
Abstract
Abstract
Background:
Antibiotic prophylaxis guidelines suggest single-dose regimens are adequate, but comparisons of multiple agents are lacking. We compared post-operative infection rates retrospectively among six common prophylactic agents given as a single dose to colorectal surgery patients.
Methods:
A commercial database supplied demographics, All-Patient Refined Diagnosis-Related Groups (APR DRGs), International Classification of Disease (ICD)-9 codes, and drug utilization information for patients discharged from 303 hospitals from January 2007–December 2008 whose charts had been sampled for reporting Surgical Care Improvement Project (SCIP) measures. The patients (n=4,634) had the same APR DRG, no baseline infection, and prophylaxis discontinued within 24 h of surgery. Development of infection was determined by ICD-9 code. “Single dose” was defined as ≤3 g of ampicillin–sulbactam (AMP); ≤2 g of cefotetan (CFT), cefoxitin (FOX), or ertapenem (ERT); or metronidazole and ≤2 g of cefazolin (CFZ) or ≤750 mg of levofloxacin (LVX) given on the day of the procedure. Multivariable logistic regression evaluated factors associated with infection, including agent choice.
Results:
Frequency of use and rate of infection (3.7% overall) were FOX 1,752 (4.9%), ERT 1,166 (2.7%), CFZ 549 (2.7%), AMP 447 (3.6%), LVX 402 (3.2%), and CFT 318 (3.5%). The unadjusted infection rate differed by agent (p=0.037). Multiple regression analysis found infection to be associated significantly with increasing APR DRG severity, longer procedures, younger age, and male gender (p<0.01 for each except p=0.02 for age), as well as agent choice. Among agents (vs. FOX as reference), ERT was associated with a lower infection rate (odds ratio 0.53; 95% confidence interval 0.34–0.82; p<0.01); the odds ratio for all other agents contained the value 1.0.
Conclusions:
Agent selection among prophylactic antibiotics is one of many factors associated with infection development in colorectal surgery patients.
At this writing, the Draft Therapeutic Guidelines on Antimicrobial Prophylaxis in Surgery—a collaborative document by the American Society of Health-System Pharmacists, Infectious Diseases Society of America (IDSA), Society for Healthcare Epidemiology of America (SHEA), and Surgical Infection Society (SIS)—is available on the ASHP website (www.ashp.org/prophylaxis; accessed September 22, 2010; hereinafter referred to as the Draft Guidelines). These Guidelines discuss many aspects of prophylaxis in colorectal surgery, but indicate that, although the selected agent obviously should have activity against the anaerobic and aerobic flora of the bowel, “the optimal choice of antimicrobial agent has not been resolved fully.”
Single-dose prophylaxis is considered desirable for simplicity and is as efficacious as multiple doses, although re-dosing is recommended for longer procedures because the concentration of antibiotic decreases with time (and because most agents recommended for prophylaxis exhibit time-dependent killing). The Draft Guidelines concur with this assertion. Similarly, a recent Cochrane database meta-analysis of randomized controlled trials of prophylactic antibiotic use in colorectal surgery found no significant difference in infection rates in patients given single-dose vs. multiple-dose regimens (relative risk [RR] 1.17; 95% confidence interval [CI] 0.67–2.05); however, it did find that additional anaerobic coverage produced improvement (RR 0.55; 95% CI 0.35–0.85) [9].
Whereas single- vs. multiple-dose strategies have been studied widely, most reflect comparisons of a single dose of one agent with a multiple-dose regimen of another. Few studies comparing single and multiple doses of the same agent can be found in the literature; indeed, the Draft Guidelines note only two such studies, both of which were conducted prior to 1990 [10,11]. However, a recent study by Fujita et al. comparing one and three doses of a cephalosporin (in the absence of metronidazole) as prophylaxis in elective colorectal procedures did find a significant difference in incisional infection rates in favor of multiple dosing (14.2% vs. 4.3% for one vs. three doses; p=0.009 unadjusted), but not in organ/space infection (2.6% vs. 4.8%; p=0.26 unadjusted]) [12]. Additionally, those investigators reported a lower incidence of incisional infection in the three-dose group even among procedures lasting <3 h (i.e., where only one dose was given). This finding suggests that a higher antibiotic concentration even after the incision has been closed may affect infectious outcomes, raising the hypothesis that different agents with different concentration–time profiles might yield different outcomes when each is administered once. The Draft Guidelines state with emphasis that “no evidence supports greater efficacy for doses given after completion of the procedure,” while recommending that additional doses be considered for procedures lasting longer than 3–4 h, depending on the half-life of the agent.
Thus, although a consensus seems to have formed around the efficacy of single-dose prophylaxis, the influence of factors such as drug half-life remain unclear. Further, the current literature lacks a direct comparison of the available single-dose agents. To address this, we evaluated the rate of post-operative infection in colorectal surgery patients given only a single dose of any one of six commonly utilized agents (with anaerobic coverage, if appropriate), while controlling for other risk factors for infection.
Patients and Methods
Data sources and patient selection
Patient-level discharge data were obtained from Premier Inc. (Charlotte, NC), a commercial entity that aggregates inpatient billing data from >400 U.S. hospitals. The initial patient cohort was identified by International Classification of Disease (ICD)-9 codes as those who were discharged between January 1, 2007 and December 31, 2008 after undergoing a qualifying colorectal procedure and were sampled by their hospital for reporting to the Surgical Care Improvement Program (SCIP), such that SCIP measures were reported to Premier. According to the SCIP methodology, only patients with no evidence of baseline infection can be sampled; as such, all patients in our cohort appeared to be infection–free at the time of surgery. We also requested data on re-admissions within 30 days for the cohort for follow-up.
Only patients who had a recorded response to SCIP measure Inf_1f (received prophylactic antibiotic within 1 h of incision) were included, to enable the investigators to control for compliance with this measure. This cohort was then reduced to those patients with an All-Patient Refined Diagnosis-Related Groups (APR DRG) of 221 (Major Small and Large Bowel Procedures) to enable comparison using the APR DRG-specific severity score. This constituted the “overall cohort.” The cohort was reduced further to those who received a single dose of prophylactic antibiotic (as defined below), and whose antibiotic was discontinued within 24 h of surgery (documented by the corresponding SCIP measure). The purpose of the 24 h criterion was to attempt to exclude patients for whom an initially unsuspected infection was discovered during the colorectal procedure. This constituted the “comparison cohort,” in which the study analyses were conducted.
Definitions and variables assessed
Patients were considered to have received a “single dose” of prophylactic antibiotic if they received one of the following on the day of their colorectal procedure: ≤3 g of ampicillin–sulbactam or ≤2 g of cefotetan, cefoxitin, or ertapenem. Alternatively, the patient could have received either ≤2 g of cefazolin or ≤750 mg of levofloxacin if metronidazole was given also. Demographic data collected included age, race, and gender; the co-morbidities measured were diabetes mellitus and chronic obstructive pulmonary disease (COPD). Descriptive data were collected on admitting physician specialty and admission source.
The surgical variables collected were indication for surgery, admission type (elective, emergency, urgent, or other), procedure type, and procedure duration (in minutes unless elsewhere noted). The indication for the procedure was grouped into six categories: Benign colonic neoplasm, ulcerative colitis/regional enteritis, colon cancer, rectal cancer, diverticulitis, and other. Procedure type was grouped into five categories: Anterior rectal resection, hemicolectomy, total colectomy, sigmoidectomy, and other. Premier's database contains an APR DRG for each patient, as well as an APR DRG severity score. The APR DRGs distinguish among patients using disease- or procedure-specific classes of secondary diagnoses [13]. The APR DRG severity score is a prediction of resource utilization based on discharge abstracts that assigns patients to four levels: 1=minor, 2=moderate, 3=major, and 4=extreme. The severity score can be used to compare patients within the same APR DRG.
Infection was the primary outcome measure of the study; it had to have occurred during the same visit as the colorectal procedure and was identified by ICD-9 code 998.59 (“Other post-operative infection”), as has been used elsewhere in studies employing administrative databases in general and surgical infections in particular [14]. The ICD-9 code 998.59 includes the following post-operative infections: Intra-abdominal abscess, stitch abscess, subphrenic abscess, incision abscess, and “septicemia.” It specifically excludes infections attributable to implanted devices (996.60–996.69); associated with infusion, perfusion, or transfusion (999.3); and post-operative obstetrical incision infection (674.3) [15]. The in-hospital mortality rate and length of stay (LOS) also were measured.
Statistical analysis
Univariable comparisons were conducted using the Student t-test or Wilcoxon rank-sum test for continuous variables and the chi-square or Fisher exact test for categorical variables, with a two-tailed p value of 0.05 being considered significant. Logistic regression with backward elimination (p=0.1 for removal) was conducted, with development of infection as the dependent variable and explanatory variables chosen by the analyst based on significance at univariable analysis or potential as confounders, as suggested in the literature. All analyses were conducted using SAS version 9.1.2 (SAS Institute Inc., Cary, NC).
Results
A total of 16,246 patients with qualifying colorectal procedures had SCIP measures submitted to Premier during the two-year study interval; 15,802 had an APR DRG of 221. A total of 6,180 patients received a single dose of prophylactic antibiotic according to the study criteria. The remainder of the overall cohort either received multiple doses, received an agent not among the six used most frequently, did not receive anaerobic coverage where warranted, or did not have a readily discernable prophylactic antibiotic. Of these, 4,634 patients from 303 hospitals had their antibiotic discontinued within 24 h of surgery and thereby comprised the comparison cohort. The frequency of agent selection among the comparison cohort is displayed in Figure 1. The rate of infection in the overall cohort (n=15,802) was 3.9%; in the comparison cohort of single-dose recipients (n=4,634), the rate of infection was 3.7%.

Frequency of prophylactic agent selection for 4,634 subjects undergoing colorectal procedures.
Patient characteristics
The comparison cohort was 47.5% male and 72.8% white and had a median age of 67 years (range, 18
Surgical characteristics
By admission type, 4,606 of the 4,634 procedures were classifiable as elective (80.9%), urgent (8.2%), or emergency (10.9%). The indication for surgery, in descending order of frequency, was colon cancer (41.8%), benign colonic neoplasm (23.8%), other—e.g., vascular insufficiency of intestine, fistula, etc.—(13.3%), rectal cancer (12.6%), diverticulitis (5.1%), and ulcerative colitis/regional enteritis (3.5%).
The median duration of surgery was 2.8 h (range, 0.3
Univariable analysis
The rate of post-operative infection by prophylactic antibiotic is presented in Table 1. Unadjusted rates differed significantly by agent (p=0.04). The unadjusted rate of post-operative infection also differed significantly by sex (male 5.1%; female 2.5%; p<0.01); admission type (elective 3.4%; urgent 4.8%; emergency 5.4%; p=0.04); procedure type (anterior rectal resection 5.2%; sigmoidectomy 3.8%; hemicolectomy 3.0%; total colectomy 2.2%; and other 5.4%; p=0.01); duration of procedure (<3.5 h 2.8% vs. >3.5 h 6.1%; p<0.01), and APR DRG severity score (minor 1.3%; moderate 2.2%; major 9.0%; extreme 20.6%; p<0.01). The rate of infection did not differ significantly by indication (p=0.30), nor by measured comorbidities other than gender (p>0.1 for all).
Unadjusted comparison showed rates differed significantly among categories (p=0.04).
The prophylactic agent selected differed significantly by indication (p<0.01), but not by procedure type (p=0.61). The agent selected also differed by APR DRG severity score (p<0.01). The agent did not differ by duration of procedure greater than or less than 3.5 h (p=0.89), nor by duration measured as a continuous variable (p=0.72). However, the procedure was significantly longer for those who developed an infection than for those who did not for certain agents: Ertapenem (p<0.01), cefazolin (p=0.04), and cefoxitin (p<0.01). Among infected subjects only, the median duration of the procedure (in hours) did not differ significantly by agent (p=0.19): Ertapenem 3.9, cefazolin 3.5, cefotetan 3.4, cefoxitin 3.3, levofloxacin 3.0, and ampicillin–sulbactam 2.9. Figure 2 displays the duration of the procedure for subjects who did or did not develop an infection according to the prophylactic agent given.
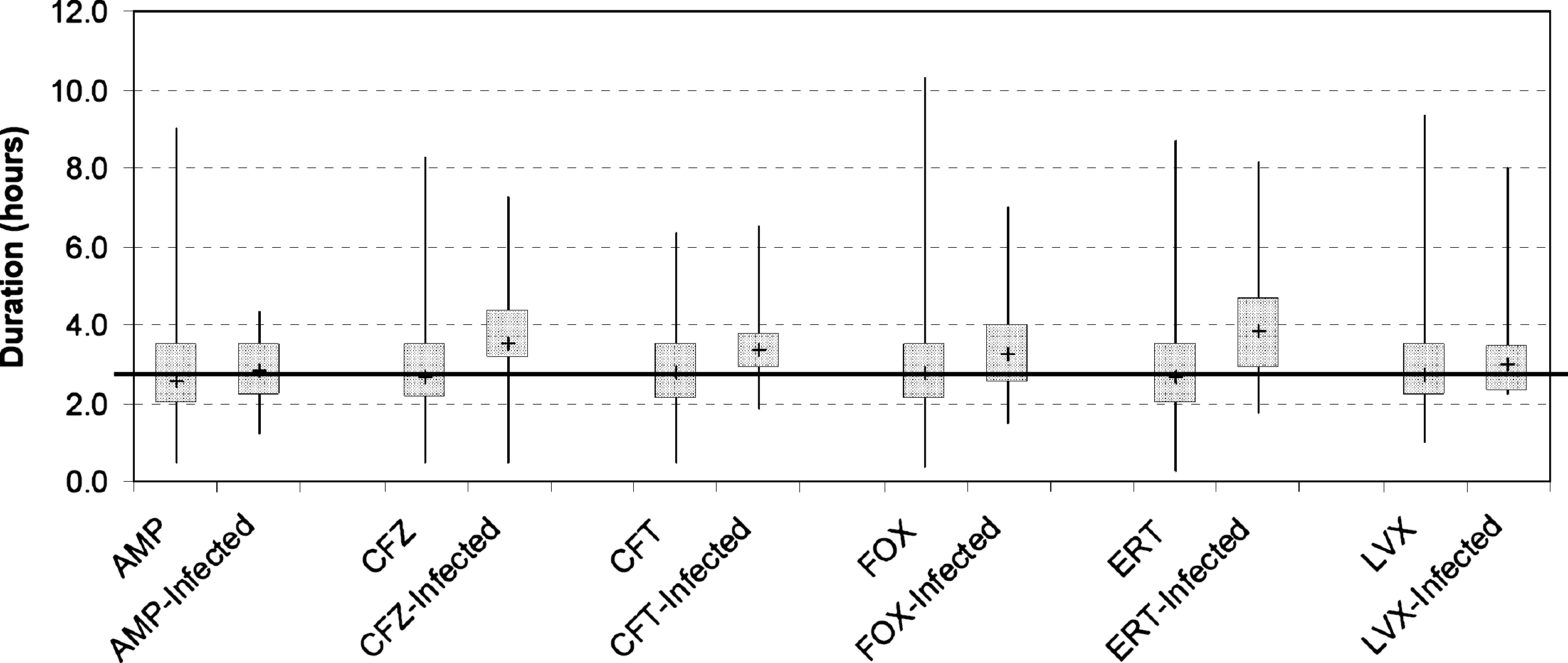
Duration of procedure for 4,634 subjects undergoing colorectal surgery according to prophylactic agent and post-operative infection status. Plus mark indicates median duration for specified agent/infection status group; whisker ends mark minimum and maximum duration; and bar ends indicate first and third quartiles. Horizontal line marks median procedure duration for entire cohort (2.8 h). First bar in each agent-specific pair is subjects who did not have a post-operative infection; second bar is those who did. Abbreviations: AMP=ampicillin/sulbactam (n=447); CFZ=cefazolin (n=549); CFT=cefotetan (n=318); FOX=cefoxitin (n=1,752); ERT=ertapenem (n=1,166); LVX=levofloxacin (n=402).
The in-hospital mortality rate was 1.5% overall and was significantly higher for those who developed infections than for those who did not (5.3% vs. 1.3%; p<0.01; comparison unadjusted). The unadjusted mortality rate also differed significantly (p=0.05) between prophylactic agents (in descending order of mortality rate: Cefotetan 0; cefazolin 0.9%, cefoxitin 1.4%, ampicillin–sulbactam 1.6%, ertapenem 1.7%, and levofloxacin 2.7%). The unadjusted mean LOS after the day of procedure was 5.9 days overall and was significantly longer for subjects who developed infections than for those who did not (15.2 vs. 5.5 days; p<0.01).
Multivariable analysis
Logistic regression with backward elimination (p=0.1 for removal) was conducted with development of infection as the dependent variable and the following as explanatory variables: APR DRG severity score, duration of surgery, age, procedure type, admission type, sex, race, COPD, diabetes mellitus, receipt of prophylactic agent within 1 h of incision, and selection of prophylactic agent, plus interaction terms for prophylactic agent and both severity score and duration of surgery. For prophylactic agent, the most frequently selected compound, cefoxitin, was used as the reference category. For procedure type, hemicolectomy was used as the reference.
The resulting model displayed adequate fit (c=0.80; Hosmer and Lemeshow goodness of fit p=0.88), but low explanatory power (max-rescaled R2=0.17). The variables remaining in the logistic regression model after elimination are displayed in Table 2, with odds ratios (ORs) and their 95% CIs. Although emergency and urgent cases are likely to have higher rates of infection, the investigators desired to retain these subjects in the study because they are given similar agents for prophylaxis. Because admission type did not remain in the multivariable model after backward elimination, the investigators forced it in; it did not affect the results. As a further check, the backward elimination model was re-run using only elective cases. The resulting model retained the same variables and displayed similar fit and explanatory power as the full model. Odds ratios were not meaningfully different, and CIs yielded no differences in significance. As such, the results of the full model are reported herein.
Max-rescaled R2=0.17; Hosmer and Leme show goodness of fit p=0.88; c=0.80).
Odds ratio for continuous variables (age and duration of procedure) corresponds to a 1 log increase in value.
Listed in order of frequency of selection, with cefoxitin being the most frequent and therefore the reference category.
Included patients who received cefazolin or levofloxacin also received metronidazole.
APR DRG=All-Patient Refined Diagnosis-Related Group.
Discussion
Although antibiotic prophylaxis in colorectal surgery is routine and relatively widely studied, unresolved questions remain. Because the development of SSI can be a serious event for the patient, each of the many contributing factors is worthy of improvement. Our earlier study of infection in colorectal surgical patients at our own institution found an attributable cost of developing an infection of $8,591 and an attributable LOS of 4.1 days; as such, even a modest reduction in infection rates in these common procedures could yield both substantial benefit to the patient and substantial savings for the institution [3].
The present study retrospectively evaluated the development of post-operative infection in patients undergoing colorectal surgery who received a single dose of one of six commonly used prophylactic agents. By accounting for the duration of the procedure and other factors influencing infection, we hoped to discern possible differences among agents with different concentration–time profiles. Where possible, we also accounted for variables that might influence the choice of agent prior to surgery. A multiple regression model found that several of our measured variables raised the odds of infection, including duration of procedure and severity of illness. These findings are consistent with the literature. In addition, the model found that use of ertapenem as the prophylactic agent (vs. the most commonly used agent, cefoxitin) yielded significantly lower odds of infection. Although the outcomes of infection were not the focus of the study, we did observe significant increases in both the mortality rate and the LOS at the univariable level of comparison between subjects who developed infection and those who did not.
The Draft Guidelines state that a single 2 g intravenous dose of either cefoxitin or cefotetan given within 60 min prior to incision is recommended (with consideration given to cefazolin plus metronidazole for cost reasons). However, they point out that studies of single-agent therapy with second-generation cephalosporins with activity against anaerobic species—including cefoxitin and cefotetan—yielded a wide range of infection rates (0
An additional route for further inquiry suggested by our data concerns the relation of procedure duration to prophylactic antibiotic selection. Subjects who received cefazolin, cefoxitin, or ertapenem who developed infection had significantly longer procedures than those dosed with the same agents who remained infection free, whereas those receiving other compounds did not. Further, among subjects who did develop an infection, duration was longest for ertapenem (3.9 h) and cefazolin (3.5 h), although the median duration did not differ significantly among agents overall. Although these findings are unadjusted for confounding variables, the multivariable model still found lower odds of infection with ertapenem (and nearly so with cefazolin) and higher odds with longer procedure duration. This pattern suggests that duration plays a larger role in infection development for some compounds than for others. This could be a result of variables not measured directly in our study, such as differing minimum inhibitory concentrations of the infecting organisms to different agents.
With regard to ertapenem, the Draft Guidelines note its indication for prophylaxis but recommend against routine use “due to concerns regarding increases in resistant organisms and potential increase in adverse events.” This statement may refer to concern that use of ertapenem, which lacks activity against Pseudomonas aeruginosa and Acinetobacter spp., may select in those species cross-resistance to other carbapenems. Our group has investigated this phenomenon in a multi-center study, where we found no relation between ertapenem use and increased carbapenem resistance in P. aeruginosa [16]. Those findings are similar to reports from single-center studies [17,18]. Because the results of the present study suggest an advantage to ertapenem, in patients or institutions where the prevalence of infection with the above species is low, the advantage of additional protection from SSI in colorectal procedures might reasonably be weighed against resistance concerns.
Our study contains important assumptions and limitations. Perhaps the most significant limitation is that our outcome measure (post-operative infection indicated by ICD-9 code), although used elsewhere to identify SSIs, does not distinguish between incisional and organ/space infection [14]. The implications for the patient certainly are more serious with deep infection.
Although the overall infection rate reported here is similar to that found in our earlier study at our institution (3.9% in the overall [i.e., not just single-dose] cohort vs. 4.1% in the earlier study), readers will note that these rates are low compared with those reported in some prospective clinical trials [3]. There are several reasons this may be so. Such trials may have longer follow-up periods, may include incisional infections, or may classify non-infectious outcomes as “antibiotic failure.” A 1998 systematic review of randomized controlled trials of antimicrobial prophylaxis in colorectal surgery reported an overall infection rate of 11%; however, this analysis preceded the implementation of the program that became SCIP, which may have influenced protocols even among non-participating institutions [19]. Indeed, only SCIP patients were included in our cohort. A recent study using the same data source (although an earlier time period and focusing only on elective colectomies) reported an overall infection rate of 3.4% (n=32,733 patients) [20].
The study contains an implied assumption that the proportion of laparoscopic procedures was equal among the prophylactic agents, as we were not able to distinguish laparoscopic from open procedures, and laparoscopic techniques result in better outcomes [21]. It is possible that some surgeons favor one agent or another when an open procedure is planned; however, we believe this limitation to be somewhat mitigated by having controlled for both severity of illness and duration of procedure. Further, our results would be affected only if such preferences were systematically in favor of (or against) a particular agent. Similarly, intra-operative incidents such as perforation or spillage may influence the development of infection, and these cannot be discerned in administrative data; the study therefore contains an implicit assumption that such incidents occurred with equal frequency among patients given different agents. We also could not adjust for surgical site preparation; clorhexidine–alcohol recently was shown to be superior to povidone
We did not account for oral antibiotics given on the day of procedure; recent studies have shown that such antibiotics do not provide additional benefit in the presence of appropriate parenteral antibiotics, suggesting that the parenteral drug is causing the observed prophylactic effect [19,23]. The Draft Guidelines consider the optimal use of oral vs. intravenous vs. oral plus intravenous regimens to be unresolved but recommend supplementing the intravenous agent with an oral agent in the case of high-risk procedures—specifically, rectal resection. We did control for procedure type in the multivariable regression model, which may mitigate this factor. Lastly, we were unable to account for other practices that may influence the development of SSI, including infection control and after-care practices that may be hospital–specific. However, because the study subjects were contributed by more than 300 hospitals and were thinly distributed among them, we believe that no individual hospital's practices influenced the results unduly.
Conclusion
Our investigation identified choice of prophylactic agent as an independent predictor of post-operative infection in colorectal surgery patients, while controlling for other potential risk factors for infection and confounders for agent selection. There may be important factors that were unmeasured by our study, as development of post-operative infection can be influenced by infection control practices, surgical skill, etc. However, our findings suggest that careful attention should be paid to agent selection and that further research on prophylactic agents and dosing strategies remains necessary.
Footnotes
Acknowledgments
This study was supported by a grant from the Research Program at Hartford Hospital and internal funds from the Hospital's Center for Anti-Infective Research and Development. Data supporting the study were obtained from Premier, Inc. (Charlotte, NC).
Author Disclosure Statement
DPN has received research support from, and serves as a consultant and on speakers' bureaus for, Merck & Co. and Ortho McNeil Pharmaceuticals. KJE reports no conflicts.