
Abstract
Abstract
Background
: We defined the contemporary conversion rate from laparoscopic appendectomy (LA) to open appendectomy and identified pre-operative factors associated with conversion.
Methods
: Retrospective review of 941 consecutive LAs performed for suspected acute appendicitis in a single urban university hospital between 2000 and 2007. Patient characteristics, clinical features, physical examination findings, laboratory values, computed tomography (CT) findings, surgeon identity, operative findings, and pathologic results were assessed. Categorical variables were compared in patients undergoing LA and those in whom conversion was necessary using the Fisher exact test; the Student t-test was used to compare continuous variables. Multivariable analysis was performed with binomial logistic regression. Statistical significance was established at α = 0.05
Results
: The overall conversion rate was 4.1% and did not change significantly over the course of the study. By univariable analysis, conversion was significantly associated with older age, male gender, American Society of Anesthesiologists (ASA) score >2 points, longer duration of symptoms, rigidity on physical examination, increased percentage of neutrophils on admission white blood cell differential count, extraluminal air on CT, inexperience of the attending surgeon with LA, retrocecal location of the appendix, gross necrosis or perforation, murky or purulent ascites, and microscopic evidence of perforation. By multivariable analysis, advanced age (hazard ratio [HR] 1.02 per year; 95% confidence interval [CI] 1.01–1.04, p = 0.02), ASA score >2 points (HR 11.2; 95% CI 5.6–24.4; p < 0.001), CT inflammation grade ≥4 (HR 4.8; 95% CI 1.9–12.3; p = 0.001), and attending surgeon inexperience (HR 7.4; 95% CI 2.6–20.8; p < 0.001) were independent predictors of conversion.
Conclusion
: The conversion rate during laparoscopic appendectomy has not changed significantly over the past seven years and remains ∼4%. Independent pre-operative predictors of conversion are advanced age, ASA score >2 points, attending surgeon inexperience, and extensive inflammation observed on pre-operative CT scan. Proceeding directly with open appendectomy under these circumstances may reduce operative time, expense, and morbidity.
Previous reports indicated that the decision to convert to an open procedure during LA usually is prompted by factors discovered intraoperatively, including a retrocecal appendix, adhesions, presence of an abscess, or inflammation or necrosis of the base of the appendix [6,7]. However, pre-operative factors may be associated with conversion, and previous studies have documented an association of conversion with age ≥65 years, diffuse tenderness on physical examination, surgeon inexperience, and severity of the findings at computed tomography (CT) [7]. Conversion to open appendectomy has been associated with longer operating times, longer hospital stays, and a higher rate of intra-abdominal abscess [6–8].
We have described recent trends in the treatment of acute appendicitis at our institution, including the increase in the utilization of LA and CT to >90% of patients [9–11]. The purpose of this study was to examine the rate of conversion of LA to open appendectomy in a single institution during an era of near-universal adoption of the laparoscopic technique, and to identify pre-operative factors that predict conversion to an open procedure. We hypothesized that factors available to the surgeon prior to operation could be utilized to identify patients at high risk of conversion to an open appendectomy in whom an open procedure might be the better first choice.
Patients and Methods
We analyzed retrospectively all patients undergoing appendectomy for suspicion of acute appendicitis at the New York-Presbyterian Hospital/Weill Cornell Medical Center between January 2000 and March 2007 after obtaining approval from our Institutional Review Board (IRB), the Committee on Human Rights in Research of Weill Cornell Medical College. This cohort of 1,425 patients has been described previously [9], and 941 of these patients who were confirmed to have undergone LA or converted open appendectomy comprise the present study group. In accordance with the Health Insurance Portability and Accountability Act (HIPAA) and the policies of the IRB, patient consent was waived. Patients were identified initially using pathology records to locate appendectomy specimens received during the study period; those undergoing interval appendectomy or surgery for reasons other than suspicion of acute appendicitis were excluded.
Clinical characteristics were obtained via chart review. Baseline factors recorded for each patient were age, sex, American Society of Anesthesiologists (ASA) physical status score, and body mass index (BMI). Presenting signs and symptoms analyzed included the duration of symptoms at the time of presentation (rounded to the nearest half day); the presence, location, and characteristics of abdominal pain; history of nausea, vomiting, fever, or anorexia; physical findings of temperature, location of tenderness, presence of signs of peritonitis (i.e., abdominal rigidity, involuntary guarding, rebound tenderness); and palpable right lower-quadrant mass. Laboratory data obtained included the white blood cell count and differential proportion of neutrophils. Computed tomography (CT) reports were reviewed for the presence of appendiceal dilation, fluid-filled appendix, wall thickening or enhancement, ascites, abscess, phlegmon, periappendiceal fat stranding, extraluminal air, and appendicolith. A published system devised to assess the severity of appendicitis was applied having a scale from 0 to 5 as follows: 0 = normal appendix; 1 = possibly abnormal appendix; 2 = abnormal appendix (diameter of at least 6 mm with contrast enhancement but no peri-appendiceal fat stranding); 3 = abnormal appendix with peri-appendiceal fat stranding; 4 = abnormal appendix with peri-appendiceal fat stranding and fluid; 5 = inflammatory mass (phlegmon) or abscess [7,12].
Operative reports were reviewed to verify the identity of the attending surgeon, the method of appendectomy, the operative findings, and the reason for any open conversion. Operative findings of interest included perforation, retrocecal position of the appendix, appearance of the appendix (i.e., normal, inflamed, suppurated, or necrotic/gangrenous), and the presence or appearance of ascites (i.e., none, serous, turbid/purulent). The pathology report for each specimen was reviewed to classify the diagnosis as positive or negative for appendicitis and verify the presence or absence of histologic evidence of perforation.
Development of post-operative abscess was detected by reviewing daily progress notes, follow-up clinic notes and emergency room visits, or re-admissions within 30 days of appendectomy. Suspicion of post-operative abscess was confirmed by CT scan.
Continuous variables were compared using the Student t-test (SPSS version 17.0, SPSS Inc., Chicago, IL). Differences in categorical variables were compared using the χ2 test unless expected cell counts were <5, in which case, the Fisher exact test was used.
Multivariable logistic regression models were created to evaluate the independent association of pre-operative factors with conversion to open appendectomy. Variables associated with conversion at p < 0.05 by univariable analysis were added to the model using a forward selection method. Model fit was assessed using the Hosmer-Lemeshow goodness-of-fit statistic, with p > 0.05 indicating acceptable model calibration. Statistical significance was set at α = 0.05.
Results
During the study period, 941 patients underwent attempted LA. Conversion to an open procedure occurred in 39 cases (4.1%). During individual years of the study, the conversion rate ranged from 3.4%–5.5% and did not differ significantly by year (χ2 = 1.0; p = 0.99). The most common reasons for conversion were dense inflammatory adhesions (n = 9), inability to see the appendix or its base clearly (n = 9), inflammatory involvement of the base of the appendix or cecum (n = 6), or gross perforation (n = 4). Less commonly, the grounds for conversion were a suspected mass (n = 3), a suspected or confirmed bowel injury (n = 3), a retrocecal appendix (n = 2), patient intolerance of the Trendelenburg position (n = 1), or diffuse peritonitis (n = 1). In one case, equipment malfunction prevented completion of the procedure laparoscopically.
The baseline characteristics of the study population are presented in Table 1. Patients requiring conversion to open appendectomy had a significantly higher mean age (53 ± 18 vs. 39 ± 18 years; p < 0.0001), were more likely to be male (64% vs. 47%; p = 0.04), and more likely to have an ASA score >2 points (30% vs. 5%; p < 0.01). No difference in conversion rate was noted according to the BMI.
ASA = American Society of Anesthesiologists physical status score; SD = standard deviation; WBC = white blood cell count.
Among elements of the history and physical examination on presentation, only the duration of symptoms was associated with conversion (Table 1). The mean duration of symptoms in patients undergoing conversion was significantly longer than that in the group whose operations were completed laparoscopically (2.1 ± 2.1 vs. 1.4 ± 1.0 days; p < 0.0001). Whereas the conversion rate among patients with less than one day of symptoms was 2.3%, it was 4%–5% in patients with one or two days' duration and 9%–10% for patients with three or more days of symptoms (Fig. 1). A history of nausea, vomiting, anorexia, or fever was not associated with a higher rate of conversion. No physical finding predicted conversion. Whereas the white blood cell count on admission did not differ between the groups, the mean proportion of neutrophils was higher in the converted group (83 ± 10% vs. 79 ± 11%; p = 0.03).
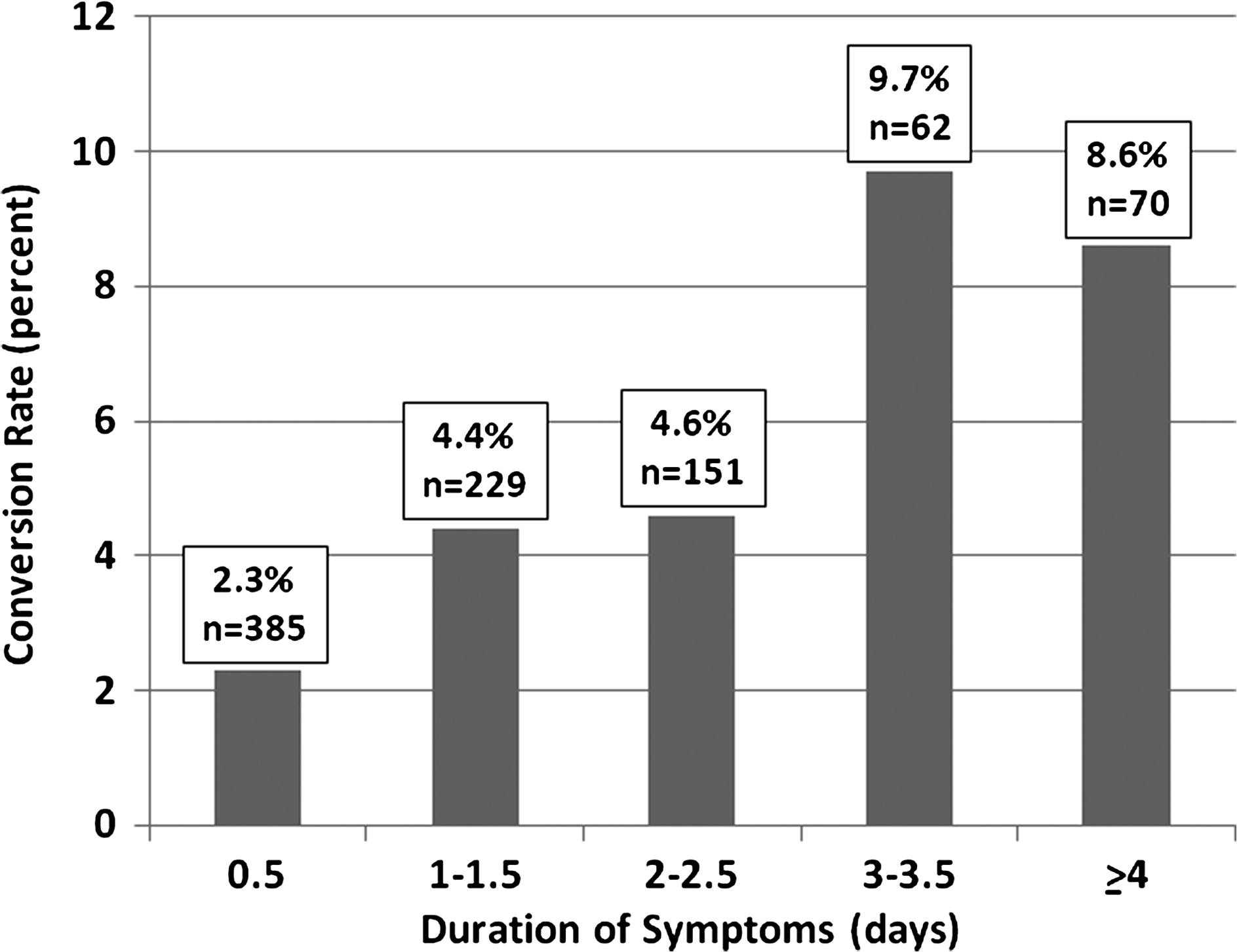
Conversion rate during laparoscopic appendectomy by duration of symptoms.
Computed tomography findings are listed in Table 2. The only isolated CT finding associated significantly with conversion was pneumoperitoneum, which was present in 20% of converted cases compared with 2% of the cases completed laparoscopically (p = 0.001). However, when the degree of inflammation on CT was scored, as has been described previously [7], a grade of at least 4 of 5, indicating the presence of an abscess, a phlegmon, or fat stranding with ascites, was present in 55% of cases necessitating conversion, compared with 26% of those completed laparoscopically (p = 0.008).
Defined by Siewert et al. [12] as an abnormal appendix in association with a phlegmon or a combination of inflammatory stranding plus ascites.
Attending surgeon identity and operative findings were related closely to the need for conversion (Table 3). The conversion rate among surgeons who performed fewer than 20 LAs over the course of the study was nearly three times the rate among surgeons performing the procedure more commonly (8.9% vs. 3.2%; p = 0.003). Retrocecal appendix location (p = 0.02), appendiceal necrosis (p < 0.0001), perforation (p < 0.0001), and purulent ascites (p < 0.0001) all were significantly associated with conversion. Likewise, histologic evidence of perforation was more likely in converted cases than in LA cases (28.2% vs. 4.4%; p < 0.0001), whereas acute appendicitis was present in most members of both groups.
An intra-abdominal abscess developed in two patients (5.1%) undergoing conversion to open appendectomy. This was not significantly different from the rate among patients undergoing either laparoscopic (4.7%; p = 0.4) or open (2.7%; p = 0.3) procedures during the study period.
To identify factors available to the surgeon prior to operation that independently predicted conversion to open appendectomy, multivariable analysis was performed (Table 4). Advanced age, ASA score >2 points, CT inflammation score ≥4, and attending surgeon inexperience were significantly and independently associated with conversion to open appendectomy.
χ2 = 638; p < 0.0001; Hosmer-Lemeshow p = 0.91.
LR = likelihood ratio.
Discussion
The decision to convert an LA to an open procedure is complex, involving patient factors, anatomic variables, and the severity of inflammation secondary to appendicitis, as well as surgeon skill and comfort with laparoscopic surgery in the setting of inflamed or gangrenous tissue. Whereas some degree of subjectivity will always be present in deciding when to convert, understanding objective factors that make conversion more likely could help identify patients who may benefit from proceeding directly with open surgery. This practice could reduce operative time and expense, as well as the potential for complications incurred during a futile laparoscopic dissection. In order to facilitate proper selection of patients for laparoscopic appendectomy, it is important to identify factors knowable pre-operatively that predict the likelihood of a successful LA.
In our population of 902 patients undergoing LA, conversion to an open procedure occurred in 39 cases (4.1%). In a meta-analysis of 54 randomized controlled trials comparing LA with open appendectomy, the conversion rate was approximately 10% [13]. Several factors are likely to account for the lower rate in our series, most notably, a selection bias such that some patients in our retrospective study who were believed likely to require open appendectomy may never have undergone an attempt at laparoscopy. Also, many of the studies included in the meta-analysis were performed in the early years after introduction of LA when usage was demonstrably lower [14], and thus, a learning curve effect may have contributed to a higher conversion rate. In fact, the conversion rate in studies completed prior to 1995 was >10%, whereas in all subsequent time periods, the rate was 7%–8% when one excludes a large outlier series with a conversion rate of 23% [13,15].
By univariable analysis, a number of risk factors for conversion to open appendectomy were identified. These included advanced age, male sex, ASA score >2 points, symptom duration of three or more days, higher percentage of neutrophils on white blood cell differential count, severity of inflammation as graded by CT scan, surgeon inexperience, retrocecal location of appendix, appendiceal necrosis or perforation, and purulent ascites. Multivariable analysis incorporating those factors available to the surgeon pre-operatively identified advanced age, ASA score >2 points, severity of inflammation on CT, and attending surgeon inexperience as being independently and significantly associated with conversion. These results highlight the complex nature of the decision to convert, inasmuch as baseline patient characteristics, disease severity, and surgeon factors each independently impact the probability of a successful laparoscopic procedure. Notably, as LA approaches universal adoption, the effect of surgeon inexperience with this procedure, now performed commonly during surgical training, would be expected to diminish. It is interesting that although on univariable analysis, increasing duration of symptoms was significantly associated with the probability of conversion (Fig. 1), this factor was not independently associated with unsuccessful laparoscopic appendectomy on multivariable analysis. Presumably, this reflects the fact that although a longer duration of symptoms is associated with a greater degree of inflammation, it is not a predictor of conversion in and of itself. Thus, in our model, radiologic assessment of the severity of inflammation on CT scan was superior to duration of symptoms as an indicator of the likelihood of conversion.
Our results are largely in agreement with those of prior studies on this topic. Liu et al. examined a series of 705 consecutive LAs, 58 of which were converted to open operations. Independent risk factors for conversion were age ≥65 years, diffuse tenderness on physical examination, surgeon inexperience, and severity of inflammation as graded by CT [7]. They utilized these four factors to stratify patients into risk groups for conversion, such that patients with no risk factors had a ∼5% chance of conversion, whereas patients with one, two, or three factors had a probability of conversion of ∼15%–40%, ∼40%–80%, or >80%, respectively. When applied to our population of patients, significant differences in the rate of conversion were found (p < 0.0001), although the overall risk was much lower than that expected on the basis of the report by Liu et al. Of 273 patients in our cohort with no risk factors, there were 2 conversions (0.7%), whereas the conversion rate in patients with one or two risk factors was 4%–6%. A small group of seven patients with three risk factors saw two conversions (29%). These authors, in a separate report on radiologic (CT) findings in patients requiring conversion to open appendectomy, examined appendix location and diameter, the presence of appendicoliths, cecal wall thickening at the appendiceal base, and lymphadenopathy as potential predictors of conversion [12]. Although none of these findings in isolation was a satisfactory predictor, use of a multifactorial six-point scale of radiologic severity of inflammation identified patients with severe inflammation (Grade 4 or 5) as at higher risk for conversion. Thus, patients who had CT findings of an abnormal appendix in association with an abscess, a phlegmon, or a combination of inflammatory stranding plus ascites had a three-fold higher probability of open conversion (21% vs. 7%; p < 0.04). This significant difference was corroborated in our cohort, although the conversion rates were substantially lower (Grade 4–5, 6.8% vs. Grade 0–3, 2.1%; p = 0.008).
Similarly, Hellberg et al. analyzed the factors associated with conversion in a series of patients undergoing LA as part of a randomized trial [6]. In this series, male gender, high BMI, elevated blood C-reactive protein concentration, and perforation of the appendix were associated with conversion (p = 0.05), and advanced age trended toward statistical significance (p = 0.06). In our series, whereas male gender and appendiceal perforation were associated with conversion, elevated BMI did not predispose a patient to conversion. In our institution, C-reactive protein is not measured routinely during the workup of acute abdominal pain.
The importance of recognizing patients at high likelihood of requiring conversion to open appendectomy is two-fold. First, if conversion is necessary, the patient has been exposed to the risks of laparoscopy (including prolonged operating times and pneumoperitoneum) and its higher associated hospital cost without receiving the purported benefits of smaller incisions, decreased pain, shorter hospital stay, and earlier return to work and normal activity [13]. These theoretical concerns were borne out in the report by Hellberg et al. Patients randomized to LA and subsequently converted to open surgery experienced longer operating times (83 min vs. 35 min; p < 0.001) and hospital stays (4.5 days vs. 2 days; p < 0.001) than patients randomized to open appendectomy [6]. Second, the morbidity of a converted procedure may be higher than that of an open procedure. Although no prospective data are available to address this question, Piskun et al., in a retrospective analysis of patients treated for complicated appendicitis, found an intra-abdominal abscess rate of 50% among 10 patients whose procedure was converted to open appendectomy, compared with 28% in 18 patients undergoing successful LA and 29% in 24 patients initially selected for open surgery [8]. In our series, no difference was observed in the rate of post-operative intra-abdominal abscess according to the method of appendectomy.
In summary, we identified a triad of pre-operative factors that predict conversion during LA, consisting of old age or infirmity, severe inflammation, and surgeon inexperience. Surgeons, especially those less experienced with LA, should consider proceeding directly with open appendectomy in patients meeting these criteria. Attempting laparoscopy under these circumstances commits a patient to a longer operating time and higher hospital cost, while possibly sacrificing the putative benefits of LA, namely, reduced pain and earlier discharge and return to normal function.
Footnotes
Author Disclosure Statement
None of the authors has direct or indirect financial or personal relationships, interests, or affiliations relevant to the subject matter of this manuscript.