
Abstract
Abstract
Background:
Cytomegalovirus (CMV) enteritis presenting with perforation in the setting of acquired immunodeficiency syndrome (AIDS) represents a particularly deadly combination.
Methods:
Case report and review of the pertinent literature.
Case Report:
The authors report a patient with AIDS and CMV enteritis presenting as recurrent small-bowel obstruction and leading to perforation of the jejunum with subsequent survival.
Conclusion:
This is believed to represent the second case in the English-language literature of survival after CMV-induced small intestinal perforation in a patient with AIDS.
Case Report
The patient is a 50-year-old man found to have AIDS (CD4+ count 18/mcL) two months prior to presentation. Approximately one month before presentation, he was hospitalized twice at an outside facility for a partial small bowel obstruction. A computed tomography (CT) scan of the abdomen/pelvis was consistent with such obstruction, with a transition zone seen in the distal small bowel. A small bowel follow-through radiograph demonstrated a thickened area in the distal small bowel. The patient underwent esophagogastroduodenoscopy and colonoscopy, which revealed mild gastritis and duodenitis with normal colonic tissue and terminal ileum (60–70 cm of distal ileum examined), respectively. Retrograde ileoscopy was performed subsequently, and a friable, firm, edematous, and ulcerated area was identified approximately 100 cm from the ileocecal valve with apparent involvement of at least 80–100 cm of the mid- and distal ileum. Biopsies revealed severe CMV-associated ileitis. Serum assays showed an elevated concentration of CMV IgG antibodies. Flow cytometry-based immunophenotyping indicated nothing suggestive of a lymphoproliferative disorder. The patient was treated with intravenous hydration, nasogastric tube decompression, and valganciclovir, with symptomatic improvement.
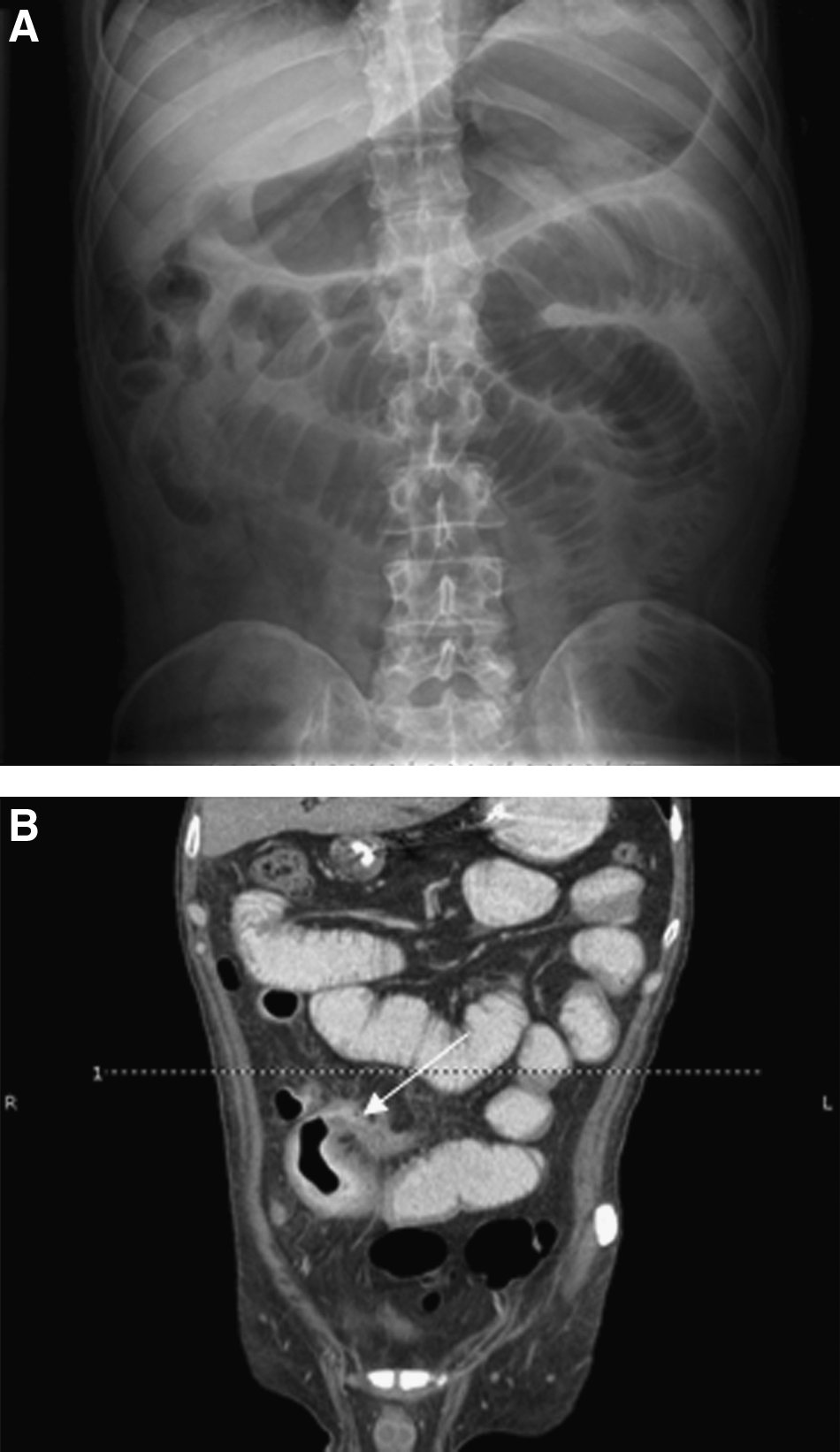
Approximately one month after discharge from the referring hospital, the patient presented to our facility with a three-day history of diffuse, crampy lower-quadrant abdominal pain associated with nausea, emesis, and diarrhea. Of note, the patient had no other notable medical history and no previous abdominal operations. At initial evaluation, the patient was afebrile but tachycardic. His physical examination was remarkable for bilateral lower-quadrant abdominal tenderness to palpation. Laboratory parameters were remarkable for a white blood cell count of 3,300/mcL (46% neutrophils, 2% bands) and a serum albumin concentration of 1.4 g/dL. Initial abdominal radiographs revealed a distended loop of small bowel in the upper mid-abdomen suggestive of a partial small bowel obstruction (Fig. 1). A CT scan of the abdomen/pelvis demonstrated several dilated loops of proximal small bowel with a transition point in the distal small bowel and significant adjacent stranding (Fig. 2).

Initial abdominal plain film performed on admission reveals distended loop of small bowel in upper mid-abdomen, suggesting partial small bowel obstruction.
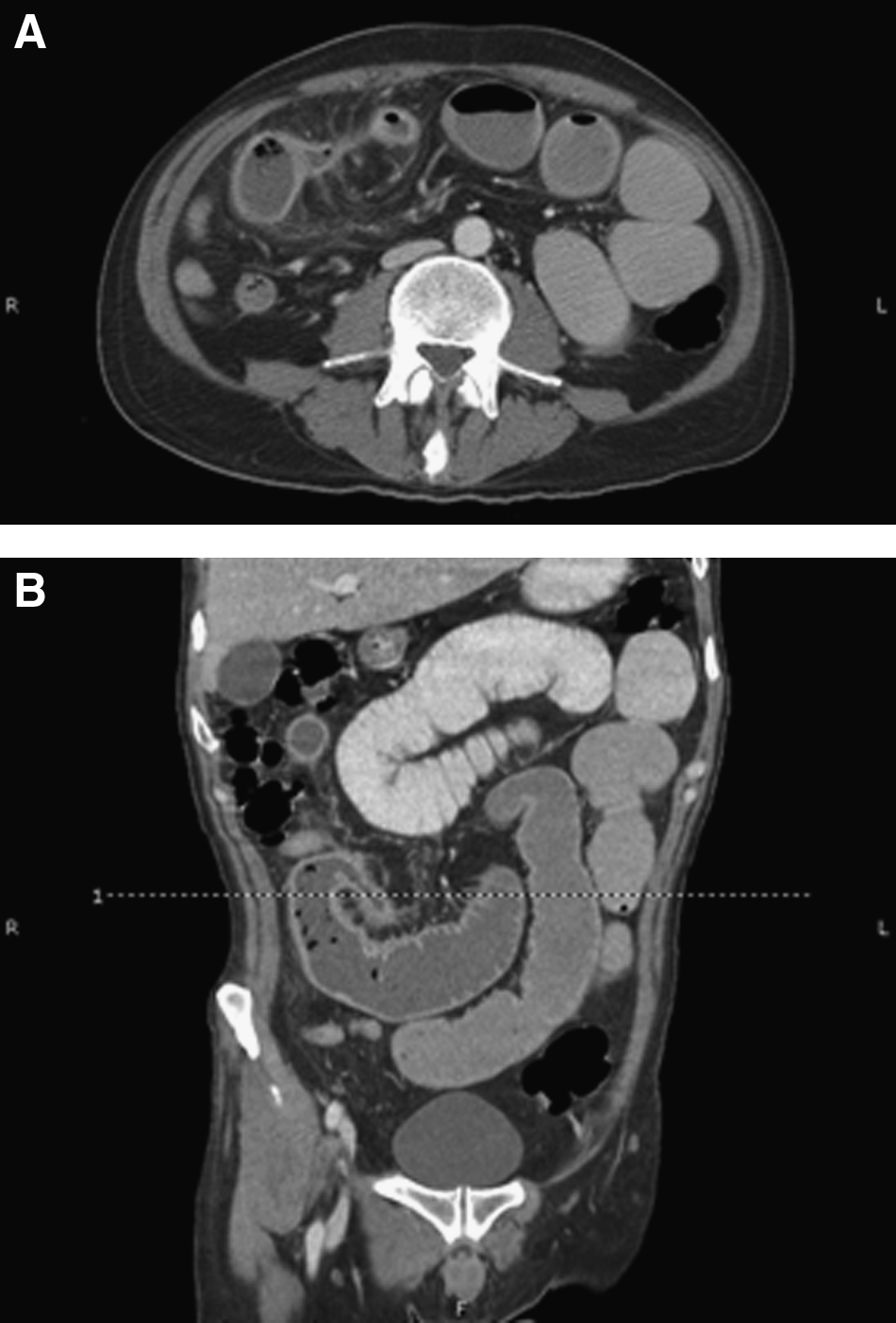
CT scan of abdomen/pelvis performed for further elucidation of plain film findings demonstrates several dilated loops of proximal small bowel with transition point in distal small bowel (
Given the patient's previous episode of CMV enteritis, he was admitted for non-operative management with ganciclovir, bowel rest, and intravenous hydration. He was followed with serial abdominal examinations and had both symptomatic and radiographic resolution of the apparent obstruction. However, five days after admission, the patient had recurrent severe crampy lower-quadrant abdominal pain associated with nausea and emesis. A repeat abdominal plain film indicated recurrent partial small bowel obstruction (Fig. 3). The patient had improvement in abdominal pain with nasogastric decompression. A repeat CT scan of the abdomen/pelvis demonstrated small bowel obstruction with a transition point again identified at the level of the distal small bowel. Stranding was noted around the transition point; however, a new focus of air was seen corresponding to gas within the bowel lumen, abscess, or focal perforation (Fig. 3).
After clinical decompensation, repeat abdominal plain film (
Because of the lack of improvement with conservative therapy and the new finding of possible extraluminal air, the patient was taken to the operating room. Intra-operatively, a moderate amount of pelvic ascites was seen, along with dark stains on the small bowel similar to what is seen with an endometriosis-type implant. A functional partial small-bowel obstruction was found secondary to several loops of intestine encasing a distal jejunal perforation. A small-bowel resection followed by a stapled side-to-side anastomosis was performed. The entire small bowel was examined without findings of additional abnormalities. Surgical pathology examination revealed mucosal ulceration with granulation tissue and mucosal epithelial cells with CMV inclusions consistent with a diagnosis of CMV jejunitis (Fig. 4).
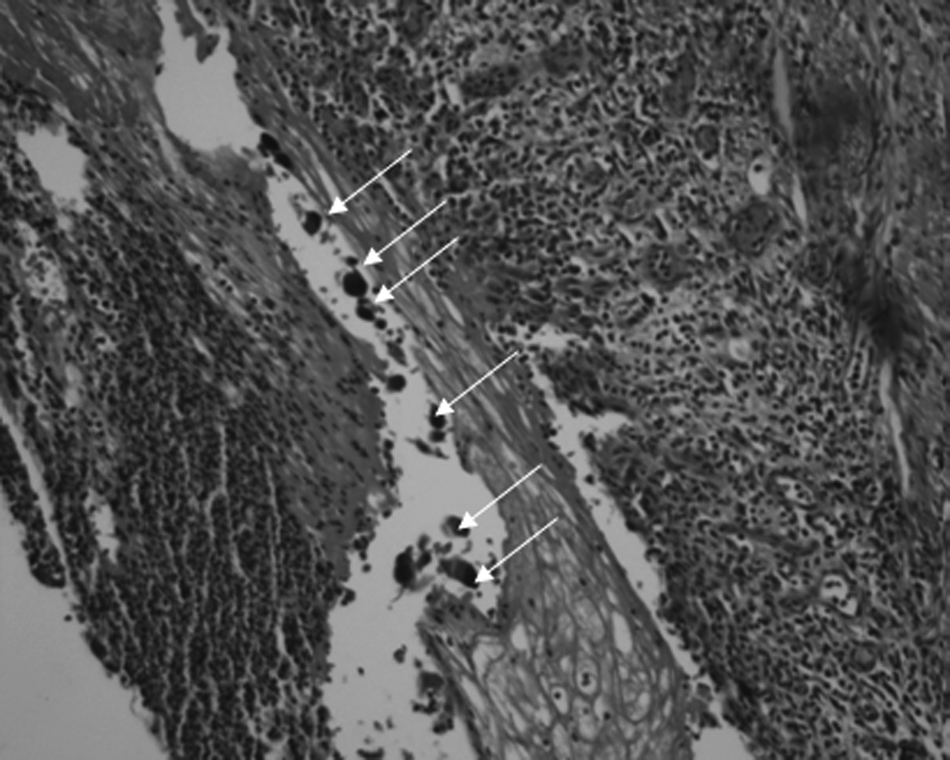
Representative section (hematoxylin and eosin stain) of mucosa demonstrating epithelial cells with cytomegalovirus inclusions (arrows).
Post-operatively, the patient had a rapid return of bowel function and no complications. At followup clinic visits up to two months later, the patient was without gastrointestinal tract complaints. On triple therapy (efavirenz, emtricitabine, and tenofovir disoproxil fumarate), his CD4+ count continued to increase, and his viral load continued to decrease (42/mcL and <48 copies/mL, respectively, when measured approximately two months after surgery).
Discussion
The most common presenting symptoms of CMV gastroenteritis are fever, abdominal pain, and diarrhea (less common with disease limited to the small bowel). The pathophysiology of CMV-related enteritis appears to be related in part to upregulation of the production of local pro-inflammatory cytokines, potentially by altering resident intestinal macrophages to express HIV proteins [2]. Infection is most common in patients with a CD4+ count ≤100/microliter. The diagnosis may be suggested by laboratory findings but is confirmed by endoscopy with biopsy revealing CMV inclusion bodies. Initial treatment usually is with anti-viral medications [3]. The majority of affected patients die from the consequences of intra-abdominal sepsis or other opportunistic infections [4].
Meza et al. reported their case of CMV causing ileal perforation and subsequent death and described eight additional cases of CMV-related small-intestinal perforation. Only two of the reported nine cases involved a jejunal perforation. Eight patients died despite definitive surgical therapy. The only patient previously reported who survived had a jejunal perforation and was treated with ganciclovir [4–6]. This report described the course of a patient with AIDS and CMV enteritis presenting as recurrent small bowel obstruction and complicated by jejunal perforation.
Remarkably, and as reported rarely in the literature, we saw survival after perforation and definitive surgical therapy. This is believed to represent only the second report in the English-language literature of survival by a patient with AIDS and CMV-associated small-bowel perforation. Despite the patient's low CD4+ count and serum albumin concentration, and lack of significant anti-retroviral therapy targeting the AIDS, the two factors that likely contributed to the patient's outcome were the contained nature of the perforation (preventing uncontrolled intra-abdominal sepsis) and the short interval to operation once perforation was suspected.
There are several important issues deserving of mention. On presentation to our hospital, the patient had a recurrent small-bowel obstruction after initial success with conservative anti-viral therapy. He remained on anti-viral therapy despite documented treatment failure (manifested by recurrent small-bowel obstruction) with initial improvement and quick relapse with perforation necessitating operative intervention. In such patients, there may be a role for CMV resistance testing by phenotypic plaque reduction, genotypic, or viral load assay. Of the three, genotypic assays are the most relevant clinically and the most reproducible and detect mutations in viral genes UL97 (phosphotransferase) and UL54 (viral DNA polymerase). If resistance is noted, there may be a role for alternate or combination anti-viral therapy, including foscarnet. In fact, current recommendations for the treatment of patients with AIDS and CMV infection of the gastrointestinal tract include induction therapy with intravenous ganciclovir or foscarnet for three to six weeks with or without maintenance therapy. In cases of relapse, combination therapy may be effective. Although not studied widely, cidofovir may be useful in cases not responsive to standard anti-viral therapy [3,7,8]. Valganciclovir, an oral drug related to ganciclovir, has not been studied widely as an induction agent for gastrointestinal CMV disease; however, it may be a good choice, given its easy route of administration and good bioavailability.
The patient described in this report had multiple factors that predicted a higher risk of post-operative complications, including the low CD4+ count [9] and severe malnutrition [10]. The authors propose that quicker operative intervention in the setting of CMV enteritis not responsive to standard conservative therapy can prevent CMV-induced perforation and the associated death. In addition, this extremely limited dataset suggests that treatment with ganciclovir or targeted anti-viral therapy in patients with suspected CMV-associated small bowel perforation is mandatory for survival.
Footnotes
Author Disclosure Statement
No competing financial interests exist. No financial support was received for this work.