
Abstract
Abstract
Background:
Hydatid disease is a parasitic infection that is endemic in Iran. It infests humans and herbivorous animals and reflects infection by Echinococcus granulosus. Although it can develop anywhere in the body, the liver and lungs are the most common sites of involvement. Primary muscular hydatidosis with no involvement of thoracoabdominal organs is a rare event.
Methods:
Case report and review of relevant literature.
Results:
We treated a 27-year old male patient with a swelling on his right shoulder that turned out to be a hydatid cyst by magnetic resonance imaging scan. The treatment included surgical excision combined with post-operative anthelminthic administration. Of the total reported cases of hydatidosis, 0.7–3% were described as musculoskeletal cysts.
Conclusions:
Especially in endemic areas, to avoid fine-needle biopsy and the risk of spillage of cyst contents irrespective of their location, hydatid disease should be considered in the differential diagnosis of muscular masses, and the diagnosis should be made by imaging and serology insofar as possible.
Case Report
A 27-year-old male farmer was referred from a rural medical center with an enlarging postero-lateral axillary mass beginning 1.5 years ago. The mass had enlarged gradually, and pain had developed in the last two months. He had no history of trauma, fever, chills, abdominal pain, weight loss, cough, hemoptysis, or respiratory distress. There was no drug ingestion history. A review of the family history showed no abnormal features.
On physical examination, a 10×5-cm non-mobile mass was noted in the right fourth–fifth intercostal space at the posterior axillary line with no evidence of inflammation, tenderness, or skin retraction. No regional lymphadenopathy was detected (Fig. 1A). The remainder of the physical examination was normal. Complete blood cell counts and serum biochemical parameters were all within normal ranges. By ultrasonography, a multi-septated cystic mass was observed in the right postero-lateral thoracic area with extension to the axilla. The liver, both kidneys, and the spleen were normal in size and shape. Magnetic resonance imaging (MRI) demonstrated multi-cystic changes within a well-defined mass (daughter cysts) occupying the right latissimus dorsi muscle (Fig. 2A).
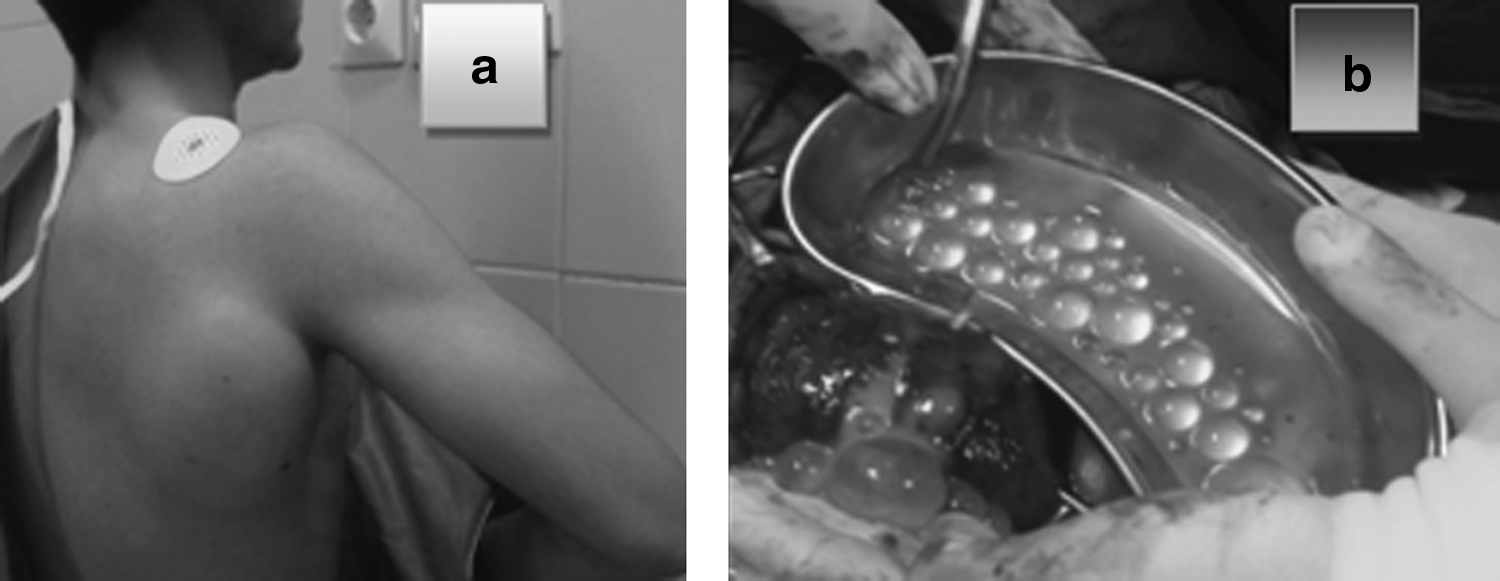
Photographs of patient. (
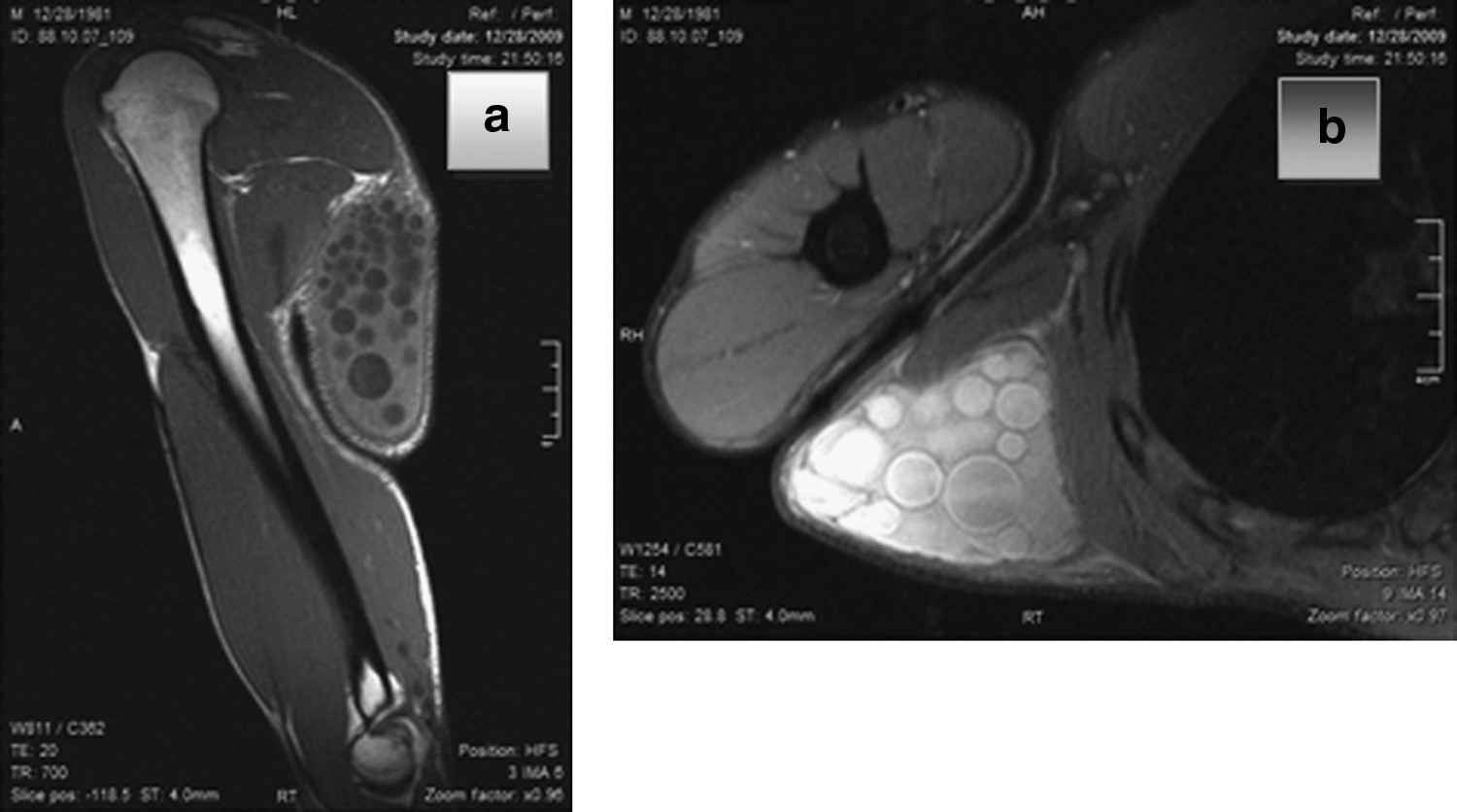
Magnetic resonance images of multi-vesicular lesions. (
The patient underwent surgery, and a horizontal incision was made over the mass. Before opening the cystic cavity, aspiration and scolicid injection was performed. Also, the surgical environment was packed away with a long scolicidal-soaked gauze before opening the cavity to prevent the spillage of scolices. Hypertonic saline was used as a scolicidal agent. The cyst was opened, all membranes and daughter cysts were removed, the cavity was irrigated with hypertonic saline, and a closed suction drain was inserted (Figs. 1B, 2B). The patient was maintained on albendazole at a dose of 600 mg twice a day for six months. Pathologic examination confirmed the diagnosis of hydatid cyst.
Discussion
Echinococcus granulosus is present in nearly all countries of the Middle East region. The reported incidence of infection ranges from 2–4 cases/100,000, with the highest rate of human infection in cattle-, camel-, and sheep-rearing countries [4].
Hydatid cysts resemble soft tissue tumors in their presentation in the shoulder region; therefore, this diagnosis has to be ruled out, both clinically and radiologically, prior to any invasive diagnostic intervention [4–6].
Ultrasonography demonstrates a thin or thick wall resembling a pericyst with internal echoes [7]. Treatment is best achieved by complete excision of the intact cyst following irrigation using cetramide, hypertonic saline, or hydrogen peroxide [4]. Although percutaneous treatment is considered as a viable alternative to surgery in patients with hydatid cysts in most of the organs of the body, such as the liver, lungs, kidney, orbit, and parotid gland, there is no study elucidating the results of percutaneous treatment of soft tissue hydatid cysts [8]. Adjuvant administration of albendazole (10 mg/kg twice a day) for as little as 2–3 mos after surgery may prevent local or distant dissemination, but medical treatment alone is not effective [9]. The treatment of soft tissue hydatid disease with albendazole does not reduce the size of the lesion, and surgical excision is still necessary [9].
Conclusion
When trying to determine the underlying cause of a rare location or an unexpected clinical presentation, hydatid cyst should be considered, especially in endemic regions and rural areas. An MRI scan is the best modality for making the definitive diagnosis, and when typical findings are present, needle aspiration/biopsy should be avoided.
Although some authors believe that percutaneous treatment is a safe and effective procedure with successful results in soft tissue hydatid cysts, surgical intervention is the appropriate treatment option for this type of cyst. Also, adjuvant administration of albendazole is recommended for six months after surgery.
Footnotes
Acknowledgment
The authors acknowledge gratefully the contribution of Ms. M. Hassanpour in editing and revising the manuscript. They have no financial conflicts in connection with this work.
Author Disclosure Statement
No conflicting financial interests exist.