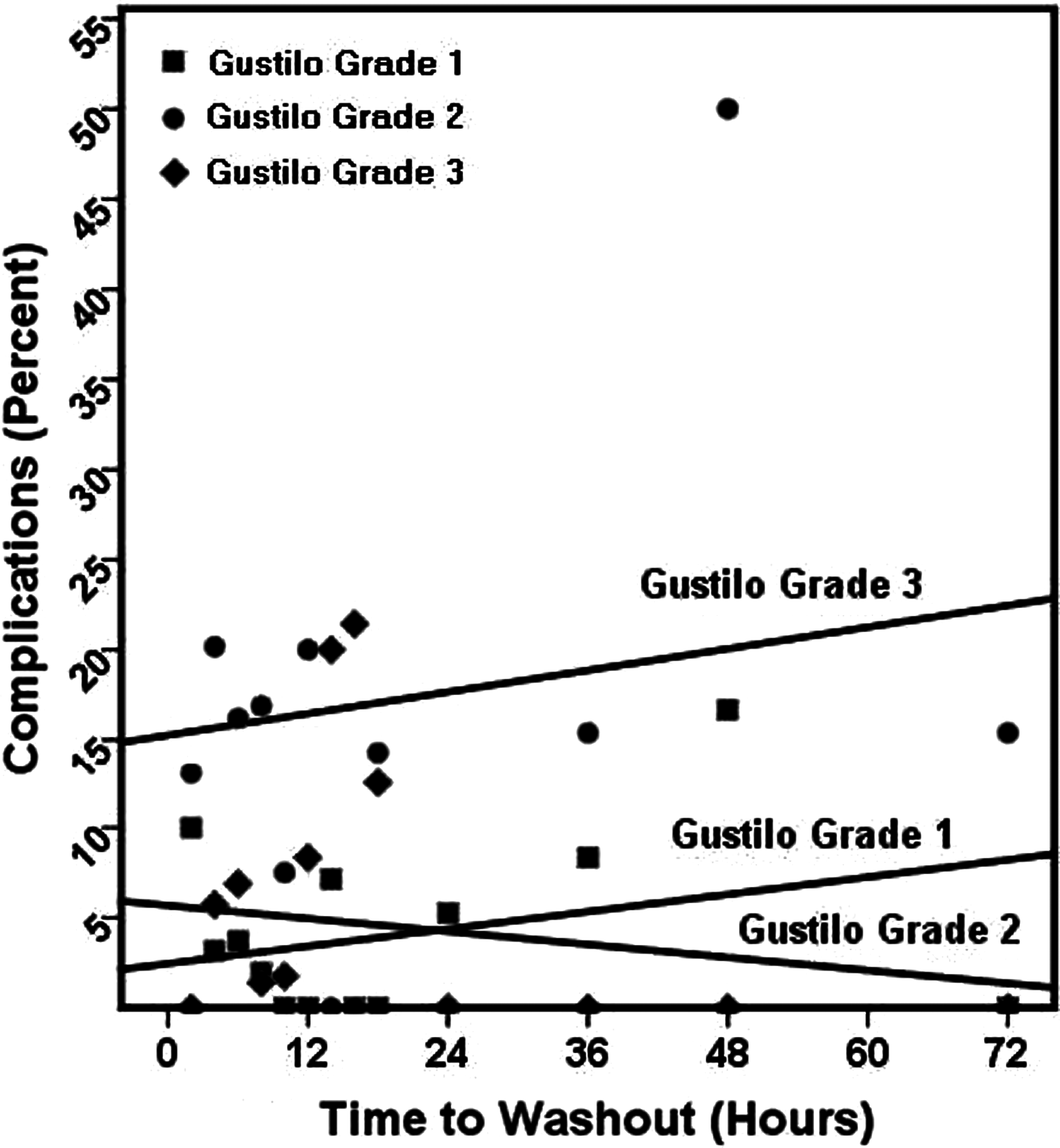
Complications according to time to washout by Gustilo grade. Time points are weighted by number of patients at that point.
Student t-test.
Mann-Whitney U test.
Fisher exact test.
Pearson χ2 analysis.
AIS=Abbreviated Injury Score, ISS=Injury Severity Score; RTS=Revised Trauma Score.
Hosmer and Lemeshow χ2 goodness-of-fit: p=0.890.
Receiver operating characteristic curve: 0.793 (95% confidence interval 0.751, 0.835).
Fifty-six primary amputations were required in 44 patients (about 6% of fractures). Thirty-six (64%) of these were finger or toe (minor) amputations, with 20 (36%) being major extremity amputations. No difference was noted between major and minor amputations by extremity site for primary amputations (major p=0.615; minor p=0.856). The primary major amputations were all in high Gustilo grade injuries—completion amputations or amputations for major crush and tissue loss. Eight patients developed an amputation site infection (included in the above infection data). Twenty-four delayed amputations (20 major; four minor) were required after failure of attempts to salvage the limb. The majority of these cases were Gustilo Class 3b fractures with a subsequent infection. No difference was noted in delayed amputation by extremity sites between major or minor amputations (major p=0.081; minor p=0.613).
Discussion
Our study examined a large and diverse population and indicates that time to washout has minimal effect on later orthopedic infections. Although this is not a new finding, nor is the fact that complications are related to Gustilo grade [6–11], we do present the largest patient and fracture population to date. Both injury severity and patient physiology are important predictors of complications, as determined in our regression analysis showing fracture grade and RTS to be predictors of negative outcome. Moreover, injury severity is most predictive of outcomes and is not mitigated significantly by early washout. Harley et al. in 2001 also reported this finding of the direct relation to injury severity to orthopedic complications in 215 patients [8]. Our study also indicates that washout in penetrating injuries has little to no effect. The finding of male sex as an independent predictor of wound complication is not so easily explained—this may be a statistical aberration attributable to a majority male trauma population, the propensity for male subjects to engage in high-risk activities and hence to present with more serious injuries and more deranged physiology not being captured by the RTS or Gustilo grade, a predilection for poor compliance with care, or a sex-based genetic and hormonal effect.
Although early surgical data indicated that washout should be accomplished without delay and that amputation rates were extremely high, care has changed dramatically in the last century. In 1989, Patzakis and Wilkins investigated factors influencing infections after open fractures. After conducting the largest review, covering 1,104 open fractures, they quoted an infection rate of 6.8% of fractures debrided and washed out within 12 h vs. 7.2% for those washed out after 12 h (χ2 analysis; p=0.879) [12]. At the Orthopedic Trauma Association in 2006, a tertiary-care center presented their case-controlled cohort study analyzing almost 900 open fractures over a 12-year period. The investigators demonstrated an overall infection rate of 11% with no difference between debridement at the 6-, 8-, 12-, 16-, or 24-h mark. High-energy and lower-extremity fractures had higher risks of complications, but when cases were matched for energy and extremity, the investigators were unable to show a higher risk of infection or non-union with delayed washout. Their logistic regression analysis of time to washout as a continuous variable did not show any higher risk of complications in either the matched or the unmatched case control groups [13]. Six other studies challenge the importance of time to debridement; each had fewer than 300 open fractures, and none demonstrated statistical support for the 6-h rule [6–11]. Additionally, our infection rate is consistent with those in similar studies (2%–20%).
Given the rural circumstances of our institution, we sought to clarify the optimal time to washout based on the grade of fracture. As the only Level I trauma center for a 29-county, rural area of eastern North Carolina, we are the major recipient of traumatically injured patients in our region. The trauma center serves a landmass of 13,735 square miles in Eastern North Carolina, with a population nearing 1.5 million. The population density for this area slightly exceeds 100 persons/square mile [2]. The state poverty level is 12%, but the eastern region has a 17% poverty level, thought to be worse because of isolation [14]. Ten counties have no hospital, and between 1974 and 2000, only 164 beds were added in the region with a net loss of three hospitals [15]. There are 155 emergency medical service (EMS) squads in this region, with more than one-third providing care only at the basic emergency medical technician level [2]. Because of the limited resources of our region, minimal care has been provided prior to arrival to our center. With the large and sparsely populated landmass we cover, long times between injury and arrival at our center are common, with delays in discovery, triage at outlying hospitals, and transport times. This has resulted in an essentially randomized time to washout, despite efforts to provide early care at our institution. It would be unethical to delay a patient's treatment on purpose in order to conduct a prospective study; thus, our randomization as a consequence of geography may be the closest to the ideal study.
Our outpatient followup rates exceed 95% (unpublished data), and, again, because of the rural nature of the region, few patients with complications seek care elsewhere. All patients readmitted to the hospital for further care of their injuries are captured by our PI system. Hence, few outpatient delayed complications are likely to have been missed by this review, excluding minor outpatient oral antibiotic-treated wounds.
The limitations of this study include the inability to account for variations in practice between the orthopedists or traumatologists. Some utilize antibiotic irrigation; some patients underwent serial washouts, placement of antibiotic beads, or both. Systemic antibiotics are standardized within the trauma service, but the few patients admitted directly to the orthopedic service or to a medical service may have had different regimes. Despite our fairly exclusive catchment area, some patients may have been seen elsewhere with complications, and a small part of our population is from other areas of the country and would have been followed up there.
Conclusions
Our data support those of prior smaller studies showing that time to washout has little direct effect in preventing orthopedic complications. Hence, resource utilization at trauma centers should be re-evaluated and directed toward the highest-risk patients. We recommend the following policy changes. Patients with penetrating trauma and low-grade fractures (Gustilo grades 1 and 2) do not require routine timed washouts. Patients with more severe fracture anatomy must be evaluated for other methods to mitigate their injuries, and rapid and aggressive control of abnormal physiology must be a first priority, certainly a higher priority than time to orthopedic washout. We must develop new methods to decrease orthopedic complications, as the historical standard of time to washout is no longer valid.
Footnotes
Author Disclosure Statement
No competing financial interests exist. No author has any financial disclosures to make.