
Abstract
Abstract
Background:
Cefazolin is used commonly to prevent surgical site infection (SSI) after operations on patients with morbid obesity (MO), but specific dosing guidelines are lacking. We hypothesized that cefazolin 2 g given by intravenous (IV) push over 5 min (IVP) or infusion over 30 min (INF) would suffice for SSI prophylaxis in MO (body mass index [BMI] 40–50 kg/m2), and cefazolin 3 g would be sufficient in patients with super-morbid obesity (SMO) (BMI >50 kg/m2).
Methods:
Twenty-five patients undergoing elective surgical procedures were given a single dose of cefazolin: Ten with MO received 2 g via IVP (MO2-IVP), five with MO received 2 g via 30-min infusion (MO2-INF), five with SMO received 2 g via infusion (SMO2-INF), and five with SMO received 3 g via infusion (SMO3-INF). Serum cefazolin concentrations were measured 5, 30, 120, and 360 min after initiation of the dose. The half-life of the drug was calculated for each patient, as was the time the concentration was above the minimum inhibitory free concentration (fT>MIC) using 8 mcg/mL as the breakpoint. The protective duration of each cefazolin dose was assessed using the pharmacodynamic target for fT>MIC of 70%.
Results:
The mean cefazolin concentrations after 30 min were similar in all groups; the mean concentrations at 120 and 360 min were 67.1–84.8 mcg/mL and 22.9–40.8 mcg/mL, respectively. The half-life ranged from 2.3 to 3.6 h and was unaffected by administration method. The protective duration was 5.1 h for MO2-IVP, 4.8 h for MO2-INF, 5.8 h for SMO2-INF, and 6.8 h for SMO3-INF.
Conclusions:
A single 2-g dose of cefazolin appears to provide antibiotic exposures sufficient for most common general surgical procedures of <5-h duration, regardless of BMI.
Obesity is postulated to be a risk factor for surgical site infection (SSI) after a variety of surgical procedures [6–8]. Clinicians should be aware of alternate antibiotic dosing regimens to provide adequate prophylaxis for this population. However, the pharmacokinetics of antibiotic dosing in patients with MO is complicated, and studies are few in number. Antibiotics that require therapeutic monitoring, such as aminoglycosides and vancomycin, have been studied most thoroughly [9,10]. Dosing is drug-specific because of the variability in a variety of parameters, including body composition, affinity for plasma proteins, and drug lipophilicity [11,12]. Obese patients additionally have variations in blood flow to adipose tissue, cytochrome P450 activity, and glomerular filtration rate, all of which can affect pharmacodynamics [13]. Because of the relative unpredictability of pharmacokinetics in obese individuals, doses are best estimated on the basis of specific studies for individual drugs carried out in obese individuals. For example, vancomycin should be given on the basis of actual body weight, with dosage adjustments based on serum concentrations [14], whereas aminoglycoside dosing requires calculation of adjusted body weight via a correction factor [15].
Optimal dosing regimens for beta-lactam antibiotics have been less studied in this population, despite the fact that first-generation cephalosporins remain the drugs of choice for surgical prophylaxis. The efficacy of these antibiotics depends on the time the free drug concentrations are above the minimum inhibitory concentration (MIC) (fT>MIC). In general, beta-lactam agents are efficacious when administered such that their fT>MIC exceeds 60–70% of the dosing interval [16].
The purpose of this study was to determine an optimal dosing regimen for cefazolin as a prophylactic antibiotic in surgery in patients with MO. We hypothesized that cefazolin 2 g, given either via intravenous (IV) push over 5 min (IVP) or as a 30-min IV infusion (INF), would suffice for SSI prophylaxis, but that a larger dose of cefazolin (3 g) might be necessary in patients with super-morbid obesity (SMO).
Patients and Methods
The study protocol was reviewed and approved by the Committee on Human Rights Research of Weill Cornell Medical College. Patients undergoing surgical procedures for MO (including Roux-en-Y gastric bypass, biliopancreatic diversion, sleeve gastrectomy, and gastric banding) were enrolled according to institutional informed consent guidelines. Twenty-five obese patients scheduled for bariatric surgery were weighed, and the body mass index (BMI) was calculated. All patients received a single dose of cefazolin. Patients with BMI >40 kg/m2 were recruited for the study in four groups: Group 1=ten patients with BMI 40–50 kg/m2 received cefazolin 2 g via IVP (MO2-IVP); Group 2=five patients with BMI 40–50 kg/m2 received cefazolin 2 g via INF (MO2-INF); Group 3=five patients with BMI >50 kg/m2 received 2 g cefazolin via INF (SMO2-INF); and Group 4=five patients with BMI >50 kg/m2 received 3 g of cefazolin via INF (SMO3-INF). Alanine and aspartate aminotransferase were assayed, as hepatic disease can affect the half-life and protein binding of cefazolin [17]. Patients with allergy to penicillins or cephalosporins, current pregnancy or lactation, chronic kidney disease, or chronic hepatic insufficiency were excluded. Patients were assigned consecutively to groups after determination of BMI.
Blood samples were taken at 5, 30, 120, and 360 min after dose initiation. The blood was allowed to clot for 10 min and centrifuged at 3,200 rpm for 10 min to separate the serum, which was stored immediately at −80°C until analysis. Cefazolin concentrations were determined using a previously validated high-performance liquid chromatography method at the Center for Anti-Infective Research and Development (Hartford, CT) [18]. The assay was linear over a range of 0.5 to 50 mcg/mL (R2=0.997). Intra-day coefficients of variation for the low (1 mcg/mL) and high (40 mcg/mL) quality-control samples were 3.6% and 3.4%, respectively. Inter-day coefficients of variation were 4.9% and 3.7%, respectively.
Patient group characteristics were analyzed using measures of central tendency and the Kruskal-Wallis one-way analysis of variance. The elimination rate constant (ke) was calculated using a linear regression of the terminal portion of the concentration time profile, and the half-life was determined by 0.693/ke. All calculations were performed using STATA version 11.0 (Stata Corp., College Station, TX). The fT>MIC was determined using a protein binding value of 85%. The fT>MIC of 8 mcg/mL was determined for each patient, as was the protective duration of each regimen using the pharmacodynamic target of fT>MIC of 70%.
As secondary analyses, correlation and univariable regression were performed on the 20 patients who received 2 g of cefazolin to determine if weight, BMI, or age was associated with the cefazolin concentration at t=30 min (peak) and t=360 min (trough).
Results
Sixteen females and nine males were recruited for the study; by happenstance, the MO2-INF group included only females. Operations consisted of 12 Roux-en-Y gastric bypass procedures, seven placements of adjustable gastric band devices, five sleeve gastrectomies, and one biliopancreatic diversion with duodenal switch. Patient characteristics, including age, weight, BMI, and measured creatinine concentration, are presented in Table 1. The mean BMIs were 44.1±3.3 (standard deviation [SD]) in the MO2-IVP group, 43.7±3.4 in the MO2-INF group, 55.7±8.8 in the SMO2-INF group, and 55.2±2.9 in the SMO3-INF group; p<0.01. There were no significant differences in age, serum creatinine concentration, or serum albumin concentration among the groups. Whereas there was a trend toward a difference among the groups in alanine aminotransferase and aspartate aminotransferase concentrations (p=0.06 for both), all concentrations were well within normal limits.
Values presented as mean±standard deviation.
Kruskal-Wallis analysis of variance.
INF=intravenous infusion over 30 min; IVP=intravenous push over 5 min; MO=morbid obesity; SMO=super-morbid obesity.
The mean total cefazolin concentrations in each patient group (mcg/mL) are presented in Table 2. After t=30, mean concentrations were similar in all groups; p=0.64 for t=120 and p=0.51 for t=360. The administration method did not significantly affect the half-life of cefazolin, which ranged from 2.3–3.6 hours. As displayed in Table 2, the fT>MIC at an MIC of 8 mcg/mL ranged from 3.4–4.8 h, whereas the protective duration ranged from 4.8–6.8 h in these MO and SMO patients.
For MIC 8 mcg/mL.
Calculated using fT>MIC=0.70, where MIC=8 mcg/mL.
INF=intravenous infusion over 30 min; IVP=intravenous push over 5 min; MIC=minimum inhibitory concentration; MO=morbid obesity; SD=standard deviation; SMO=super-morbid obesity.
The mean free cefazolin concentration time profiles of the MO and SMO populations are presented in Figure 1. Intravenous push administration gave the highest peak mean concentration, which was documented immediately after administration. However, cefazolin was eliminated at a similar rate in groups, as evidenced by the similar half-lifes in each group. Even though the administration method led to different concentrations initially, the differences diminished over time such that the fT>MIC was similar in all groups.
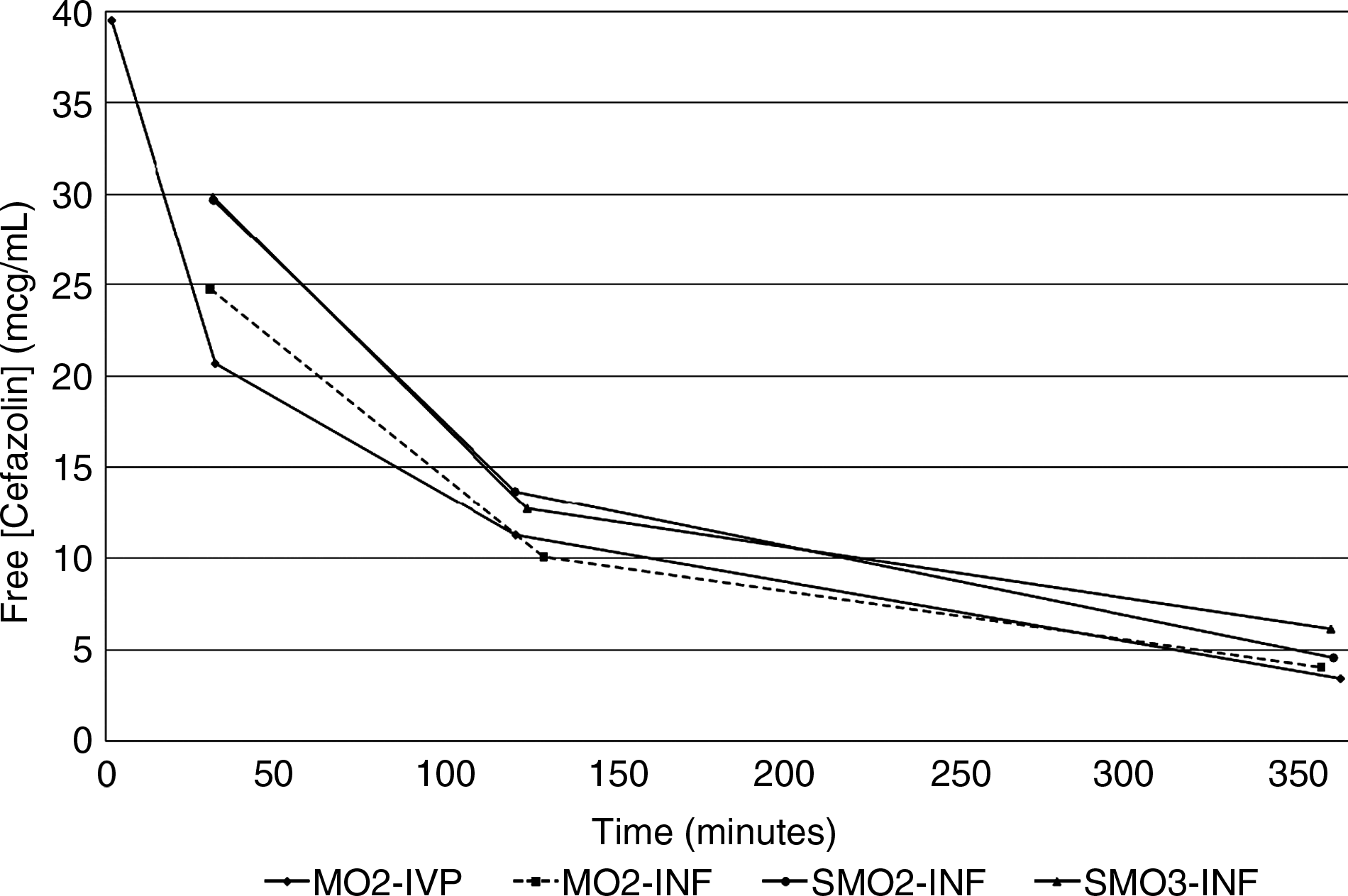
Mean free cefazolin concentrations (mcg/mL) over time for four patient groups. MO2-IVP=Group 1, Body mass index (BMI) 40–50 kg/m2; received cefazolin 2 g via intravenous (IV) push; MO2-INF=Group 2, BMI 40–50 kg/m2; received cefazolin 2 g via 30-min IV infusion; SMO2-INF=Group 3, BMI >50 kg/m2; received cefazolin 2 g via 30-min IV infusion; SMO3-INF=Group 4, BMI >50 kg/m2; received cefazolin 3 g via 30-min IV infusion.
In the secondary analyses, determination of the correlation coefficients and univariable regression were performed on the 20 patients who received 2 g of cefazolin to determine if weight, BMI, or age was associated with cefazolin concentration at t=30 and 360 min. The correlation coefficient at t=30 min was 0.08 for weight, 0.13 for BMI, and 0.20 for age; at t=360 min, the correlation coefficients were 0.29, 0.42, and −0.16, respectively. Total body weight, BMI, and age thus were not correlated with cefazolin concentrations and were not significantly associated by linear regression at either time point (Table 3), indicating that dosing based on weight as opposed to BMI is moot.
CI=confidence interval.
Discussion
Concerns in the political and regulatory arenas about increasing healthcare costs have led to the development of measures intended to limit cost and improve quality. One such measure, devised by the Centers for Medicare and Medicaid Services (CMS), specifically targets SSI after bariatric surgery as a “hospital-acquired condition.” The implication of this designation is that in 2009, CMS stopped reimbursements to hospitals for treatment of SSI in inpatients after bariatric surgery [19]. Therefore, the development of SSI in bariatric patients has not only clinical implications for patients but also economic implications for hospitals and physicians.
The SSI rate after bariatric surgery has been reported to be between 1.3% and 22.0%, with wide variation secondary to evolving practices and non-standardized reporting [20–22]. Recent data from a multi-institutional prospective trial examining staple height as a function of leak rate after laparoscopic gastric bypass surgery reported the overall superficial incisional SSI rate to be 7.9% [23]. Morbid obesity is itself a major risk factor for SSI; a 1989 study noted a 16.5% incidence in patients with MO undergoing clean-contaminated surgery, compared with 2.5% in a non-obese group [20]. Laparoscopy is associated with lower rates of SSI, with a significant differential in SSI rates from as high as 10.5% after open operations to 1.3% after laparoscopic procedures [22]. In addition, a variety of other factors have been associated with higher infection rates. One study of laparoscopic gastric bypass noted a decrease in SSI rate from 22% to 1.5% after institution of routine bowel preparation and systematic use of a wound protector for removal of the stapler [24].
Administration of antibiotics and the dose administered also are key components of prevention of SSI in MO. In the 1980s, two studies reported use of cefazolin in MO populations. An early study of open procedures showed a reduction in SSI incidence from 21% to 4% when a prophylaxis regimen of 1 g cefazolin was used compared with placebo [21]; a later study showed a similar effect when cefazolin 2 g was used instead of 1 g, with a decrease from 16.5% to 5.6% [20]. A more recent study evaluated serum and tissue concentrations of cefazolin in three groups of patients: BMI 40–49 kg/m2, 50–59 kg/m2, and ≥60 kg/m2. All three groups received 2 g for prophylaxis, with a scheduled second dose at 3 h. Blood sampling was performed relative to the time of incision, as opposed to drug administration time. Serum concentrations measured immediately before the second dose noted that 41.1% of the samples from the BMI 40–49 kg/m2 group were above the therapeutic threshold, defined as 32 mcg/mL; 18.2% of samples from the 50–59 kg/m2 group and no samples from the ≥60 kg/m2 group were above the cut point [25], but cefazolin protein binding was not considered in the analysis.
In addition to dose, the optimal regimen for cefazolin should specify the infusion method and parameters for redosing. Our data indicate that cefazolin is appropriate prophylaxis for MO and SMO against pathogens with expected MICs <8 mcg/mL, the typical pathogens causing SSIs after elective surgery. In the 2-g groups, an infusion over 30 min led to similar concentrations and durations as administration via a 5-min IV push, the latter being ideal for convenience of administration in the immediate pre-operative setting. For MO and SMO, cefazolin 2 g can be administered safely by IV push or by 30-min infusion. As administered, the 2-g or 3-g doses will provide concentrations above the MIC of 8 mcg/mL for at least 3.4 h. Using a protective duration of fT>MIC of 70%, the time to redosing would be 5 h. Although the 3-g dose of cefazolin is safe for patients with BMI >50 kg/m2, this dose does not appear necessary, as a 2-g dose provided sufficient exposure. Our data suggest that a single 2-g dose of cefazolin is likely to be sufficient for most common general surgical procedures of <5 h duration, regardless of body mass. In our analysis, neither patient age, weight, nor BMI was associated significantly with peak or trough cefazolin concentrations.
This study has several limitations. The sample size was small and consisted only of healthy patients undergoing elective surgery. These data thus cannot be extrapolated to critically ill populations or patients with renal dysfunction. There also was no control group of patients with normal BMI, but the pharmacokinetics of normal-weight individuals have been described for cefazolin. The small sample size did not allow determination of the relation between serum cefazolin concentration and clinical outcomes. However, the goal of this study was to perform a pharmacokinetic study on a morbidly obese population, and the sample size is adequate for this purpose. Additionally, clinicians should consider the distribution of the antibiotic to the peripheral tissues for maximum efficacy. Future studies should look more closely at the timing of tissue distribution and concentrations to determine the potential for efficacy.
In 2010, the Clinical and Laboratory Standards Institute (CSLI) revised the MIC breakpoints for treatment of Enterobacteriaceae infections with multiple cephalosporins and aztreonam, including cefazolin. For cefazolin, an MIC ≥4 mcg/mL is now considered resistant, MIC 2 mcg/mL is considered intermediate, and only MIC ≤1 mcg/mL indicates susceptibility [26]. These breakpoints were revised to reflect contemporary gram-negative pathogens, accounting for increasing occurrence of resistance mechanisms such as extended-spectrum beta-lactamases and AmpC-type enzymes. In light of these new resistance breakpoints, interpreted for an MIC ≤1 mcg/mL, the dosing interval for all four groups could be extended to >7 h to maintain fT>MIC at 100%. Although clinicians need to consider that gram-negative pathogens are showing increasing resistance to cefazolin in the context of surgical prophylaxis, these pathogens are infrequent causes of infection. When considering methicillin-susceptible Staphylococcus aureus, the majority of MICs for cefazolin are ≤2 mcg/mL; thus, using the prior breakpoint of ≤8 mcg/mL with the 2-g prophylaxis regimen utilized in this study provides a high probability that adequate exposures will be achieved for procedures lasting ≤5 h.
Strategies beyond conventional prophylaxis to prevent SSI have been postulated. Both randomized and non-randomized studies suggest that continuous infusion of beta-lactam antibiotics increases the fT>MIC and allows more consistent attainment of therapeutic concentrations [27, 28]. However, these trials were performed in specific clinical settings such as critically ill patients or those with chronic obstructive pulmonary disorders [29, 30]. Whether this administration method is effective for prophylaxis has yet to be elucidated [31]. Alternatively, some success has been noted in MO utilizing an infusion of kanamycin into the subcutaneous space of the incision; in one study, only six of 837 patients undergoing open abdominal bariatric surgery (0.72%) developed deep incisional SSIs, a rate much lower than other published SSI rates in MO [32]. Prevention of SSI in MO and SMO will require vigilant, simultaneous use of multiple strategies, including appropriate antibiotic administration, antisepsis techniques, careful tissue handling, and management of individual patient risk factors.
Footnotes
Acknowledgments
The authors thank Christina Sutherland of the Center for Anti-Infective Research and Development for her assistance with determination of cefazolin concentrations.
Author Disclosure Statement
No conflicting financial interests exist.