
Abstract
Abstract
Background:
Complicated intra-abdominal infections (cIAI) are a common problem in surgical practice. The effect of body mass index (BMI) on the outcome is poorly understood. We compared the association of BMI and type of antibiotic therapy for cIAI described in a previously published trial of ertapenem vs. piperacillin-tazobactam (Namias N, Solomkin JS, Jensen EH, et al. Randomized, multicenter, double-blind study of efficacy, safety, and tolerability of intravenous ertapenem versus piperacillin/tazobactam in treatment of complicated intra-abdominal infections in hospitalized adults. Surg Infect 2007;8:15–28).
Methods:
A post-hoc analysis was performed using data obtained from the published study. The effect of BMI and type of antibiotic used for therapy were calculated for clinically favorable outcomes at early follow-up assessment (EFA).
Results:
The 231 patients who were microbiologically evaluable at EFA were stratified by BMI (<30 or ≥30 kg/m2). Twelve patients were excluded because of missing BMI data, leaving 219 patients for analysis. There were some differences in baseline characteristics between patients with a BMI <30 kg/m2, including the source of intra-abdominal infection (more appendicitis in BMI <30 group; p=0.01) and gender (more men in the BMI <30 group; p=0.03). There was no difference in cure rates between the groups (82.9% for BMI <30 kg/m2 vs. 74.5% for those with BMI ≥30 kg/m2; 8% difference in proportions, 95% confidence interval [CI] −5%, 25%). There was an 80% favorable clinical response to ertapenem in the BMI <30 group compared with an 81% favorable rate in the BMI ≥30 group (−1% difference in proportions; 95% CI −22%, 19%). This compared with an 86% favorable response rate to piperacillin-tazobactam in the BMI <30 group vs. a 65% favorable clinical response rate in the BMI ≥30 group (21% difference in proportions; 95% CI −1%, 47%).
Conclusions:
There was no difference in the cure rate of patients with cIAI in the BMI <30 and BMI ≥30 kg/m2 groups. There were no statistically significant differences in the likelihood of response to an antibiotic regimen. However, there was a nominally 21% lower cure rate in the high BMI group receiving piperacillin-tazobactam (86% vs. 65%; 21% difference in proportions; 95% CI −1%, 47%), whereas there was only a 1% difference in the cure rate between BMI groups in the patients receiving ertapenem. This difference may be related to gender and etiology of infection. Although limited by the small number of high BMI patients and post-hoc methodology, these results merit consideration of the design of future prospective antibiotic trials to include stratification for BMI and consideration of the effect of BMI on pharmacokinetics and pharmacodynamics.
Differences in the health management of obesity should include an understanding of the pharmacokinetics of certain antibiotics used for common or life-threatening infections, such as complicated intra-abdominal infections (cIAIs). These infections are those that necessitate operative interventions or percutaneous drainage for initial source control. They may result in substantial morbidity or death for patients of any BMI. Together with adequate source control, antibiotics are the mainstay of therapy for these polymicrobial infections caused by gram-positive, gram-negative aerobic, or anaerobic organisms [5].
An earlier randomized controlled trial compared the effectiveness of ertapenem with that of piperacillin-tazobactam in treating cIAIs. This multicenter trial demonstrated non-inferiority of ertapenem to piperacillin-tazobactam in hospitalized patients. The present post-hoc analysis of the data generated by this randomized study was undertaken specifically to evaluate the effect of BMI on the treatment of cIAIs.
Patients and Methods
Study design
This was a post-hoc, sub-group analysis of a recently reported randomized, double-blind trial that evaluated ertapenem vs. piperacillin/tazobactam in the treatment of cIAIs. Enrolment included men and women from the ages of 18 to 90 years with presumptive (pre-operative) or confirmed (intra-operative or post-operative) complicated infections, which were defined as any infection necessitating source control (surgical drainage, resection, or percutaneous drainage). The dosing regimen was as follows. Treatment was provided for 4–14 days, according to the patient's condition, with either ertapenem (1 g once daily, followed by a saline placebo q 6 h for three additional doses daily) or piperacillin-tazobactam (3.375 g q 6 h daily) without the healthcare personnel knowing the identity of the drug given to a particular patient. There was no dosing adjustment according to the BMI. Clinical follow–up was conducted at six weeks.
This post-hoc analysis was carried out in the evaluable population described in the previous randomized controlled trial. The patients underwent initial source control either by surgical intervention (laparoscopic or open) or by radiological drainage of abscess cavities. Ertapenem or piperacillin-tazobactam was administered to all patients. Demographic characteristics were balanced between the groups for randomization into the ertapenem or piperacillin-tazobactam groups after stratification according to disease severity (Acute Physiology and Chronic Health Evaluation [APACHE] II score >10 or ≤10 points).
Outcome measures
As in the initial trial, the investigators evaluated the clinical response to treatment on the basis of clinical findings. These included changes in the signs and symptoms of infection, abdominal examination, and examination of the incision at the time of discontinuation of intravenous (IV) therapy. Early follow–up assessment (EFA) was completed at two weeks and late follow-up assessment (LFA) at 4–6 weeks. The investigator's assessment of the clinical response determined the assignment of clinical outcome. Infections were designated as showing “cure” if there was complete or substantial improvement of the index infection, such that no further intervention or antibiotic therapy was needed. Infections were designated as a clinical “failure” if there was persistent or recurrent abdominal infection; an incisional site infection, defined as an open wound with signs of infection that necessitated additional antimicrobial therapy or non-routine wound care (e.g., incision and drainage); or death related to intra-abdominal infection. The study's primary efficacy endpoint was the proportion of patients with a favorable clinical response (defined as “cure”) at the EFA. Secondary clinical efficacy endpoints were the proportion of patients who had a favorable clinical response at the end of therapy and LFA.
Statistical method
Discrete variables for demographics were compared with Fisher's exact test or the Student t-test, where appropriate (GraphPad, San Diego, CA). Difference in proportions for outcomes were analyzed, and 95% confidence intervals (CIs) for the differences in proportion were calculated as an outcome of a contingency table using an exact test. All testing was done using the same software (GraphPad Prism v 4).
Results
Study population and baseline characteristics
Figure 1 demonstrates the flow of patients through the initial randomized controlled trial [5]. The obese population was in fact closer to being morbidly obese, as the mean BMI was 37 kg/m2, the definition of morbid obesity (MO) being a BMI ≥40 kg/m2.
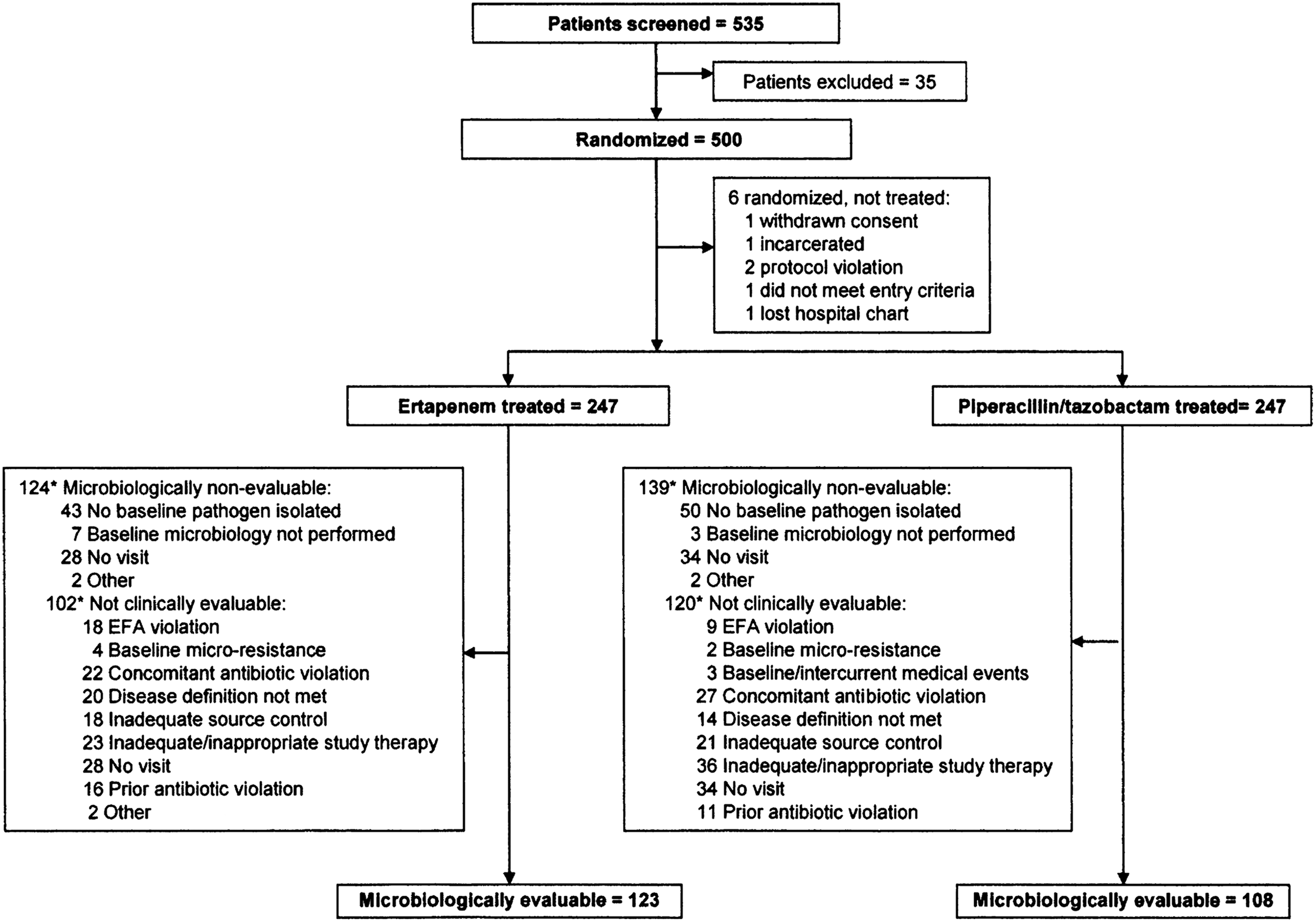
Patient Flow through initial randomized control trial, (1) with permission.
Patient characteristics are shown in Table 1. Notably, age and APACHE II scores were similar in the two groups. However, the heavier group had more patients with non-appendiceal pathology (from the colon or small bowel) and more female subjects. There was no significant difference in the number of laparoscopic approaches to surgical source control in the two groups. The BMI ≥30 kg/m2 group had a nominal 8% lower cure rate than the lower-weight group: 74.5% (41/55) vs. 82.9% (136/164). Despite the nominal difference, the 95% CI included 0 (8% difference in proportions; 95% CI −5%, 25%).
Twelve patients with missing BMI data not included.
APACHE=Acute Physiology and Chronic Health Evaluation; NS=not significant; Pip-tazo=piperacillin-tazobactam; SD=standard deviation.
For patients treated with ertapenem, there were no differences in age, APACHE II score, gender, or frequency of appendiceal pathology between BMI <30 and BMI ≥30 kg/m2 (Table 2). However, among patients treated with piperacillin/tazobactam, there were significantly more cases of non-appendiceal pathology and female sex in the heavier group (Table 3). The most frequent sources of intra-abdominal pathology were appendix (34%), colon (29%), and small bowel (13%). This was similar to the non-obese group, albeit with fewer cases of acute appendicitis. There was no statistically significant difference in clinically favorable outcomes (cure rates) between BMI groups according to the antibiotic regimen (Table 4).
None of the differences is statistically significant.
APACHE=Acute Physiology and Chronic Health Evaluation; SD=standard deviation.
APACHE=Acute Physiology and Chronic Health Evaluation; NS=not significant; SD=standard deviation.
CI=confidence interval; Pip-tazo=piperacillin-tazobactam.
Discussion
Obesity continues to increase in prevalence, not only in the U.S., but around the world. It has been considered an epidemic, with more than one-third of adults in the U.S. considered to be obese [6]. A BMI ≥30 kg/m2 is associated with a higher risk of death in addition to life-threatening medical co-morbidities [1].
Complicated intra-abdominal infections are those that extend beyond the hollow viscus of origin into the peritoneal space and are associated with either abscess formation or peritonitis. This represents a common problem, with acute appendicitis alone affecting more than 300,000 patients a year in the U.S. [7]. Additionally, the mortality rate from complicated intra-abdominal infections is substantial, with cIAI being the second leading cause of infectious death in the intensive care unit. The goals of management are based on source control, either operative (laparotomy or laparoscopy), or percutaneous drainage, with concurrent antibiotic administration. Obesity has been implicated as a risk factor in the development of post-operative surgical site infections, either superficial, deep, or organ space [8]. This also has been documented in the post-operative bariatric surgery population, possibly related to inappropriate antibiotic dosing [9]. De novo cIAIs may be affected by obesity as well, but this is not proved [10]. These are important considerations when treating patients from populations with an increasing prevalence of obesity.
Guidelines for the initial diagnosis and subsequent management of cIAIs in adult and pediatric populations have been published recently [11]. Although these guidelines highlight poor nutritional status and low serum albumin concentration as clinical predictors of failure of source control, there is no mention of the role played by obesity in cIAIs in adults. What is noted, however, is the importance of appropriate pharmacokinetics to ensure optimal antibiotic dosing. This is important to ensure maximum efficacy and minimal toxicity while reducing the risk of antibiotic resistance. Antibiotic dosing typically follows lean body mass and estimated extracellular fluid volume, as in dosing with aminoglycosides, although dosing may be considered on the basis of total body mass [3].
The antibiotics used in the present study were ertapenem and piperacillin-tazobactam. Ertapenem appears in the latest guidelines as a choice for monotherapy in community-acquired cIAI of mild-to-moderate severity. Piperacillin-tazobactam appears in these same guidelines as a choice for monotherapy in cIAI of high risk or severity.
Little has been written about the effect of obesity on therapeutic response and clinical outcomes in intra-abdominal infection. A recent pharmacokinetic evaluation in healthy adults who were obese, morbidly obese, or non-obese indicated that the standard once-daily ertapenem dosing at 1 g may in fact not achieve appropriate tissue concentration, causing underdosing and thus potentially reducing bactericidal killing. However, no clinical outcomes were measured, as the volunteers were healthy [4]. Other trials indicate that the 1-g daily dosing of ertapenem is adequate for improvement in clinical outcomes; for example, in moderate-to-severe diabetic foot infections, although obesity was not a risk factor for treatment failure on multivariate analysis [12,13]. Piperacillin-tazobactam pharmacokinetics were also studied in a single morbidly obese patient with a BMI of 50 kg/m2. The patient was receiving the drug IV for a soft tissue infection at a dose of 3.375 g q 4 h. Minimum inhibitory concentrations (MICs) of 8 mg/L were achieved more than 90% of the time, but reached 16 mg/L only 55% of the time. The authors concluded that further study is needed to dose appropriately those obese patients infected with organisms possessing elevated MICs [14].
The randomization of patients in this trial was not stratified by BMI. Accordingly, we found some differences between the BMI <30 and BMI ≥30 kg/m2 groups. The high BMI group had more non-appendiceal pathology and more female subjects. The excess non-appendiceal pathology in the high BMI group could bias the results toward worse outcomes in this group. The effect of excess female subjects in the high BMI group is not as clear. In one clinical trial on sex-related differences, female sex predisposed to a worse outcome [15], but this remains controversial. The difference in the proportion of patients with a favorable outcome in our post-hoc analysis was 8% favoring the low BMI group; the 95% CI for this difference did include 0 but was largely distributed in the positive range (−5%, 25%). It is unknown if a larger sample would have shifted the confidence interval to the right. The observed trend certainly suggests further research is needed.
There were no statistically significant differences in cure rate at EFA for either the obese or the non-obese group when analyzed with respect to antibiotic. There was, however, a trend toward a diminished cure rate in the obese piperacillin-tazobactam group. This is interesting given the abovementioned Surgical Infection Society (SIS) and Infectious Diseases Society of America (IDSA) guidelines, which recommend piperacillin-tazobactam over ertapenem in more severe or high-risk cIAIs [11]. In this group, the difference in the proportion cured among the patients with high and low BMI was 21% (95% CI of −1%, 47%). Although it includes 0, the CI is heavily skewed to the right. It is possible that piperacillin-tazobactam in particular requires higher or more frequent dosing or longer infusion times than were used. This may be true given that for patients with a BMI <30 kg/m2, this difference in the proportion cured with piperacillin-tazobactam is much less (6% vs. 21%). The meaning of this trend is made less clear by the above-mentioned fact that the obese patients receiving piperacillin-tazobactam had more non-appendiceal pathology and more women than did the non-obese patients receiving piperacillin-tazobactam. No such difference between obese and non-obese patients receiving ertapenem was observed; therefore, the trend to worse outcomes in the obese patients receiving piperacillin-tazobactam may simply be an artifact of unfavorable distribution of patient characteristics in this post-hoc analysis.
There are limitations to this study. This was a post-hoc analysis of a previous randomized controlled trial, with limitations inherent in post-hoc design, including small sample size for sub-group analysis. Therefore, this study is prone to a type II error, as there were few patients who were obese. Additionally, the inclusion and exclusion criteria of the first trial may limit overall generalizability of this analysis to unselected patient populations.
It is difficult to know the role that pharmacokinetics and pharmacogenetics play in the treatment of cIAI in obese populations. Whereas some pharmacokinetic modeling has demonstrated underdosing at all BMIs with 1 g of ertapenem IV, there are no clinical data to support this view [4]. Additionally, underdosing may occur with piperacillin-tazobactam in this and other obese populations [14,16]. It remains to be seen, with larger randomized trials, if piperacillin-tazobactam indeed must be administered and dosed in specific ways for obese populations to eliminate the trend seen here toward treatment failure.
In compliance with full disclosure, it must be stated that the data were generated from an industry-sponsored trial. Such trials have been prone to publication bias, in favor of the industry-sponsored drug, limiting the usefulness of the results [17–20]. It is possible, but unclear, if this sponsorship influenced the results of this post-hoc analysis.
Conclusions
Complicated intra-abdominal infections remain a clinical challenge to treat in both the obese and non-obese populations. Appropriate source control coupled with antibiotic therapy is the mainstay of treatment. In this post-hoc analysis, we found that there were no differences in treatment failure between obese and non-obese patients with cIAIs. Although there was a nominal, but not statistically significant, increase in treatment failure for the obese group receiving piperacillin-tazobactam, this may be secondary to demographic factors such as type of cIAI or gender. These data highlight the need for further randomized trials of antibiotics that consider differences in pharmacokinetics, pharmacodynamics, and pharmacogenetics in obese and non-obese populations.
Footnotes
Author Disclosure Statement
NN is a speaker for Merck & Co. and a participant in a Merck Advisory Board, for which he receives honoraria. DAH is an employee of Merck & Co. TZ has no competing financial interests.