
Abstract
Abstract
Background:
Primary cutaneous zygomycosis caused by Saksenaea vasiformis is rare. Such infections usually are not suspected, and delay in their diagnosis and treatment results in a poor outcome.
Methods:
Case report and review of the relevant English-language literature.
Results:
A fulminant cutaneous infection developing after intramuscular injection in the gluteal region of a 60-year-old female patient is described. The hallmark of this uncommon infection was the rapidity with which the skin and subcutaneous tissues of the right gluteal and lower abdominal regions underwent necrosis. The infection remained undiagnosed for nearly two weeks, leading to a fatal outcome.
Conclusion:
Awareness of the fact that fungi can also be the cause of cutaneous infections, as well as a high index of suspicion in patients who do not respond to conventional therapy, should help in the early diagnosis and management of such infections and may help in reducing the mortality rate.
Although candidiasis and aspergillosis are the fungal infections encountered commonly, zygomycosis, caused by fungi of the order Mucorales, may be seen at times. The order Mucorales contains genera such as Mucor, Rhizopus, Rhizomucor, Lichtheimia (formerly known as Absidia), Apophysomyces, Cunninghamella, Saksenaea, and Cokeromyces that usually cause human infections in six main clinical forms: Rhinocerebral, pulmonary, cutaneous, gastrointestinal, disseminated, and isolated renal [1,2].
Saksenaea vasiformis is one such rare pathogen belonging to the order Mucorales that has been implicated infrequently in the causation of cutaneous zygomycosis in human beings since it was first reported [3]. A search of available English-language literature revealed only 38 cases of S. vasiformis infections in human beings [4–16]; we report another such case with right-sided gluteal necrotic infection and stress the need for clinicians to be aware of such infections.
Case Report
A 60-year-old female presented to the surgical emergency department of our hospital with swelling, ulceration, and pain in the right gluteal region following an intramuscular multivitamin injection at that site one week previously. The swelling and ulceration had increased rapidly over this period to involve the lower part of the abdomen.
Clinical examination revealed a toxic-looking patient, with tachycardia, tachypnea, and pallor. Local examination of the right gluteal region revealed a large (10×10-cm) ulcerated, necrotic patch with surrounding cellulitis and induration extending onto the anterior abdominal wall. There was purulent discharge from the wound. Laboratory investigations revealed a hemoglobin concentration of 8.5 g/dL, a total leukocyte count of 20,600 cells/L−9, and marginally elevated blood urea and serum creatinine and normal blood glucose concentrations. Her human immunodeficiency virus status was negative. With a diagnosis of necrotizing fasciitis and sepsis, the patient was started on broad-spectrum antibiotics and taken for debridement under general anesthesia. The necrotic wound was debrided up to healthy margins, and the tissue was sent for histopathologic examination and bacterial cultures according to our routine.
She was managed on the ward by daily dressing changes and regular minor bedside debridements in addition to supportive care, and gradually became ambulatory. The culture from the specimen sent intra-operatively revealed Enterococcus faecalis sensitive to linezolid; therefore, that drug was started to control the bacterial infection. The histopathology report of the tissue sent after the initial debridement was received after one week, revealing zygomycosis. The patient therefore was taken for further debridement under general anesthesia to clear all unhealthy-looking tissues with wide margins.
Microbiologic examination was done as a potassium hydroxide wet mount and calcofluor white stain, which revealed sparsely septate broad hyphae with right-angle branching (Fig. 1). On histopathologic examination of the tissue, the same findings were corroborated by hematoxylin and eosin stain (Fig. 2) as well as Grocott methenamine silver staining. Fungal culture on Sabouraud dextrose agar and brain heart infusion agar grew white mycelial cottony material at 25°C as well at 37°C within 48 h. No spores could be induced. The isolate was later sent to the Mycology Reference Laboratory and Curator of the National Collection of Pathogenic Fungi, Bristol, UK, where the fungus was identified as S. vasiformis using molecular techniques.
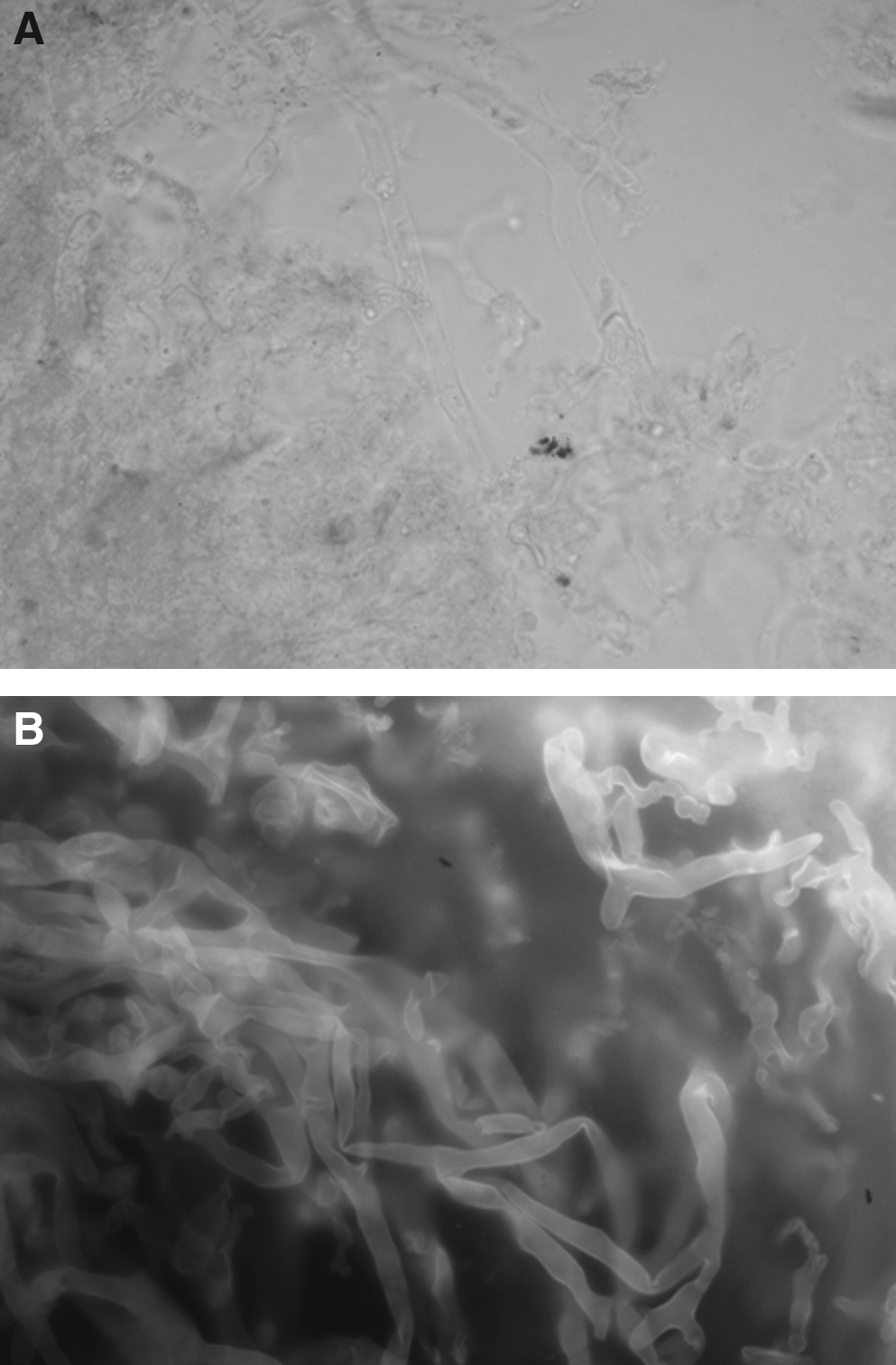
Causative fungus. (
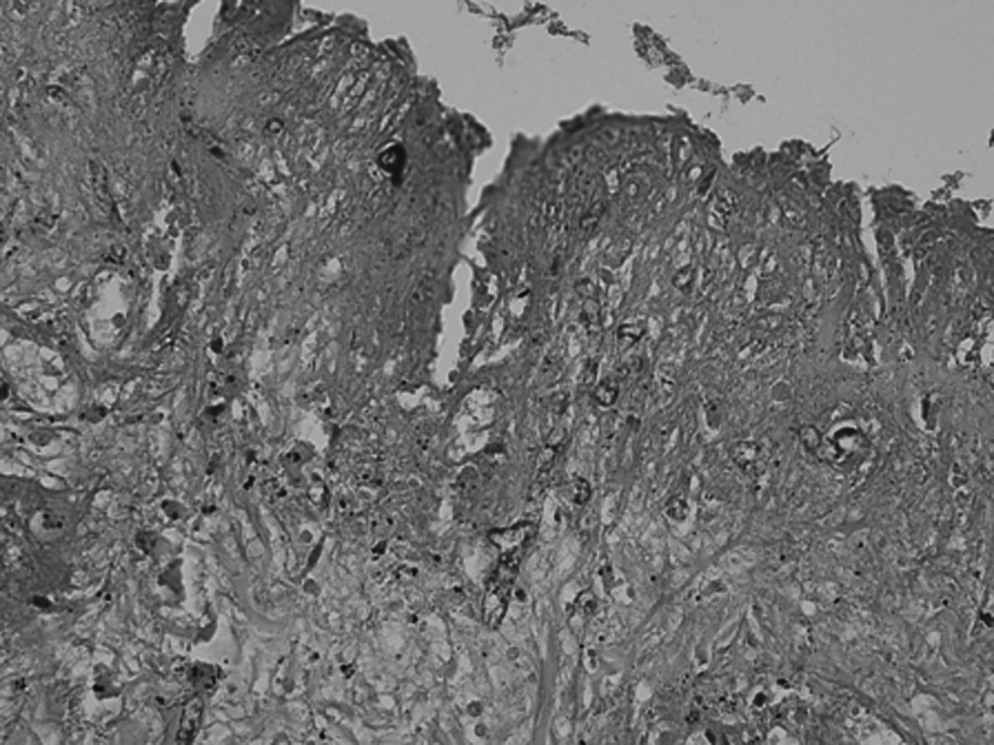
Histopathologic examination corroborating same findings by hematoxylin and eosin staining. (Original magnification ×400.)
With establishment of the diagnosis of cutaneous zygomycosis, injectable amphotericin B was added to the treatment schedule in incremental doses to reach a maximum of 0.6 mg/kg/day, with regular monitoring of renal function (particularly serum creatinine and potassium). However, after a cumulative dose of 485 mg, persisting hypokalemia and rising blood urea nitrogen and serum creatinine concentrations forced us first to change to an alternate-day schedule of amphotericin B and later to stop the drug completely. Although we kept on performing regular debridements, cessation of antifungal therapy led to further deterioration in the wound, as well as in the patient's general condition. She developedmultiple organ dysfunction syndrome and had to be shifted to the intensive care unit on ventilator support. As her condition deteriorated further, petechial hemorrhagic spots appeared all over the wound, and the infection spread deeper into the muscle planes (Fig. 3). The patient succumbed to her infection nearly one and one-half months after admission.

Deteriorating condition of wound, with petechial hemorrhagic spots and infection spreading deeper into the muscle planes.
Discussion
S. vasiformis was first isolated from forest soil in India and described by Dr. S. B. Saksena in 1953 [17], but since then, it has been reported from many other countries such as the United States, Australia, Central America, Iraq, and Israel [7, 18]. It is a ubiquitous fungus normally present in the environment but is a rare human pathogen, as it is unable to cause infection in the presence of an intact skin barrier. Thus, it tends to be pathogenic after trauma, burns, insertion of arterial lines, tattooing, surgery, or intramuscular injections [19–21]. In our patient, the fungus probably was implanted by a contaminated intramuscular injection, leading to the development of necrotizing cutaneous infection that remained unrecognized and untreated for nearly two weeks, resulting in a fatal outcome.
Although the first human infection with this organism was reported by Ajello et al. in 1976 [3], only 38 cases have been documented in the English-language literature since [4–16]. Of these, only 12, excluding the present report, were published in the years from 2000 through 2010 (Table 1) [5–16]. The low recent incidence may not reflect the actual burden of the disease but rather: (1) Lack of awareness of this clinical entity; (2) the high mortality rate of untreated or inadequately treated cases; (3) tissues not being sent routinely for histopathologic examination and fungal cultures in most places; (4) difficulty in inducing sporulation in cases of S. vasiformis infections that may have led to such cases being identified simply as zygomycosis; (5) clinical bias, in which isolation of secondary bacteria on routine cultures has led the clinician away from the actual diagnosis of zygomycosis; and (6) microbiological bias, where the fungus may be discarded as a contaminant rather than taken seriously as the cause of infection.
AMB=amphotericin B; LAMB=liposomal amphotericin B.
A high index of suspicion, early diagnosis, and treatment by amphotericin B and surgery are the cornerstones of managing such infections [21]. Clinically, the infection can be superficial or deep and can appear in the form of pustules, blisters, nodules, necrotic ulcerations, ecthyma gangrenosum-like lesions, or necrotizing cellulitis. The appearance of blackish eschar-like tissue or “cheesy” whitish material within the wound or a rapidly progressing wound that does not respond to conventional antibiotic therapy should alert the clinician to the possibility of cutaneous zygomycosis [1,21,22].
Histopathologic confirmation is essential once the diagnosis is suspected on clinical grounds [21,23]. The hallmark of zygomycosis is extensive cellular and vascular invasion resulting in thrombosis and tissue infarction/necrosis [21,24]. In most cases, there is a narrow zone of polymorphonuclear leukocytes surrounding the fungal hyphae within the necrotic tissues [20]. Fungal cultures and routine stains of the wound by themselves are not sensitive and may give false and misleading results, even among patients with histologically proved infection (the viability of the fungus may be damaged inadvertently during processing, it may be discarded as a contaminant, or it may fail to grow and sporulate) [23]. As the present report highlights, delay in diagnosis can have a fatal outcome, and therefore, it is recommended that the tissues be subjected to frozen section analysis in suspicious cases [18] to obtain an early diagnosis rather than waiting for the routine histopathology report, which can be delayed.
Amphotericin B remains the drug of choice for the treatment of zygomycosis, as these fungi are resistant to many of the other antifungal drugs available. Although posaconazole has shown efficacy against these fungi (alone or in combination with amphotericin B), it is well established that voriconazole, despite having wide therapeutic activity, is not effective in infections by zygomycetes [25,26]. It is recommended to administer amphotericin B in incremental doses to reach a maximum daily dose of 0.5 to 0.75 mg/kg in order to reduce the chances of side effects. Some authors recommend even higher doses (1 to 1.5 mg/kg/day) [21], but this can cause renal toxicity. Although liposomal amphotericin B is less nephrotoxic than amphotericin B deoxycholate, we were unable to use this preparation in the treatment of the present case because of its prohibitive cost; this is an important factor in determining drug prescriptions in our institution, as many of the patients are unable to afford expensive therapy. The inability to afford liposomal amphotericin B prohibited adequate antifungal therapy in our patient and contributed to the fatal outcome.
Aggressive surgical debridement also is important, as antifungal therapy alone is inadequate to control the infection. Repeated debridements may be necessary to achieve control. Necrotic tissue acts as a barrier to the penetration of amphotericin B to the site of infection [22], and surgery removes that barrier. Such tissue can form a nidus for secondary infection and act as a source of continuing sepsis. In patients in whom there is involvement of a limb, amputation may become inevitable. The mortality rate of untreated cases is almost 100%, but patients with cutaneous disease who undergo aggressive debridements and adequate antifungal therapy have a mortality rate only of around 10% [1,21].
Footnotes
Acknowledgments
The authors are thankful to Dr. Elizabeth M. Johnson, Director, Mycology Reference Laboratory and Curator of the National Collection of Pathogenic Fungi, Myrtle Road, Kingsdown, Bristol, United Kingdom, for finally identifying the fungal isolate.
None of the authors has any commercial association that might create a conflict of interest in connection with this manuscript.
Author Disclosure Statement
No conflicting financial interests exist.