KrzyzaniakMichael JMDPetersonCarrie YMDLoomisWilliam HBSKennedyVinceBansalVishalMDEliceriBrianPhDBairdAndrew NPhDCoimbraRaulMD, PhDPutnamJames GBS
Naval Medical Center San Diego
MAINTENANCE OF THE GUT EPITHELIAL BARRIER VIA VAGAL NERVE STIMULATION PROTECTS AGAINST SECONDARY PULMONARY INJURY AFTER THERMAL INJURY
Background: We have previously shown that vagal nerve stimulation protects the intestinal epithelial barrier by maintaining the integrity of tight junction proteins following a thermal insult. We have also shown that acute lung injury is prevented when protective strategies to the gut mucosa are employed. The link between prevention of acute lung injury by maintaining the gut barrier has yet to be investigated. We hypothesize that maintenance of the gut epithelial barrier via vagal nerve stimulation and its action on the enteric nervous system prevents the subsequent systemic inflammation and attenuates acute lung injury.
Methods: Balb/c mice were subjected to 30% TBSA burn with and without electrical stimulation directly to the cervical right vagus nerve. Histology, myeloperoxidase (MPO), NFkB, and ICAM-1 immune staining, MPO enzymatic assay, Lung IL-8 levels (ELISA) were performed. Additionally, Lung NF-kB and IkBα immunoblots as well as NF-kB activation measured by photon emission analysis (Ivis Lumina Xenogen) using NF-kB luc transgenic mice were performed. Lung Histology (H&E) was performed at 6 and 24 hours post burn.
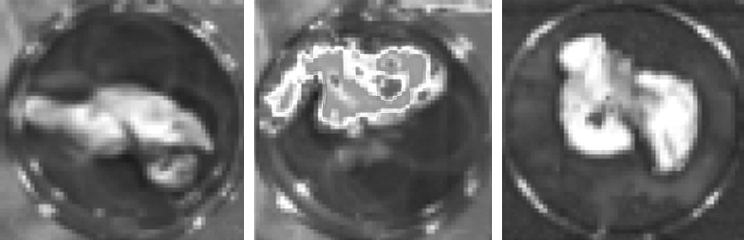
Results: At 6 hours post burn, an increase in phosphorylation of both NF-kB p65 and IkBα were observed. These findings coincide with increased photon emission signal in the lungs of the NF-kB luc transgenic animals. Vagal nerve stimulation blunted NF-kB activation to levels similar to sham animals. MPO positive cells were increased in the lung at 24 hours post burn. Similarly, ICAM-1 expression was up regulated in the lung endothelium at 24 hours. Lung histology demonstrated significant pulmonary edema, intra-alveolar hemorrhage and intra alveolar hyaline membrane formation at 24 hours. Vagal nerve stimulation markedly decreased neutrophil infiltration in the lung demonstrated by MPO immune staining and enzyme activity. More importantly, vagal nerve stimulation markedly attenuated acute lung injury at 24 hours (lung injury score similar to sham animals).
This picture demonstrates increased photon emission from transgenic NFkB-luciferase mice as a result of burn injury at 6 hours (picture sequence: Sham, 6 hour burn, 6 hour burn with vagal stimulation). Vagal nerve stimulation reduces the NFkB activity thereby decreasing the expression of the luciferase gene and decreasing the signal.
Conclusion: Vagal nerve stimulation affects the enteric-pulmonary axis by maintaining the integrity of the epithelial gut barrier. Vagal nerve stimulation markedly attenuates lung injury by down regulating NF-kB activation and neutrophil recruitment in the lung.
VogelTodd RMD, MPHDombrovskiyViktor YMD, MPH, PhDLowryStephen FMD
UMDNJ-Robert Wood Johnson Medical School
DELAY OF ELECTIVE SURGERY FOR HIGH VOLUME PROCEDURES: THE IMPACT ON INFECTIOUS COMPLICATIONS
Introduction: The development of infectious complications after high volume elective surgical procedures imposes a significant clinical burden to the United States population. This study evaluated the association of delay of elective procedures and the subsequent impact on infectious complications after coronary artery bypass graft (CABG) surgery, colon resection, and lung resection. Infectious complications evaluated included pneumonia (PNA), urinary tract infections (UTI), postoperative sepsis, and surgical site infections (SSI).
Methods: The Nationwide Inpatient Sample was queried between 2003–2007 and patients that developed postoperative infectious complications were identified. Time to elective surgery in days from admission was calculated and the following delayed groups were created: 0, 1 day, 2–5 days, and 6–10 days. Patients with a surgery delay of more than 10 days (less than 1% of all cases) were excluded. Chi square, multivariable logistic regression analyses, and Cochran-Armitage trend test were utilized.
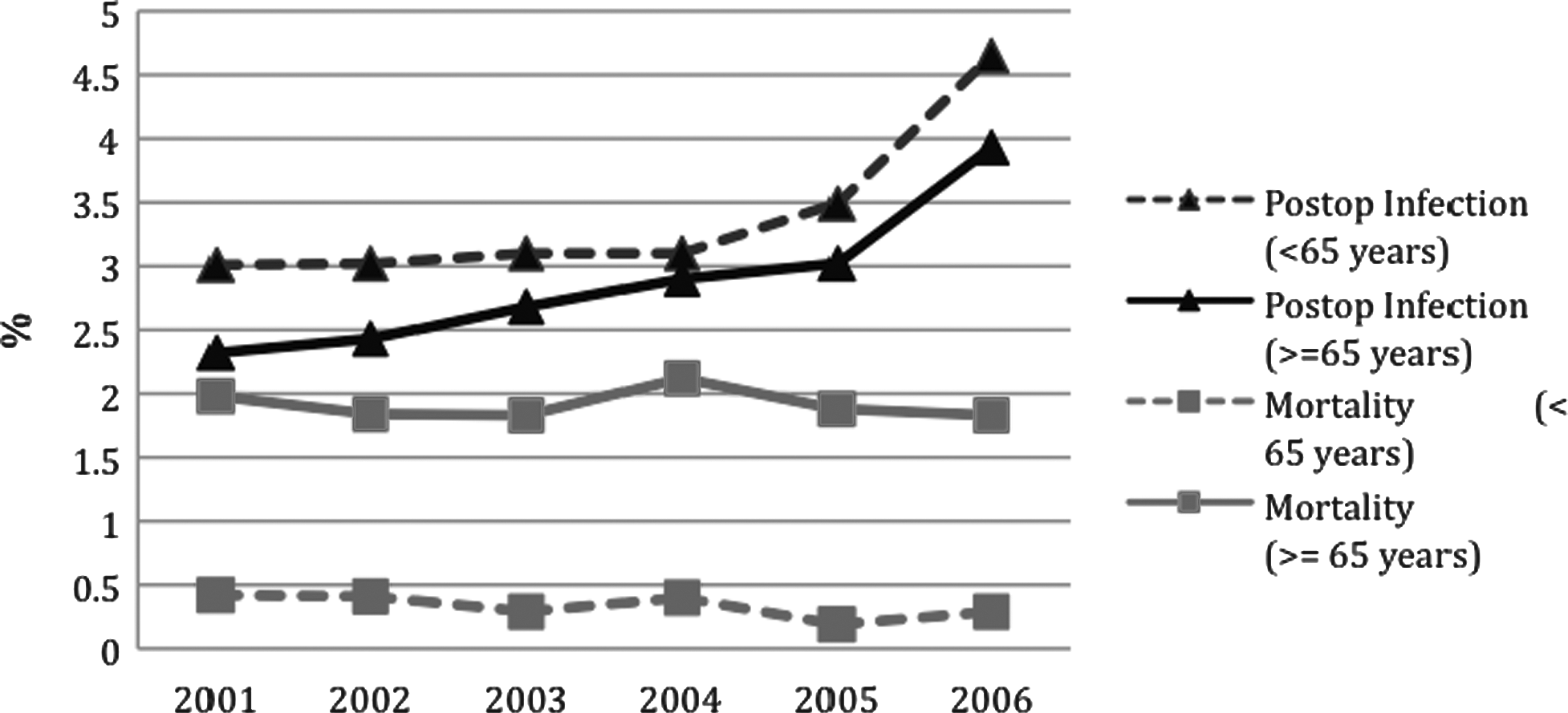
Results: 87,318 CABG procedures, 46,728 colon resections, and 28,960 lung resections were evaluated (non-weighted values). Total infection rates significantly increased after elective surgery delays: CABG: 0 = 5.73%; 1 = 6.68%; 2-5 = 9.33%; 6-10 = 18.24%; Colon Resections: 0 = 8.43%; 1 = 11.86%; 2-5 = 15.79%; 6-10 = 21.62%; and Lung Resections: 0 = 10.17%; 1 = 14.53%; 2-5 = 15.53%; 6-10 = 20.56%, p < .0001 for all trends. Trends for increasing infections after delay were significant for PNA and sepsis for all procedures (P < 0.0001); UTI and SSI significantly increased after CABG and colon resection. Adjusted by age, gender, race, and comorbidities, the odds ratios of developing postoperative infection by delay from admission were calculated (graph above). Mean cost increased after all procedures with delays: CABG: $36,079 vs. $47,527 (p < .0001), Colon Resections: $20,265 vs. $29,887 (p < .0001), and Lung Resections: $26,323 vs. $30,571 (p = 0.0032).
Adjusted odds ratios of Developing Postoperative Infection by Delay from Admission. Error bar = 95% confidence interval.
Conclusions: Delay of elective surgery from the day of admission was associated with a significant increase in infectious complications. This delay was also associated with a significant increase in hospital cost and utilization. Future policy directed toward preventing delay of elective surgery could offer significant cost savings and decrease infectious complications after elective surgery.
EmamiClaudia NMDMittalRahulPhDNemaniPrasdarao VPhDFordHenri RMD, MHA, FACS
Childrens Hospital Los Angeles, USC Department of Surgery
THE ROLE OF DENDRITIC CELLS IN ENTEROBACTER SAKAZAKII-INDUCED DISRUPTION OF THE EPITHELIAL CELL BARRIER: IMPLICATIONS FOR THE PATHOGENESIS OF NEC
Introduction:Enterobacter Sakazakii (ES) is a rare and virulent pathogen that has been associated with outbreaks of necrotizing enterocolitis (NEC) in neonates. Our previous studies have shown that ES expressing outer membrane protein A (OmpA) induces NEC in neonatal rats by triggering enterocyte apoptosis. Intestinal dendritic cells (DCs) play a key role in luminal antigen sampling and alert other leukocytes in the lamina propria to the presence of pathogenic bacteria. However the role of DCs and their interaction with bacteria has not been explored in NEC. In this study, we investigate the role of DCs in ES-induced disruption of the intestinal epithelial barrier; the first step in the pathogenesis of NEC.
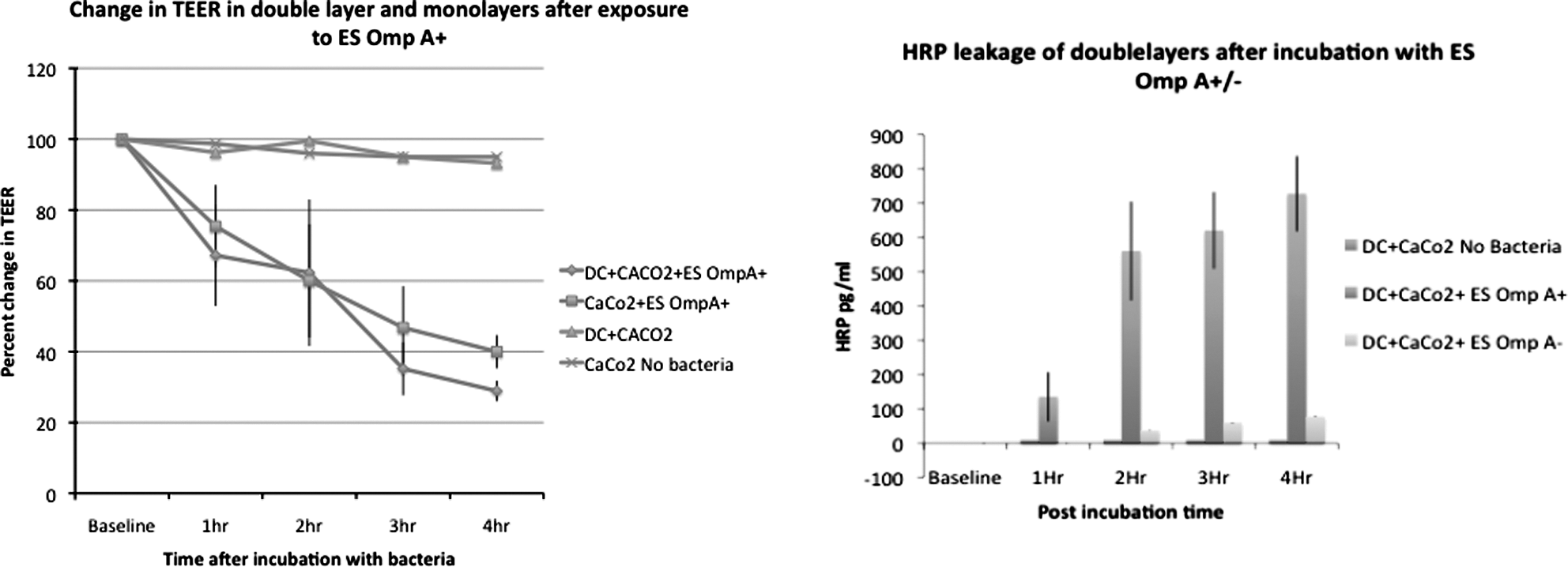
Methods: To mimic the presence of DCs at the basement membrane of the intestine, double layers of CaCo2 cells and bone marrow-derived DCs (BMDCs) were developed using trans-wells. CaCo2 cells were seeded in the upper side of the trans well chamber while BMDCs were seeded at the bottom of the porous membrane and cultured for 24 hours. In addition, BMDCs were cultured for 24 hours with OmpA + ES or OmpA− ES, and the supernatants were collected. The cytokine levels in these supernatants were measured using ELISA. The permeability of the double layer after treatment with OmpA + or OmpA- ES was measured using trans-epithelial electrical resistance (TEER) as well as HRP leakage at one-hour time intervals up to 4 hours. These measurements were compared to the permeability of CaCo2 monolayers treated only with the bacteria as well as the monolayers pretreated with BMDC/ES co cultures supernatants and subsequently treated with ES.
Results: Presence of BMDCs in the double layer model exacerbates the effects of ES on barrier permeability as demonstrated by a faster decrease in the TEERs as well as HRP leakage (Figures 1, 2). Similarly the decrease in TEER is greater when the monolayers are pretreated with OmpA+ , but not OmpA− DC/ES co-culture supernatants. Absence of OmpA protein dampens the effect of ES on the double layers as well as pretreated monolayers. The bacterial lysate does not show the same effect on the monolayers as the co-culture supernatants. Interaction of ES with BMDCs suppresses the production of pro-inflammatory cytokines (TNFα and IL-6), but increases the levels of anti-inflammatory cytokines (IL-10 and TGF-β). Preliminary data show that addition of anti-TGF-β Antibody in the co-cultures protects barrier function.
Conclusions: Interaction of ES with DCs causes disruption of the epithelial barrier by inducing cytokine production, which exacerbates the damage to the tight junctions caused by ES. Presence of OmpA is necessary for the deleterious effects of ES on intestinal epithelial barrier permeability.
MonaghanSean FMDHeffernanDaithi SMD, AFRCSIThakkarRajan KMDReinertSteven EMachanJason TPhDGreggSheaMDKozloffMatthew SMDConnollyMichael DMDAdamsCharles AMDCioffiWilliam GMD, FACS
Brown University, Rhode Island Hospital
URINARY TRACT INFECTIONS SIGNIFICANTLY WORSEN OUTCOMES IN TRAUMA PATIENTS: AN ANALYSIS OF 8,841 PATIENTS
Background: In October 2008, the Centers for Medicare and Medicaid Services stopped paying for care associated with catheter-related urinary tract infections. Since that time, there has been a huge push for decreased use of Foley catheters in order to decrease hospital acquired urinary tract infections (UTI). No direct evidence exists correlating a negative impact from the presence of a UTI. This study describes the impact of a hospital-acquired urinary tract infection on a trauma patient.
Methods: All trauma patients from 2003 to 2008 were included in this IRB-approved study if they survived past a three-day hospital stay. All available urinalysis and urine cultures were reviewed for these patients. A positive urinary tract infection was defined as either the presence of >5 WBCs, or leukocyte esterase on urinalysis or a positive urine culture. The medical chart was reviewed for injury severity score, specific body site injury scores, mechanism of injury, age, and gender. Primary outcome measure was hospital length of stay but it also included ICU stay, ventilator days, and mortality. Kaplan-Meier curves, Chi square and Student's t-test were applied to the data.
Results: Over this period, 8841 patients were admitted to the trauma service, with 6145 patients accounting for 17,924 urinalyses sent and 2494 patients accounted for the 6756 urine cultures. 5751 patients stayed longer than three days, of which 683 patients had a UTI. The length of stay in a patients with a UTI was 26.7 days compared to 9.5 days (p ≤ 0.001). Patients who had a UTI have a significantly higher ISS (17.7 vs 12.2, p ≤ 0.001). When patients were divided into groups based upon ISS (<15, 15–25, and >25) and censored for death, all groups had significantly longer length of stay if the patient developed a UTI. For those with mild injury (ISS < 15), the median length of stay was 5 days (95% CI = 4.9-5.2) which increased to 12 days (95% CI = 10.6-13.4) if the patient had a UTI. In moderately injured patients (ISS15–25), the median stay was 7 days (95% CI = 6.6–7.4), which increased to 21 days (95% CI = 17.7-24.3) in the presence of a UTI. In severely injured patients (ISS > 25) the median stay was 14 days (95% CI = 12.5-15.5), but a UTI increased median length of stay to 35 days (95% CI = 29.4-40.6) Within mild and moderate ISS groups, mortality was also significantly increased in the presence of a UTI. (mild 6.8 versus 1.1, p ≤ 0.001; moderate 11.7 versus 5.2, p = 0.003).
Conclusion: This is the first description of the impact of a UTI on hospitalized trauma patients. When accounting for death and across all ISS, trauma patients who acquire a UTI while in the hospital extend their hospital length of stay. Furthermore the presence of a UTI independently negatively impacts the mortality of trauma patients, however the degree of cause and effect versus an association needs further delineation. In light of these findings, it is apparent that all available means to prevent UTI in trauma patients should be employed.
NealMatthew DMDSodhiChhinder PPhDRichardsonWard MMDAfraziAminBSSiggersRichardPhDHackamDavid JMD, PhD
Division of Pediatric Surgery, Department of Surgery, University of Pittsburgh Medical Center
TLR4 INDUCED AUTOPHAGY INCREASES BACTERIAL INTERNALIZATION BY ENTEROCYTES
Introduction: We have recently identified a critical role for the LPS receptor, Toll-like receptor 4 (TLR4) in the pathogenesis of intestinal inflammation, and we have shown that enterocytes are capable of TLR4 mediated internalization of Gram-negative bacteria (SIS 2004). The cellular processes that mediate internalization of bacteria are unknown. TLR4 has recently been shown to be an environmental sensor for autophagy in macrophages, and autophagy has been shown to be critical in the processing of internalized bacteria by epithelial cells. We now hypothesize that enterocytes undergo TLR4 induced autophagy and that autophagy plays a role in processing of internalized bacteria.
Methods: Enterocytes lacking the ability to undergo autophagy were engineered using siRNA to the critical autophagy gene, ATG16 (ATG16−/−). TLR4 knock-out cells were generated with shRNA (TLR4−/−). Wild-type intestinal epithelial cells (IEC-6), TLR4−/−, and ATG16−/− were pre-treated with the autophagy inducer, rapamycin (50 nmol/L, 18 hrs), the TLR4 agonist, LPS (25 ug/ml, 18 hrs) and the autophagy inhibitor, chloroquine (10 uM, 3 hrs). To assess for internalization, cells were incubated with E. coli that were pre-labeled with green fluorescence and biotin. Following internalization (2hrs, 37C), cells were incubated with rhodamine-streptavidin to distinguish bound bacteria (red and green) from internalized (green alone). Quantification of internalization was performed by flow cytometry and confocal microscopy. Immunofluorescence was performed for the autophagosome marker, LC3 using anti-LC3 antibodies. IEC-6 cells transfected with mCherry-LC3 were incubated with LPS-coated latex beads and imaged using live-cell fluorescent microscopy.
Results: Activation of TLR4 with LPS increased LC3 expression in IEC-6 cells demonstrating that TLR4 activation leads to autophagy in enterocytes. IEC-6 were capable of internalizing E. coli, confirming our earlier findings (SIS 2004). Strikingly, activation of autophagy with both rapamycin and LPS increased internalization (control 11.5, rapa 18, LPS 16.7, p < 0.05, recorded as % internalization). Inhibition of autophagy with chloroquine did not significantly change internalization (11.7 vs. 11.5, p = 0.71). Enterocytes deficient in autophagy (ATG16−/−) were able to internalize but had no change with rapamycin, LPS, or choloquine (control 11.8, rapa 11.1, LPS 11.6, p = NS). Internalization was significantly inhibited in TLR4 knock-out cells with no increase after stimulation of autophagy (control 10.6, TLR4−/− 0.9, rapa-TLR4−/− 1.1, LPS-TLR4−/− 0.7, p < 0.01), indicating the critical role for TLR4. LC3 was found to co-localize with E. coli and LPS-coated beads, indicating that autophagosomes form around internalized bacteria.
Conclusion: These data prove a novel and unexpected link between TLR4 activation and autophagy in enterocytes leading to the internalization of gram-negative bacteria. This new paradigm linking autophagy with bacterial internalization may have broad implications in our understanding of the factors leading to the regulation of intestinal inflammation and systemic sepsis.
AminParth BMDMagnottiLouis JMDFischerPeter EMDCroceMartin AMDFabianTimothy CMD
Presley Trauma Center, University of Tennessee, Memphis
PROPHYLACTIC ANTIBIOTIC DAYS AS A PREDICTOR OF SENSITIVITY PATTERNS IN ACINETOBACTER PNEUMONIA
Introduction: Ventilator-associated pneumonia (VAP) secondary to Acinetobacter spp. in critically-ill trauma patients has increased. More importantly, the incidence of multi-drug resistant (MDR) Acinetobacter VAP has also increased. Still, the risk factors associated with this increased resistance have yet to be elucidated. The purpose of this study was to evaluate the change in Acinetobacter sensitivity over time and determine which risk factors predict resistance in trauma patients.
Methods: Patients (surviving >5 days post-injury) with Acinetobacter VAP (≥105 CFU/mL in BAL) over 5 years were divided based on pathogen sensitivity (sensitive [SEN] vs MDR) and stratified by age, severity of shock (BE, blood transfusions), injury severity (ISS, admission GCS, chest and extremity AIS) and year. Empiric (E), prophylactic (P), E + P and total antibiotic days, ventilator days and mortality were compared. Multivariable logistic regression (MLR) was performed to determine which risk factors were independent predictors of resistance
Results: 96 patients (81% men) were identified: 62 SEN and 34 MDR. Groups were clinically similar in terms of age, shock and injury severity with the exception of ext AIS (Table). Antibiotic exposure was also increased in the MDR group (Table). The incidence of MDR Acinetobacter VAP increased from 0 to 66% (p < .0001) over the study.
E
P
Total
Ext AIS
SEN
2.5
1.7
15
1.4
MDR
1.8
6.9
26
2.2
P
.052
<.0001
.0001
.01
MLR identified P antibiotic days as an independent predictor of MDR in patients with Acinetobacter VAP after adjusting for age, chest AIS and year (OR = 1.94, p < .0001).
Conclusion: The incidence of MDR Acinetobacter VAP has increased over time. Increased extremity AIS may have contributed to unnecessary prolonged antibiotic exposure in those patients with MDR Acinetobacter VAP. In fact, MLR identified prophylactic antibiotic days as an independent risk factor for MDR Acinetobacter VAP in trauma patients.
RomanowskiKathleen SMDZaborinAlexPhDValuckaiteVestaMDBabrowskiTrissa AMDFinkDavidMDMorozovaIrinaMSLiuDonald CMD, PhDMatthewsJeffery BMDZaborinaOlgaPhDAlverdyJohn CMD
University of Chicago
EVIDENCE THAT LETHAL GUT-DERIVED SEPSIS DUE TO CANDIDA ALBICANS IN MICE IS DEPENDENT ON THE LOCAL CONCENTRATION OF PHOSPHATE
Background: Our laboratory has demonstrated that lethal gut-derived sepsis in mice due to P. aeruginosa is dependent on the local concentration of phosphate owing to the presence of a highly conserved phosphoregulatory system in this pathogen that detects low phosphate and activates its quorum sensing signaling system. Here we determined if this conserved mechanism of virulence activation can also be demonstrated for the opportunistic fungal pathogen C. albicans which is also known to be a common cause of lethal gut-derived sepsis.
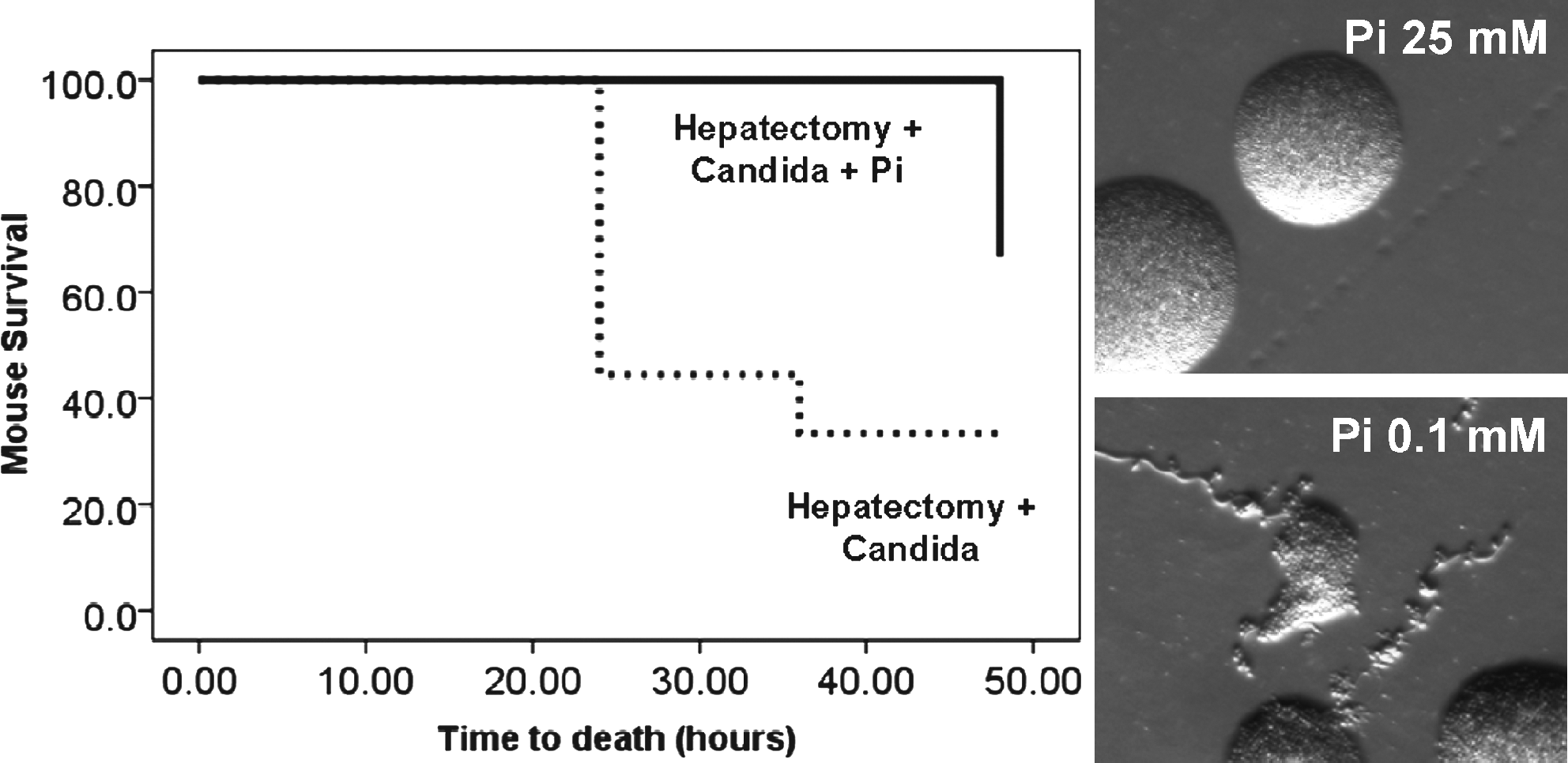
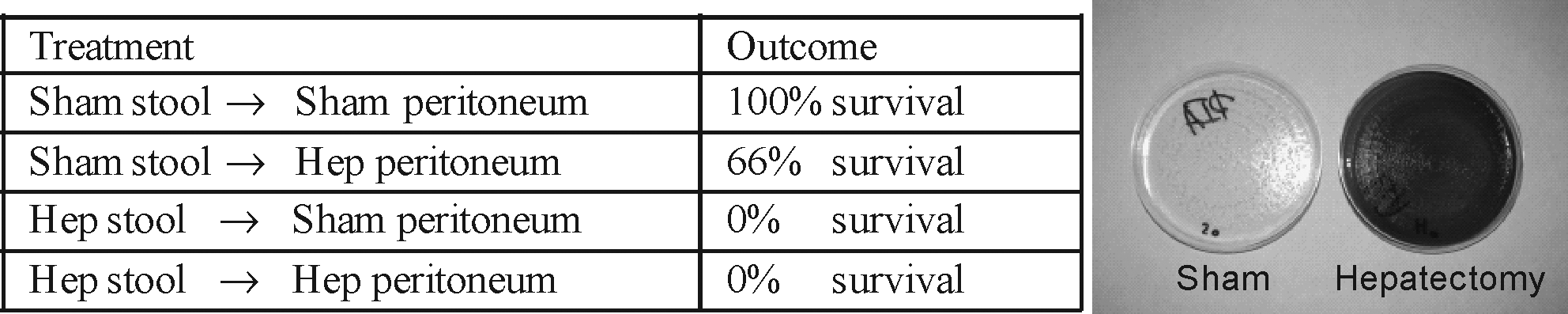
Methods: Hyphae formation, an inducible morphological change known to shift C. albicans to an invasive and virulent phenotype, was assessed using a strain of C. albicans isolated from the stool of a critically ill patient. The strain was examined under phosphate [Pi] limiting conditions using a SZX16 Olympus stereomicroscope. To determine if C. albicans can kill its host when exposed to low phosphate conditions, we injected C. albicans (107 CFU) into the mouse cecum following a 30% hepatectomy, a known model of local intestinal phosphate depletion as well as into similarly operated mice orally replenished of Pi (25mM). Adhesiveness of C. albicans in intestinal tissues from mice was examined between groups by scanning electron microscope (SEM) using a FEI Nova NanoSEM 200 (FEI, USA).
Results:C. albicans grown on agarized media depleted of phosphate was observed to shift to its hyphae-like form (see Figure), a phenotype associated with invasion and dissemination. Mice undergoing 30% and intestinal inoculation of C. alb cans had a mortality rate of 66.6% at 48 hours (n = 9, p < 0.03) whereas mortality in this model decreased to 33.3% (n = 9) when the intestinal tract was phosphate repleted with oral phosphate supplementation. Examination of intestinal tissues by SEM revealed evidence of abundant hyphae among C. albicans present in the phosphate depleted environment of the mouse cecum following 30% hepatectomy with evidence of loss of the normal epithelial architecture. However mice orally supplemented with Pi demonstrated suppression (absence) of hyphae formation among identified C. albicans and preservation of normal intestinal architecture.
Conclusion: These data show for the first time that C. albicans-mediated lethal gut- derived sepsis can be experimentally modeled to occur following surgical injury alone, without pharmacologic immunosuppression and without antibiotic decontamination of the normal flora. In addition we show that C. albicans shifts its morphology in response to surgical injury in a phosphate dependent manner. Taken together, results of this study suggest that maintenance of local phosphate sufficiency may be a novel approach to prevent gut- derived dissemination/sepsis from C. albicans and merits further study.
LeukhardtWilliam HMDCarterJeffrey WMDHaridasManjunathMDInuiTazo SMDMalagoniMark AMD, FACSClaridgeJeffrey AMD, MS, FACS
MetroHealth Medical Center
THE PRESENCE OF SPECIFIC BACTERIAL ORGANISMS PREDICTS MORTALITY IN PATIENTS WITH INTRA-ABDOMINAL INFECTIONS
Background: Intra-abdominal infections (IAI) are a major cause of hospital morbidity and mortality. However, due to the multi-factorial nature of IAI, treatment failure and mortality have been difficult to reliably predict. We hypothesize that specific infecting organisms predict mortality independent of all other patient factors.
Patients and Methods: All patients with non-appendiceal IAI treated at an academic tertiary care facility over 8 years (June 1999–June 2007) were included. Data collected included demographics, comorbidities, source of infection, intra-abdominal culture results, type of infection (community vs nosocomial), type of intervention (operation vs percutaneous drainage), and mortality. Charlson Comorbidity Index and multiple organ dysfunction score (MODS) were evaluated.
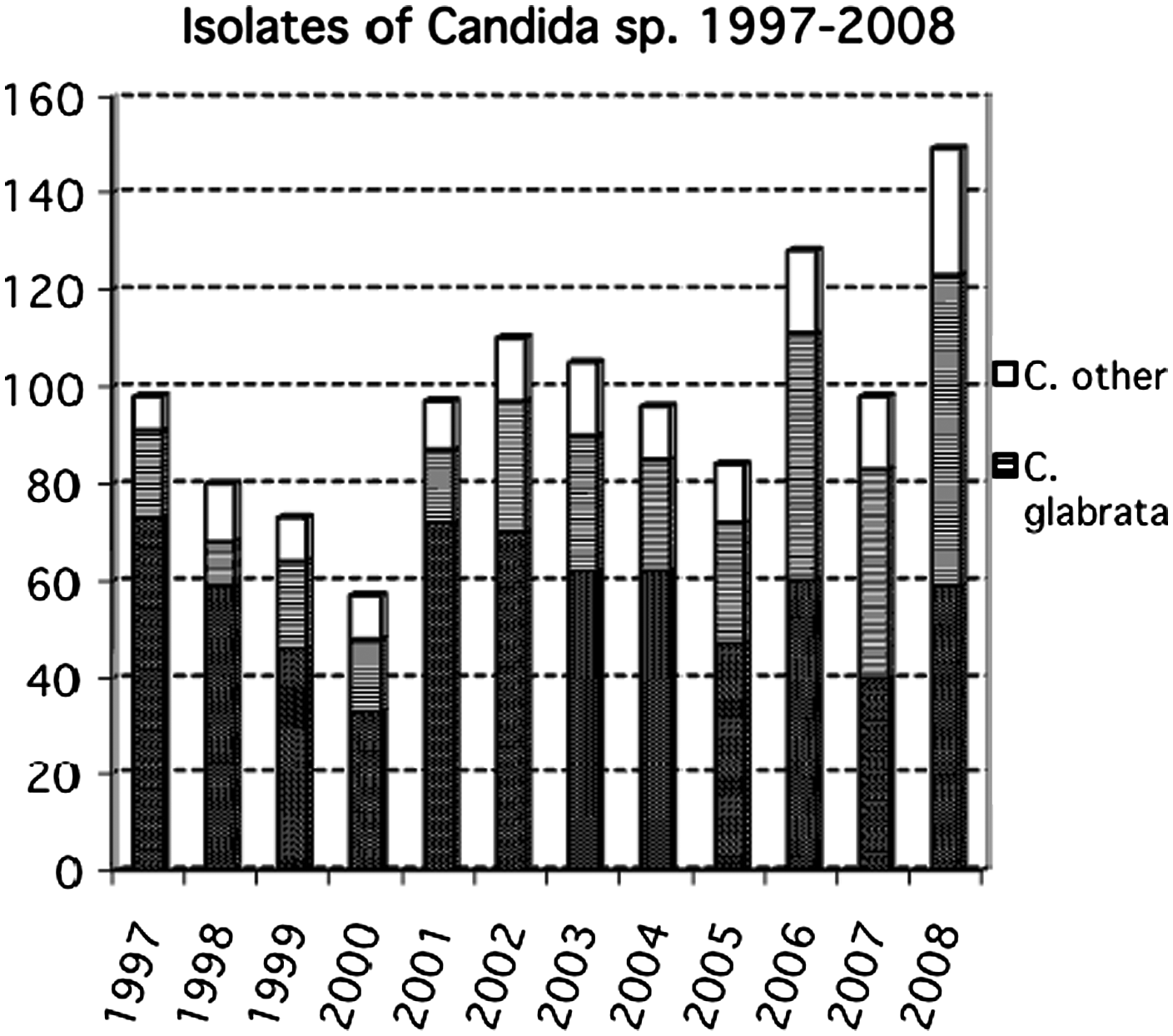
Results: 323 patients had an overall mortality of 8.7%. Intra-abdominal cultures were obtained on 303 (93.8%) patients. The mean age was 54 and 50% were male. The most common etiology of IAI was post-operative infections (44%). There were 49 distinct species isolated. The most common organisms were: Enterococcus species (93), E. coli (75), Pseudomonas aeruginosa (38), Candida albicans (35), and Bacteroides fragilis (34). Twenty-five cultures (8.3%) had no growth, 35.6% grew one organism, 20.1% grew two organisms, 20.1% grew three organisms, 11.6% grew four organisms, 12 (4.0%) grew 5 organisms, and 1 (0.3%) grew six organisms. Bivariate analysis revealed multiple risk factors associated with mortality (see table).
Risk Factors
No Mortality (N = 295)
Mortality (N = 28)
p-value
Age ≥65
26%
61%
<0.001
Charlson score ≥2
23%
68%
0.031
Operative Management
75%
96%
0.008
Vent >72 hours
27%
57%
0.001
Cardiac Event
10%
54%
<0.001
CRBS Infection
12%
54%
<0.001
Pre-op MODS ≥4
21%
43%
0.016
POD#7 MODS ≥4
17%
54%
<0.001
Needed re-intervention
23%
46%
0.01
Pneumonia
17%
39%
0.006
More than one species
55%
63%
NS
Colon Etiology
29%
39%
NS
Bacteroides Species (Non-B. fragilis)
4%
19%
0.008
P. aeruginosa
11%
26%
0.059
Enterococcus (VRE + faecalis + faecium)
10%
30%
0.008
C. perfringens
3%
11%
0.05
Logistic regression demonstrated that independent risk factors for mortality were Age ≥65 (OR = 2.92), cardiac event (OR = 5.50), catheter-related bloodstream infection (OR = 7.63), the presence of Bacteroides species (non-B. Fragilis) (OR = 7.37), and Enterococcus (VRE + faecalis + faecium) (OR = 5.67). The C statistic was 0.89.
Conclusion: These results demonstrate that in addition to age and intrinsic patient factors, the presence of specific bacterial organisms independently predicts mortality in patients with IAI.
CostantiniTodd WMDPetersonCarrie YMDPutnamJames GBSLoomisWilliam HBSRyuSeok YongMD, PhDBansalVishalMDCoimbraRaulMD, PhD
University of California, San Diego School of Medicine
VAGAL NERVE STIMULATION MODULES INTESTINAL TIGHT JUNCTION PROTEIN EXPRESSION THROUGH THE ACTIVATION OF ENTERIC GLIA CELLS
Introduction: Vagal nerve stimulation has been shown to have significant immunomodulatory effects following injury. We have recently shown that vagal nerve stimulation activates enteric glia cells, which are known to play an important role in maintaining gut barrier function. Activated enteric glia cells have been shown to modulate intestinal barrier integrity and tight junction protein expression through secretion of s-nitrosoglutathione (GSNO). We hypothesized that vagal nerve stimulation would decrease burn-induced intestinal barrier injury through modulation of the tight junction proteins myosin light chain kinase (MLCK) and phosphorylated myosin light chain (MLC). We also postulated that injection of GSNO immediately following burn would improve intestinal barrier integrity and modulate tight junction protein expression.
Methods: Male balb/c mice underwent electrical cervical vagal nerve stimulation for 10 minutes prior to 30% total body surface area steam burn. Segments of distal ileum were obtained 4 hours following injury to assess intestinal TNF-α using ELISA, and MLCK protein expression by Western blot. Confocal microscopy was utilized to demonstrate changes in phosphorylated MLC localization. Animals were also given an intraperitoneal injection of GSNO (10mg/kg) immediately following burn. Intestinal barrier integrity was assessed using histology and by measuring in vivo intestinal permeability to 4 kilodalton FITC-Dextran.
Results: Severe burn injury results in a 4-fold increase in intestinal MLCK protein expression, which is associated with elevated gut TNF-α. Stimulation of the vagus nerve immediately prior to burn decreases intestinal MLCK expression to sham levels. There is no difference in intestinal TNF-α between sham and burned animals undergoing vagal nerve stimulation. Confocal microscopy images demonstrate that vagal nerve stimulation attenuates the burn-induced phosphorylation of intestinal MLC. Injection of GSNO following burn injury improved gut barrier function (see Figure), decreased burn-induced histologic gut injury, and was associated with decreased phosphorylation of MLC compared to burn alone.
Conclusion: Vagal nerve stimulation attenuates gut barrier injury following burn by modulating expression of the intestinal tight junction protein MLCK. These results further demonstrate the immunomodulatory effects of vagal nerve stimulation, suggesting a novel mechanism by which activation of enteric glia maintains intestinal barrier integrity following injury through secretion of GSNO.
ZaborinAlexander VPhDRomanowskiKathleenMDMorozovaIrinaMS,BethelCindyMT, (ASCP),BabrowskiTrissaMDOlivasAndreaMDFinkDavidMDFrankKarenMD, PhDLiuDonaldMD, PhDZaborinaOlgaPhDAlverdyJohn CMD
University of Chicago
INTESTINAL PHOSPHATE DEPLETION DEVELOPS DURING HUMAN CRITICAL ILLNESS AND ACTIVATES THE VIRULENCE OF KEY COLONIZING PATHOGENS ASSOCIATED WITH GUT-DERIVED SEPSIS
Introduction: We previously demonstrated that phosphate [Pi] depletion develops within the mucus layer of the distal intestine in mice during surgical injury and activates a lethal phenotype in Pseudomonas aeruginosa via conserved phosphate response regulation. The aims of the present study were to determine whether other intestinal pathogens also activate their virulence in response to [Pi] depletion and to determine if they display molecular evidence of exposure to [Pi] depletion in vivo.
Methods: Stool samples were consecutively collected from 12 ICU patients yielding 60 microbial isolates that were identified by culture and profiled for antibiotic resistance. Isolates were then tested for their ability to express virulence in response to [Pi] limitation using C. elegans nematodes as a screening tool. C. elegans, which feed on microbes as their main food source, were transferred onto high cell density microbial lawns growing on high (25 mM) and low (0.1 mM) phosphate media and tracked for known behavioral responses associated with microbial virulence expression such as colony avoidance, reduced progeny formation, and mortality. We also performed electron microscopy of recovered strains to identify if phosphate sensing protein PstS was expressed on bacterial membranes as a function of phosphate scavenging under phosphate-limited conditions. Finally to assess if microbes are exposed to low [Pi] when present in the human intestine during critical illness, human stool filtrates were assayed by ELISA for bacterial proteins involved in phosphate sensing (i.e PstS).
Results: Pathogens typically associated with gut-derived sepsis were isolated from stool of critically ill patients including C. albicans, K. pneumoniae, P. aeruginosa, and S. marcescens. There was predominance (∼70%) of multi-drug resistance (MDR) among isolates. Phosphate dependent mortality against C. elegans was observed for all pathogens isolated, with C. albicans and MDR P. aeruginosa displaying the greatest killing effect (p < 0.01, data not shown). Nematodes fed on phosphate-depleted lawns of MDR K. pneumoniae and S. marcescens expressed colony avoidance behavior and reduced progeny formation with both phenotypes disappearing when bacterial strains were grown under [Pi] sufficient conditions (p < 0.001, data not shown). PstS was identified to be present on outer membrane surface in certain bacterial strains recovered from stool of ICU patients demonstrating the overactivation of phosphate-scavenging system. Finally proteins found to be secreted by isolated strains of P. aeruginosa under low Pi conditions (PstS PA5369, PstS PA0688, PA0681) were detected to be several fold increased in the stool filtrates of critically ill patients providing compelling evidence that intestinal pathogens are exposed to low [Pi] in vivo.
Conclusion: These data provide the first clinical evidence that, despite aggressive daily protocols to prevent and treat hypophosphatemia with supplemental phosphate, the intestinal tract of critically ill patients can be depleted of phosphate- a condition that has the potential to shift a wide variety of its colonizing flora to express enhanced virulence and a potentially lethal phenotype. Strategies to maintain local intestinal phosphate sufficiency during critical illness may have important therapeutic non-antibiotic implications for infection/sepsis prevention.
BantonKaysie LMDMcCullochKaren ABSWasilukKaren RPhD
University of Minnesota
TIR DOMAIN VARIANTS OF MAL/TIRAP RESULT IN ALTERED TLR4 SIGNALING
Background: Mal/TIRAP is an integral protein of several Toll-like receptor (TLR) pathways, the activation of which results in NF-kB upregulation and leads to cytokine production. Mal, TLR4, and MyD88 all share a conserved C-terminus containing 3 distinct regions, or boxes, of amino acid (aa) sequence similarity which is collectively referred to as the Toll-Interleukin 1 Receptor (TIR) domain. Mal is unique in that it does not share aa sequence similarity of box 3 within the TIR domain with other TIR proteins. Mal acts as a bridging adaptor between TLR4 and MyD88 amplifying the signaling response pathway. We hypothesize that the TIR domain of Mal specifies the binding and activation proclivities of Mal when activated through TLR4 by LPS stimulation.
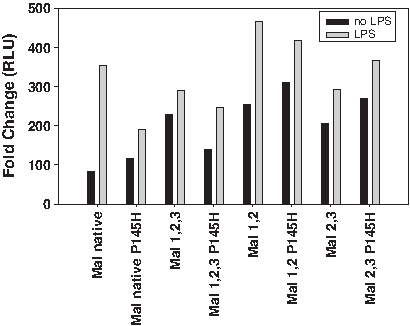
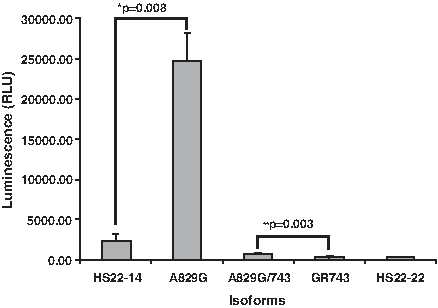
Methods: Mal and truncated Mal TIR constructs containing various combinations of the 3 boxes and a potential dominant negative mutation (P145H) within the TIR domain were cloned into the expression vector pcDNATM4HisMax and cotransfected into RAW 264.7 cells with an NF-kB luciferase reporter vector and a control vector. Transfected RAW 264.7 cells were then stimulated with lipopolysaccharide (LPS). NF-kB upregulation was measured by luciferase assay. The P145H mutation mimics the box 2 TIR domain mutation found in the dominant negative form of TLR4 identified in C3H-HeJ mice, known to be resistant to the effects of lipopolysaccharide.
Results: Mal P145H was found to significantly abrogate the upregulation of NF-kB in RAW 264.7 cells in response to LPS stimulation, whereas Mal 1,2,3 had increased activity over that of the full length native protein but does not significantly increase the stimulation with LPS. The dominant negative form (Mal 1,2,3 P145H), while having baseline diminished activity compared to Mal 1,2,3 was able to be stimulated by LPS. Mal 1,2 and Mal 2,3 have activity far exceeding that of the full length protein with and without the P145H mutation in box 2 and show increased upregulation of NF-kB in the presence of LPS.
Conclusion: These structure function studies of Mal suggest that although the individual contribution of the N-terminal portion of the protein may be important for MyD88/TLR4 coupling based on computer models, the C-terminal TIR domain is critical for downstream NF-kB and cytokine activation independent of the polymorphic P/H mutation. Identification of the role of each conserved box within the TIR will lead to further understanding of the molecular mechanisms regulating the proinflammatory response.
DarwicheSophie SMDRuanXiangcaiMDScottMelanieMD, PhDHoffmanRosemaryPhDPapeHans-ChristophMDBilliarTimothy RMD
University of Pittsburgh
LATE POST-TRAUMATIC IMMUNE DYSFUNCTION: THE ROLE OF TLR2 AND TLR4 SIGNALING
Introduction: Imbalance in the post-traumatic inflammatory response often leads to severe complications in multiple trauma patients including increased suspectibility to sepsis post-injury. Toll-like receptors (TLRs) have been implicated in inflammatory responses after trauma. However, the role of TLR4 and TLR2 in delayed immune dysfunction following trauma such as severe skeletal injury is unknown. To study this we have developed a novel pseudofracture model which recapitulates the systemic and end-organ responses observed following bilateral femur fracture and we investigated the contribution of TLR2 and TLR4 on the delayed immune dysfunction following severe trauma.
Methods: Male wild type (WT) C57BL/6, TLR2-/- and TLR4-/- mice (n = 4-10), underwent pseudofracture (crushed bone solution injection and soft tissue injury to the thigh musculature bilaterally). Control mice received no experimental manipulation. At 48 hrs, spleens were harvested to assess splenocyte proliferation and Th1cytokine release (IFNγ, IL-2) in response to concanavalin A (2.5 μg/ml). Splenocyte proliferation was assessed using tritiated thymidine uptake as counts per minute (c.p.m.). Statistical significance (p < 0.05) was assessed by Student's t-test and ANOVA.
Results: WT mice showed a significant decrease in splenocyte proliferation at 48 hrs after pseudofracture (21,258 ± 1,723 c.p.m.) in comparison to controls (48,102 ± 4,808 c.p.m.). Splenocyte proliferation in TLR2-/- mice was similar to WT mice at baseline (46,486 ± 3,371 c.p.m.). However, in contrast to WT mice, splenocytes from TLR2-/- mice proliferated at the same rate as uninjured mice even after injury (40,249 ± 1,900 c.p.m.). We found significantly impaired splenocyte proliferation in all TLR4-/- mice, both uninjured controls (22,161 ± 3,906 c.p.m) and at 48hrs after pseudofracture (27,386 ± 2,650 c.p.m).
Splenocyte release of Th1 cytokines was also significantly decreased in injured WT mice (IL-2: 94.9 ± 8.5 pg/mL; IFNγ: 158.0 ± 31.8 pg/ml) in comparison with controls as expected (IL-2: 250.3 ± 18.5 pg/mL; IFNγ: 622.0 ± 50.8 pg/ml). This significant suppression was also found in the splenocytes from the injured TLR2-/- mice (IL-2: 159.6 ± 5.9 pg/mL; IFNγ: 199.7 ± 31.9 pg/ml) compared with TLR2-/- control mice (IL-2: 309.4 ± 10.0 pg/mL: IFNγ: 477.1 ± 82.3 pg/ml). However, all the TLR4-/- mice showed reduced IL-2 release, in a similar pattern that mirrored the proliferation findings (uninjured: 91.0 ± 8.0 pg/mL; injured: 126.8 ± 6.9 pg/mL). A reduced IFNγ release was noted in splenocytes from control TLR4-/- mice (174.6 ± 38.9 pg/mL), and this was not seen in injured TLR4-/- mice where IFNγ release was similarly raised to baseline WT levels (531.3 ± 40.9 pg/mL).
Conclusion: Our novel pseudofracture model leads to delayed immune dysfunction typical of severe injury models. Our observation that TLR2 and TLR4 deficient animals fail to develop specific aspects of the delayed immune dysfunction indicates that signaling through these TLRs contributes to the immunosuppression seen after severe trauma and represent potential as therapeutic targets to limit injury-induced immune suppression and susceptibility to sepsis post-injury.
WangJinMS,GrishinAnatoly VPhDFordHenri RMD, MHA
Childrens Hospital Los Angeles
MKP-1 PROMOTES TOLERANCE TO TLR LIGANDS IN ENTEROCYTES
Introduction: Tolerance to intestinal microbiota is one of the key aspects of gut homeostasis. In fact, intestinal disorders such as necrotizing enterocolitis and inflammatory bowel diseases may result from the failure to establish or maintain tolerance to luminal bacteria. Thus, understanding the pathogenesis of these diseases critically depends on our ability to define the mechanisms that govern mucosal tolerance. In this study, we sought to elucidate the role of MKP-1, the mitogen-activated kinase (MAPK) phosphatase that negatively regulates inflammatory signaling via MAPK, in tolerance to toll-like receptor (TLR) ligands in enterocytes.
Methods: Enterocyte cell lines were treated with various TLR ligands for 0-4 h. Expression of MKP-1, phosphorylation of p38, and degradation of inhibitory subunits (IkB) of nuclear factor kappaB (NF-kB) were examined by Western blotting. MKP-1 was localized intracellularly using immunofluorescence microscopy. Binding of NF-kB and activation of MKP-1 promoter were examined using chromatin immunoprecipitation and transcriptional reporter.
Results: Ligands of TLR3 (dsRNA), TLR4 (lipopolysaccharide, LPS), TLR5 (flagellin, Fla), and TLR9 (CpG DNA), but not TLR2 (peptydoglycan, Pgn), transiently induce MKP1, coincident with dephosphorylation of p38 following peak TLR ligand-induced phosphorylation, and preceded by transisent degradation of IkB (Figure). Inhibitors of NF-kB, but not MAPK, block LPS-induced expression of MKP-1, whereas siRNA knockdown of IkBα prolongs expression of MKP-1. Rat MKP-1 promoter contains two NF-kB-binding sites. Mutational inactivation of these sites abrogates LPS-induced transcription from the MKP-1 promoter. In the small intestine, MKP-1 is expressed in the crypts, the epithelial compartment that also displays bacteria-dependent activating phosphorylation of p38.
Conclusion: TLR ligand induced, NF-kB-mediated expression MKP-1 may promote rapid establishment of tolerance to TLR ligands in enterocytes via deactivation of p38.
LapchakPeter HMSc, PhD,RaniPoonamMSc,KannanLakshmiPhDLuccaJurandir J DalleMDTsokosGeorge CMD
Beth Israel Deaconess Medical Center and Harvard Medical School
PLATELET CD154 MEDIATES REMOTE TISSUE INJURY FOLLOWING MESENTERIC ISCHEMIA AND REPERFUSION
Introduction: Platelets express a number of immunologically important proteins including CD40, and when activated, CD154 (CD40L), CD62P (P-selectin) and its ligand, (PSGL-1) which together link platelets to innate immunity. While previous studies have demonstrated a role for CD62P in ischemia/reperfusion (I/R) injury, no studies have determined a central role for platelets and platelet CD154 or CD40. We hypothesize that expression of CD154 on activated platelet mediate local mesenteric and remote lung tissue damage after ischemia and reperfusion.
Methods: Wild type (WT; C57BL/6J), CD40 knock out (KO) mice, CD154KO mice, CD154KO mice passively transferred with normal gamma globulin and platelet-depleted WT mice transfused with CD154KO platelets underwent mesenteric ischemia for 30 minutes and reperfusion for 3 hours. Local intestinal and remote lung injury was evaluated by histology.
Results: Wild type mice that underwent mesenteric I/R injury had tissue damage characterized by loss of villi integrity and hemorrhage. Remote lung injury was characterized by increased vascular congestion consisting of erythrocytes, platelets, neutrophils and monocytes. In contrast, CD40KO and CD154KO mice that underwent I/R demonstrated significantly less villi damage and no remote injury to the lung when compared to WT mice. The CD154KO mouse is the equivalent to human hypergammaglobulinemia which is characterized by the presence of normal to high serum IgM and the absence of other Ig isotypes. CD154KO mice passively transferred with normal IgG underwent I/R. Replacement of IgG in these mice did not induce local nor remote tissue damage. We next determined whether platelet-depleted WT mice transfused with CD154KO platelets presented with local and remote tissue damage following I/R. Mesenteric tissue damage in WT mice transfused with CD154KO platelets was similar when compared to WT mice. In contrast, no remote lung tissue injury was apparent when compared to WT mice by histological examination.
Conclusions: These findings indicate that CD154 expression on platelets does not mediate local (intestinal) injury. In contrast,, platelet CD154 expression is a critical mediator in remote (lung) tissue injury. Replacement of IgG in CD154KO mice did not mediate either local or remote tissue injury suggesting that CD154 on immune cells other than platelets participate in this injury process. Together, these findings suggest that multiple mechanisms are involved in local and remote tissue injury and also identify platelets or platelet CD154 as a potential therapeutic target to limit remote tissue injury.
ElhassanIhab OMDHannoushEdward JMDAlzateWalter DBSc, MSc,SifriZiad CMDLivingstonDavid HMDMohrAlicia MMD
New Jersey Medical School
BETA BLOCADE PREVENTS HEMATOPOIETIC PROGENITOR CELL SUPPRESSION FOLLOWING HEMORRHAGIC SHOCK
Introduction: Previous work has shown that severe injury accompanied by sympathetic stimulation induces bone marrow (BM) dysfunction by both suppression of hematopoietic progenitor cell (HPC) growth within the BM and HPC mobilization to the peripheral circulation. The resultant anemia and immune system suppression can last for up to two weeks following injury. Our previous work has demonstrated that beta blockade given prior to lung injury reduced both HPC mobilization and restored HPC growth within the BM. This study aims to examine the effect of beta blockade prior to or at the time of hemorrhagic shock (HS).
Methods: Male Sprague-Dawley rats (wt 250 - 300 g) were assigned to four groups (N = 4-8 per group). Three groups underwent hemorrhagic shock (HS) via blood withdrawal maintaining the MAP between 30 - 40 mmHg for 45 minutes after which shed blood was reinfused and the animal was sacrificed at 3 hours. Two of the three groups received beta-blocker as follows: one group received a single daily IP propranolol dose (8-10mg/kg) for three days prior to HS (3dBB/HS), the other group received a single dose of IP propranolol (10 mg/kg) following HS during resuscitation (HS/BB). HPC growth was assessed via GEMM, BFU-E, and CFU-E colony growth in the BM at 3 hours. Blood pressure and heart rate were recorded (*p < 0.05 by ANOVA and Tukey-Kramer analysis).
Results: Administration of beta blockers prior to injury or during resuscitation restored HPC growth similar to that of control levels (*p < 0.05). This trend was similar for both GEMM and CFU-E colony growth. 3dBB/HS and HS/BB had a decrease in heart rate as compared to HS at the end of shock (360 bpm and 340 bpm vs. 490 bpm).
Conclusion: Administration of non-specific beta blockade at the time of resuscitation significantly reduces BM suppression following HS. The BM protection is identical to that observed when beta blockers are administered prior to injury. Therefore, beta blockade may play an important role in attenuating the BM dysfunction seen following shock.
CastleShannon LMDWangJinMS,WilliamsMonicaBSGrishinAnatoly VPhDUppermanJeffrey SMDFordHenri RMD, MHA
Childrens Hospital Los Angeles, Keck School of Medicine, University of Southern California
P-GLYCOPROTEIN IS REQUIRED FOR BREAST MILK-INDUCED PROTECTION FROM NECROTIZING ENTEROCOLITIS IN A NEONATAL MOUSE MODEL
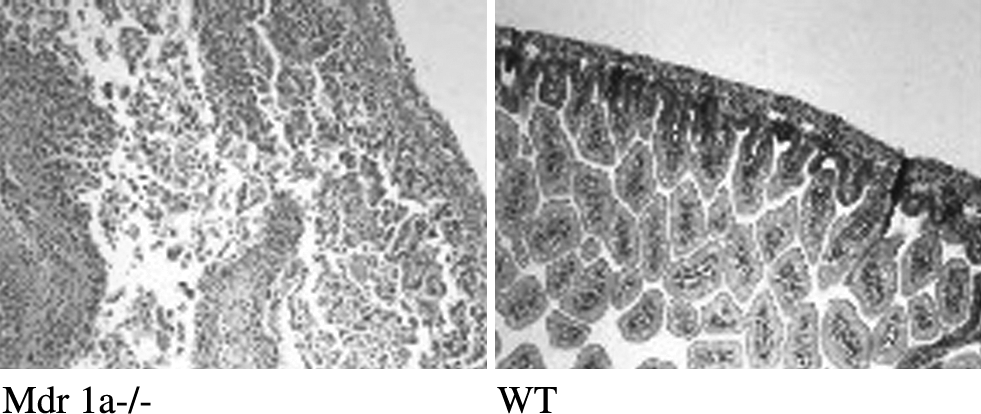
Background: Necrotizing enterocolitis (NEC) is an inflammatory intestinal disorder affecting premature infants. NEC presumably involves colonization of the gut with opportunistic pathogens. One such pathogen, Enterobacter sakazakii (ES) has been associated with hospital outbreaks of NEC. It is also known that breast feeding protects from NEC. P-Glycoprotein (Pgp), a product of the multidrug resistance gene, Mdr1a, a transmembrane transporter found on intestinal epithelial cells, may protect against the effects of bacterial invasion by facilitating the efflux of xenobiotics and toxins. We have previously shown that breast milk induces Pgp in the neonatal intestinal epithelium and that Pgp-deficient mice have increased susceptibility to NEC. In this study, we tested the hypothesis that breast feeding protects from NEC via induction of Pgp.
Methods: WT and congenic Mdr1a−/− newborn mice were administered 107 cfu ES or equivalent amount of PBS and allowed to nurse with their mothers. Mortality was determined as frequency of death or events requiring euthanasia (abdominal distension, profuse bleeding or diarrhea, cyanosis, lethargy). Pathology of NEC was graded by examination of H&E-stained ileal samples by a pathologist blinded to the groups. Mortality, timing of disease, and pathology grades were compared using the Mann-Whitney test.
Results: There was no evidence of illness in the 2 groups not exposed to ES, and the average pathology grade was 0.19+/−0.25 in the WT and 0.75+/−0.75 in the Mdr1a-/- group. In the WT-ES group, 4 of 9 died on day of life (DOL) 3(1 pup), 4(2 pups) and 5 (1 pup) respectively, and the remainder were healthy by DOL 5. In the Mdr1a−//−-ES group, all 8 died, with death occurring at DOL 2(2), 3(4), 4(1) and 5(1). Mean pathology scores in the two latter groups were 0.5+/−1.3and 2.5+/−1.4, respectively.
Conclusion: Mdr1a-/- mice had higher mortality, more rapid onset of the disease and higher NEC pathology grades than WT mice when challenged with ES. We conclude that P-glycoprotein is required for breast milk-induced protection from NEC.
A CONCISE INSTRUMENT FOR SEPSIS SCREENING IN GENERAL SURGERY PATIENTS
Purpose: Validate a screening tool for the early identification of sepsis in a general surgical ward.
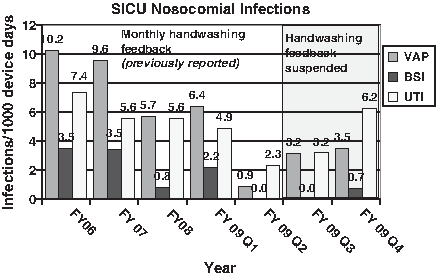
Background: Sepsis is the leading cause of mortality in non-coronary intensive care units (ICU). Recent studies have shown that early implementation of evidence based guidelines improves survival. We have developed a comprehensive logic-based sepsis protocol for our surgical ICU (SICU); however, we found that early recognition of sepsis was a major obstacle to protocol implementation. To improve this, we developed a three-step sepsis screening tool with escalating levels of decision making. We previously validated that this tool was effective in identifying sepsis in the SICU; however, >50% of the septic patients (pts) were transferred from the surgical ward. Therefore, in order for our sepsis screening tool to be maximally effective it needed to be implemented & validated in the non-SICU setting. We hypothesized that our sepsis screening tool would identify sepsis on the surgical ward.
Methods: All pts admitted to the general surgical ward were screened twice daily by nursing staff. The initial screen assesses the systemic inflammatory response syndrome (SIRS) parameters (heart rate, temperature, white blood cell count, & respiratory rate) & assigns a numeric score (0 to 4) for each based on severity of derangement. Pts with summed SIRS scores ≥4 screened positive & proceeded to the 2nd step of the tool in which a mid level provider attempts to identify an infectious source. If the patient screens positive for both SIRS & an infection, the attending surgeon was notified & sepsis specific interventions were implemented. Pts demographic & outcome data including source of sepsis, SICU transfer status, & mortality were prospectively collected. After verifying satisfaction of logistic regression analysis assumptions & testing for interactions, logistic regression analyses quantified the predictive properties of the overall SIRS score, & hierarchically assessed predictive properties of each of its 4 subcomponent scores.
Results: Over 6 months ending 10/06/09, 9,332 screens were completed on 959 pts. The average age of the screened population was 56.8 ± 17.6 years & 61.5% were female. The prevalence of sepsis was 1.7%. The screening tool yielded a sensitivity of 99.9%, specificity of 91.3%, a positive predictive value of 16.3%, & a negative predictive value of 99.9%. The sepsis related mortality in those pts that screened positive for sepsis was 6.3%. Of the 16 pts that developed sepsis, 4(25%) required transfer to the SICU. Of the 16 true-positive screens, 14 (87.5%) had sepsis, & 2 (12.5%) had severe sepsis at the time of the screen. The sources of infection were intrabdominal (62.5%), bloodstream (6.25%), urinary system (6.25%), skin/soft-tissue (6.25%) & 3 cases did not have a definitive source identified.
Conclusion: The three-step sepsis screening tool is a valid method for the early identification of sepsis on a surgical ward. The vast majority of pts detected by the screening tool were in sepsis & had not progressed to severe sepsis/septic shock. The high sensitivity & negative predictive value of the screening tool make it a useful & safe screening tool for sepsis in the surgical population. Future studies evaluating the use of this screening tool in conjunction with early goal directed therapy for sepsis & the impact of this on SICU transfer rates & patient outcomes are planned
ShankerBeth-AnnMDChoiChunMDCoyleSusette MRN, MSN,MacorMarie ARN,NosherJohn LMDCalvanoSteve EPhDLowryStephen FMD
UMDNJ-Robert Wood Johnson Medical School
ROUTE OF FEEDING DIFFERENTIALLY INFLUENCES MONOCYTE GENE EXPRESSION
Introduction: Specialized nutrition support is a common technology applied to surgical and critically ill patients. Currently, there is little understanding of how varying the route of feeding (parenteral versus enteral) and nutritional formulations influence gene expression. We hypothesized that there would exist distinctly different gene expression profiles in monocytes obtained from subjects on enteral versus parenteral routes of feedings. Knowing the effects of nutritional formulation and routes of feeding on gene expression could improve our understanding of the relationship between nutritional substrates, gene expression, and immune and metabolic responses in critically ill patients.
Methods: Nine healthy subjects, aged 18-40, were admitted for 4 days/3 nights. Subjects were randomized into parenteral (TPN, n = 6) or enteral (TF, n = 3) feeding groups, and all received continuous feedings for 72 hours. All subjects had blood collected for monocyte purification and gene expression analysis by Affymetrix FOCUS chip (8,793 gene probes). Acceptance criteria for differentially expressed genes required ≥1.5 median fold change (FC) and/or p < 0.05. Significant data were annotated to pathways using Ingenuity Pathway Analysis. An innate filter was also applied to the significant gene data set.
Results: Monocytes gene expression after 72 hours of feeding.
The above differentially expressed genes were also categorized into immune function pathways. Among the differentially expressed genes in the TPN subjects were up-regulated Signal Transducers and Activators of Transcription (STAT) 1 and 3; up-regulated Toll-Like Receptor 4 (TRL4); up-regulated TNF receptor-associated factor 5 (TRAF5); up-regulated gp130 and IL-6 receptor; and down regulated IL-18.
Conclusion: Differing nutritional modalities influence monocyte gene expression. Parenteral feeding appears to have a more profound effect than enteral feeding on monocyte gene expression after 72 hours. By the stringent criteria adopted for this study, the genes and pathways most affected are those involved in immune function and signaling.
All genes
Immune Filter
TF p < 0.05
143 67 up; 76 down
4: 2 up, 2 down
TF p < 0.05 + FC ≥ 1.5
11: 4 up; 7 down
1 up
TPN p < 0.05
1524: 1003 up; 521 down
38: 22 up, 16 down
TPN p < 0.05 + FC ≥ 1.5
187: 75 up; 111 down
8: 2 up, 6 down
KraftRobertMDHerndonDavid NMD, FACS,SongJuquanMDKulpGabriela AMS,JeschkeMarc GMD, PhD
University of Texas Medical Branch, Galveston
PREDICTIVE VALUE OF IL-8 FOR SEPSIS AND SEVERE INFECTIONS AFTER BURN INJURY: A CLINICAL INVESTIGATION
Introduction: Monitoring the inflammatory response after thermal injury is one of the major challenges in burn care. Burn injury leads to an increased inflammatory response. Markers such as CRP and IL-6 are not sensitive to predict sepsis and major infections post burn. IL-8 is one of the major mediators of the inflammatory response. IL-8 is also considered as a mediator of the inflammatory response and in metabolic processes. The aim of our study was to investigate the role of IL-8 as a diagnostic marker for infections post burn.
Methods: Four hundred sixty eight pediatric patients were enrolled in this study. Plasma cytokines, acute phase proteins, constitutive proteins, and hormones were analyzed during the first 60 days post admission. Demographics and outcome variables (length of stay, sepsis, multi organ failure, and mortality) were recorded. A cut off level for IL-8 was determined using receiver operating characteristic (ROC) analysis. Statistical analysis was evaluated by Student's t-test corrected with Bonferroni`s post-hoc test and Chi Square test. Statistical significance is set at (p < 0.05).
Results: ROC analysis identified a cut off level of 234 pg/mL for IL-8 and survival (A = 0.88). Patients were grouped according this cut off in high (h) and a low (l) groups. Analysis of cytokines, and acute phase response showed significant higher levels in the h group (IL-6, CRP) (p < 0.05). In the l group regression analysis revealed a significant predictive value of IL-8 to TBSA burn size and incidence of MOF (p < 0.001) but not to incidence of sepsis (p = 0.41). In the h group a significant link between IL-8 and sepsis (p = 0.002) was identified whereas burn size and MOF were not significant related.
Conclusion: IL-8 expression is associated with burn size and infections. Levels up to 234 pg/mL are significantly related to TBSA burn size and multi organ failure. Levels greater than 234 pg/ml are correlate strongly with the incidence of sepsis and mortality. These data suggest that plasma levels of IL-8 may be a valid parameter monitoring sepsis in burn victims.
FancherTiffany TMDPieracciFrederic MMD, MPH,EachempatiSoumiMDRashidiLailaMS,NashGarrett MMD, MPH
St. Marys Hospital, Denver
INTERVAL APPENDECTOMY AFTER NON-OPERATIVE MANAGEMENT OF ACUTE APPENDICITIS AT A CANCER CENTER
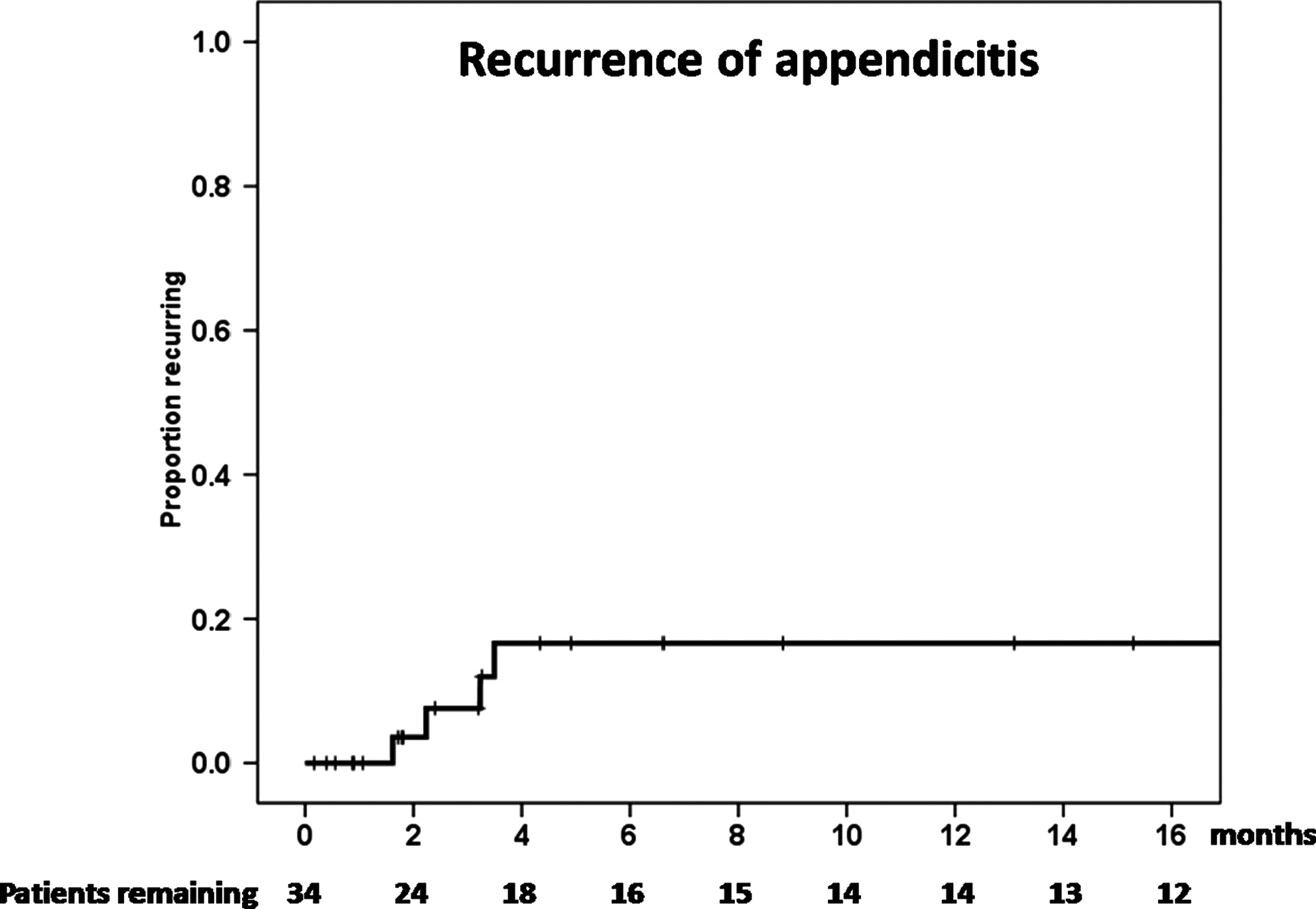
Background: The role of interval appendectomy in adults after non-operative management of acute appendicitis (AA) is unclear. We hypothesize that recurrent appendicitis is uncommon in patients managed without appendectomy (NA) during their index hospitalization for AA.
Methods: Clinical presentation, cancer treatment, and follow-up were collected from the electronic medical records of patients with CT scan confirmed AA from July 1999 through July 2009 at a tertiary cancer center. Medians of continuous data were compared using the Wilcoxon rank sum test.
Results: Seventy-five of 109 AA patients (68.8%) underwent appendectomy during the index hospitalization (IHA). Three IHA patients had more than 48 hours of medical management of AA prior to appendectomy. Thirty-four of 109 AA patients (31.2%) were NA. The median index hospitalization length of stay of the NA patients 6 days (0-55) and the median age was 59 (18-80). The reasons for NA were presence of an abscess or phlegmon (N = 14), mild symptoms (13), high surgical risk (3), end-stage cancer (3), and patient declining surgery (1). Among NA patients, 8 had percutaneous drainage of an abdominal abscess, the median duration of IV antibiotics was 5 days (0-55) and the median total duration of IV + PO antibiotics was 12 days (0-55). 35% of NA patients and 35% of IHA patients had received chemotherapy in the prior 30 days. During the index hospitalization for AA there were 6 deaths (3 IHA, 3 NA), 4 patients died of sepsis and 2 of cancer progression. At a median follow up of 19 months (range 1-103), 4 of the 31 NA patients who survived initial hospitalization had recurrent AA (12.9%) at 2, 2, 3 and 3 months after the first episode of AA [Figure]. Each had radiologic or symptomatic resolution of AA between episodes. Five NA patients had planned interval appendectomy (16.1%) at 1-7 months post AA and 22 remained asymptomatic without interval appendectomy (70.9%). Three of 22 subsequently asymptomatic patients suffered cancer-related death less than 1 year after AA.
Conclusion: Among patients at a cancer center managed non-operatively at the time of the initial episode of AA, recurrent AA was early (<4 months) but uncommon. Interval appendectomy should be used judiciously in this patient population.
DuttonWilliam DMDAbouassalyChadi TMDCottonBryan AMD, MPHMayAddison KMDGunterOliver LMD
Vanderbilt University Medical Center
MASSIVE TRANSFUSION DOES NOT CAUSE INFECTIONS IN THE CRITICALLY ILL
Background: Transfusion of blood and blood products has been associated with immunologic modulation and increased risk of infection. While the total volume of blood transfusions has been shown to increase risk, the need for large volume transfusions in hemorrhaging patients has not been examined as a risk factor. We evaluate a non-trauma surgical critical care population to identify independent risk factors for infection and hypothesize that massive transfusion (≥10 U RBC in 24 hours) is not independently associated with hospital-acquired infections.
Methods: A retrospective study of adult critical care patients entered into a prospectively collected surgical critical care database between 01/2005 and 06/2008 was performed to identify risk factors for nosocomial infection. Massive transfusion (MT) was defined as ≥10 units RBC transfused in a 24-hour period following admission to the ICU. Prospective surveillance using standard NHSN definitions for hospital-acquired infections (HAI) was performed. Univariate analysis identified factors associated with development of HAI. Using HAI as the primary endpoints, multiple logistic regression analysis was performed to identify the independently associated covariates.
Results: 3,791 patients were admitted during the study period and comprised the study group. 2,667 (70%) received no transfusion, and 1,056 (28%) received <10U RBC during their entire ICU admission. 68 (1.8%) received MT. MT patients were predominantly male, were more likely to develop HAI, and had a longer ICU length of stay (LOS), higher APACHE II scores, and ICU mortality (p < 0.001). After adjusting the study group for age, gender, BMI, mechanical ventilation, total blood volume, and APACHE II, MT was not significantly associated with HAI, specifically; blood stream infection (BSI), pneumonia (PNA), or surgical site infection (SSI), however was independently associated with urinary tract infections (UTI).
Conclusion: Massive transfusion is not solely responsible for hospital-acquired infections such as BSI, PNA, or SSI. The risk of development of HAI should not be a deterrent to indicated transfusion, especially in hemorrhaging patients that may require massive transfusion. Further investigation is necessary to determine the relationship of transfusion-related immunosuppression with HAI.
HAI, hospital-acquired infections; OR , odds ratio; CI, confidence interval; BSI, blood stream infection; PNA, pneumonia; SSI, surgical site infection; UTI, urinary tract infection; *adjusted OR to age, gender, ICU LOS, BMI, mechanical ventilation, total blood volume, and Acute Physiology and Chronic Health Evaluation II. ROC AUC ≥ 0.79 in all models.
TowfighShirinMDClarkeTatyanMDGuptaAnkurMDCitronDiane MMS
Cedars-Sinai Medical Center
CHRONOLOGICAL STUDY OF BACTERIAL FLORA IN CONTAMINATED WOUNDS
Introduction: Contaminated surgical wounds may be treated with primary closure and systemic antibiotics, with an expected infection rate of 20% (range 7–50%). The change in bacteriology and the counts within these wounds have never been studied as a function of time.
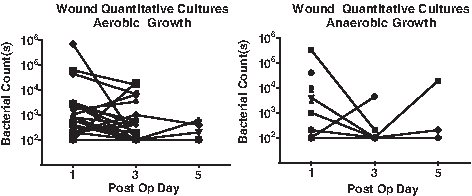
Methods: Patients with perforated appendicitis underwent open appendectomy and qualitative intra-abdominal cultures. All patients were given antibiotics and randomized to primary wound closure vs wound closure plus daily wound probing using a sterile cotton tip applicator. Quantitative cultures of the wound were performed on post-operative days (PODs) 1, 3, and 5, or until the wound had sealed and was impenetrable.
Results: From 2007–2009, 77 patients were randomized. Patients in the wound-probing arm (N = 38) had significantly less wound infection compared to the non-wound-probing arm (2.6% vs 18.9%, p = 0.028). Quantitative wound cultures on POD 1 showed aerobic growth in 30/38 (78.9%, range bacterial counts: < 102, 7x105). The most common aerobic bacteria were Coag (-) Staph. (60.5%), Alpha-Strep. (26.3%), and gram (-) lactose fermenting rods (13.2%). In comparison, the abdominal cultures of aerobes were E. coli (44.7%), Strep. (36.8%) and P. aeruginosa (21.1%). Anaerobic growth was found in 13/38 (34.2%, range bacterial counts: < 102, 3.2x105). The most common anaerobic bacteria were gram (+) bacilli (36.8%) and gram (+) cocci (7.9%). In comparison, the abdominal cultures of anaerobes were Bacteroides (68.4%) and Prevotella (10.5%) species. Most wounds were impenetrable within 3 to 4 days (See Figures). All bacterial counts prior to wound healing were less than 104 for aerobes and less than 103 for anaerobes. We found no correlation between bacterial counts or flora and patient demographics, diabetes, body mass index, and abdominal girth.
Conclusion: The microbiology of contaminated wounds are mixed flora of aerobic bacteria, with one-third also having anaerobic bacteria. This is independent of diabetes and body habitus. There is poor correlation between abdominal cultures and wound cultures, with a predominance of Staph. and other gram (+) bacteria found in the wound even on POD 1.
The bacterial counts decrease sharply, with less than 104 aerobes and 103 anaerobes by POD 3.
While direct comparison of wound bacterial counts cannot be made between the probed and the non-probed wounds, the six-fold reduction in wound infections in the probed wounds cannot be ignored. We surmise that wound probing appears to reduce the rich substrate necessary for bacterial proliferation and may be the reason for the drops in bacterial counts. This minimally invasive procedure certainly warrants additional study as an effective tool in dramatically reducing wound infections in contaminated settings.
HoVanessa PMDNicolauDavid PPharmD,DakinGregory FMDPompAlfonsMDRichBarrie SMDToweChristopher WMDBariePhilip SMD, MBA
Weill Cornell Medical Colege
CEFAZOLIN DOSING FOR SURGICAL PROPHYLAXIS IN MORBIDLY OBESE PATIENTS
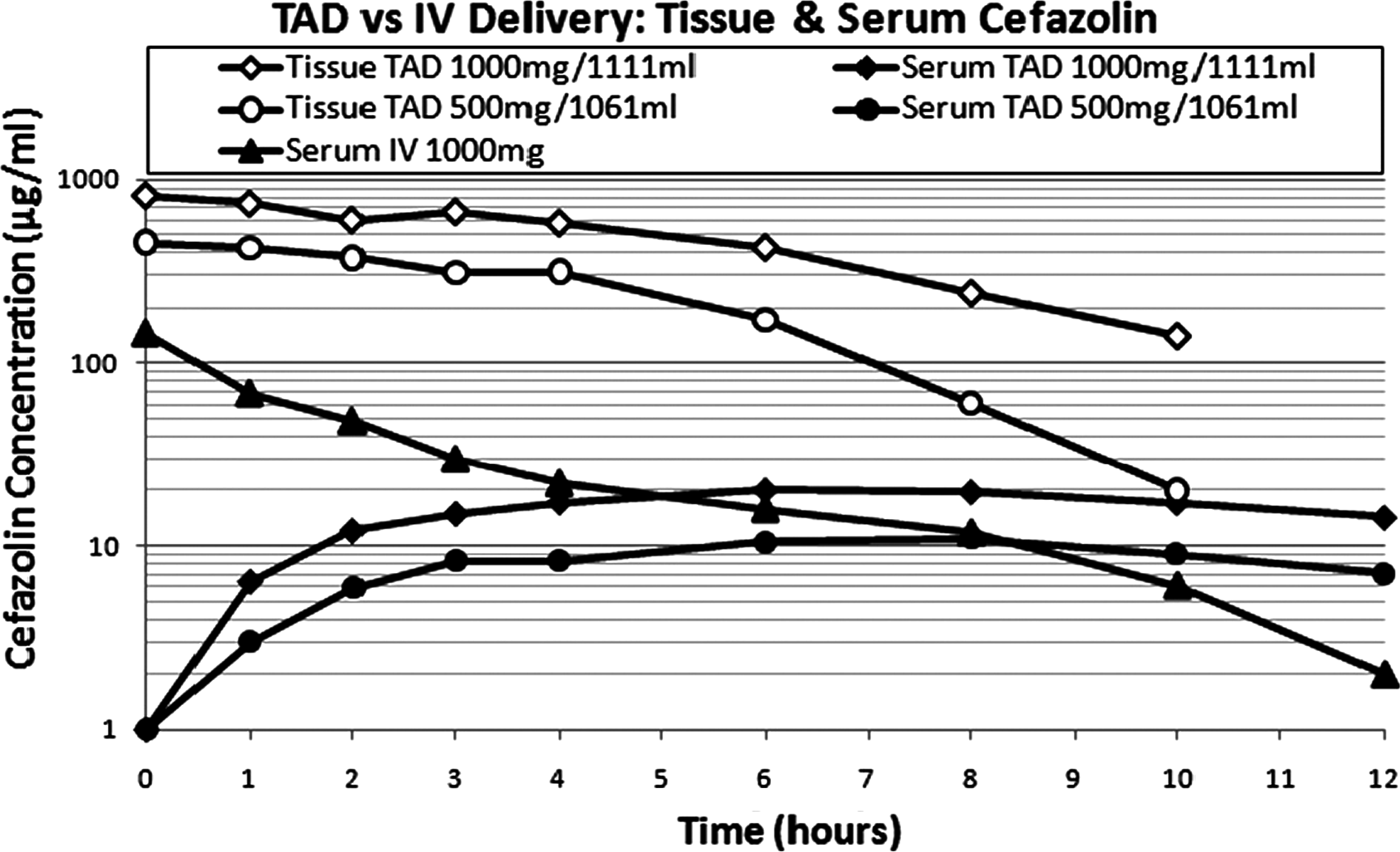
Background: Cefazolin (CZL) is used commonly to prevent surgical site infection (SSI) after procedures on morbid obesity (MO) patients, but specific dosing guidelines are lacking. We hypothesized that CZL 2 g given either IV push (IVP) or over 30 min (INF) would suffice for SSI prophylaxis in MO, and CZL 3 g (C3G) would be sufficient in super-morbid obesity (SMO).
Methods: Fifteen MO patients (BMI 40-50 kg/m2) undergoing elective surgical procedures were studied. Ten received CZL 2 g via IVP, and five received CZL 2 g via INF. Five SMO patients (BMI > 50 kg/m2) received C3G over 30 min. Serum CZL concentrations were assayed at t = 0, 30, 120, and 360 min using a validated high performance liquid chromatography method. The elimination rate constant was calculated using a linear regression of the terminal portion of the concentration versus time in minutes, and time above the minimum inhibitory concentration (TMIC) was calculated using a protein binding value of 85%
Results: Mean CZL concentrations (mcg/ml) after t = 30 were similar in all groups (Figure). Administration method did not affect the elimination rate constant (IVP − 0.024, 95% CI [−0.042 - − 0.006], INF −0.033 [−0.042 - −0.024], C3G − 0.028 [−0.054- − 0.003]). For pathogens with MIC < 8, TMIC was 3.75 hours for IVP, 3.42 hours for INF, and 4.87 hours for C3G.
Conclusions: Cefazolin is appropriate prophylaxis for MO patients against low-resistance pathogens. For hospitals with SSI pathogens with MIC < 8 mcg/mL, CZL 2 g can be administered by IVP or INF with redosing every 3-4 h. A 3 g dose of CZL may not be necessary for patients with SMO.
KushnirLeonMDChambersKarinnMDGallichioMichael HMDContiDavid JMD
Albany Medical Center
URETERAL STENT PLACEMENT IS A SIGNIFICANT RISK FACTOR FOR THE DEVELOPMENT OF BK VIREMIA AFTER RENAL TRANSPLANTATION
Introduction: Polyoma (BK) nephropathy develops in 5–10% of renal transplant recipients and is a serious complication associated with a high rate of graft dysfunction and loss. The initiation of immunosuppressive agents after transplantation to prevent rejection likely leads to reactivation and proliferation of donor- or host-derived latent BK virus, which resides in the genitourinary tract. Interestingly, nephropathy due to BK virus only develops in kidney allografts and has not been reported in host native kidneys of similarly immunocompromised heart, liver or lung transplant recipients. Thus, it is hypothesized that both local tissue inflammation as well as immunosuppression are requisites for reactivation and proliferation of BK virus. Our aim was to measure whether surgical nephroureteral stent placement at the time of transplantation to facilitate the ureteroneocystostomy was associated with an increased risk for BK viremia.
Methods: In 1/06 we initiated a serum screening policy for all newly transplanted patients by obtaining monthly blood testing for BK determination by PCR. Between 1/1/06 and 12/31/08, 175 renal transplants were performed at our institution. Ureteral stents were placed in 95 (54%) recipients (group A) while stents were not used in 80 (46%) patients (group B). The decision to utilize a ureteral stent was based on local operative findings and surgeon preference. Recipients in both groups were treated with the same immunosuppressive protocol consisting of thymoglobulin induction, followed by maintenance therapy with prograf, mycophenolate mofetil and prednisone or rapamune. Demographics between the two groups were similar with respect to age, gender, ethnicity, diabetes and incidence of acute rejection.
Results: Serum PCR became positive for BK virus in 30/175 patients after transplantation (17%). Mean time to a positive PCR post-transplant was 5 months (2-11 mos.). PCR results segregated by ureteral stenting identified that BK viremia was detected in 23/95 (24%) group A patients compared to only 7/80 (9%) group B patients (P < 0.05).
Conclusion: Intraoperative placement of ureteral stents during renal transplantation is associated with a significantly increased risk of BK viremia. In light of this finding serious consideration should be given to minimize the utilization of ureteral stents or, in cases where stent placement is required due to operative conditions, early removal and aggressive screening for BK viremia.
LanJinggangPhDHeneghanAaron FPhDSanoYoshifumiMDJonkerMarkMDOmataJiroMDFuYang-XinMD, PhDXuWentongMDPierreJoeBA,KudskKenneth AllanMD
University of Wisconsin, Madison
PARENTERAL NUTRITION (PN) IMPAIRS LYMPHOTOXIN RECEPTOR (LTβR) SIGNALING VIA NF-κB
Introduction: Lymphotoxin (LT) normally stimulates LTβR in Peyer's patches (PP) to activate NF-κB via the non-canonical pathway to produce adhesion molecules (MAdCAM-1), cytokines, and chemokines critical to mucosal immune cell entry & function. Without LTβR, mice lack PP & lymph nodes and have less expression of MAdCAM-1, CCL-20, CCL25, CXCL13 and lower IL-4, IL-10 & IgA. PN decreases LTβR, MAdCAM-1 & these chemokines in PP and also lowers gut IgA compared to chow. The normal LT/ LTβR interaction activates the non-canonical NF-κB pathway to process the p100/RelB precursor and yield p52/RelB. Through an inflammatory canonical path, TNFα, IL-1β, & bacterial products (via TLR) stimulate NF-κB producing p65/p50 and c-Rel/p50 heterodimers. Inflammation increases gut IgA levels. This work determines effects of PN, exogenous LTβR stimulation & exogenous LTβR blockade on both NF-κB activation pathways.
Methods: Expt 1: Phosphorylated canonical (p50& p65) and non-canonical (p52 & Rel B) NF-κB proteins in PP were analyzed by TransAM NF-κB Family kit after 5 days of chow (n = 19) or PN (n = 16). Expt 2: For 2 days, mice received chow (n = 13), PN + 5 μg of an LTβR-stimulating antibody BID, i.v(PN-LTβR,n = 17)) or PN + control antibody (PN-control n = 18) with Phosphorylated NF-κB proteins in PP analyzed as Expt 1. Expt 3: For 3 days mice received Chow + control Ig (Chow n = 9), Chow + blocking LTβR-Ig fusion protein (100 μg i.v.) (Chow- anti LTβR. N = 10), or PN + control Ig (PN, n = 8) to analyze Phosphorylated NF-κB in PP as Expt 1.
Results: PN significantly reduced all NF-κB proteins in PP compared with chow (p < 0.01 for all except Rel B (p < 0.05)) . LTβR stimulation with PN increased p50 (p < 0.01), p52 (p < 0.01), and Rel B (p < 0.01) in PP vs PN alone with no differences vs chow in p65, p52 and Rel B; only p50 (p < 0.01) remained depressed in PN-LTβR vs chow. LTβR blockade of chow mice reduced non-canonical pathway (p52; p < 0.01) and Rel B; p < 0.01) to PN levels but not the inflammatory path (p50 and p65).
Conclusion: Lack of enteral stimulation during PN decreases canonical and non-canonical NF-κB pathways in PP. LTβR stimulation during PN completely restores PP non-canonical NF-κB activity & partly restores the canonical pathway. LTβR blockade decreases non-canonical PP NF-κB activity but not canonical.
p < 0.05 vs chow; ap < 0.01 vs chow; bp < 0.01 vs PN .
DiebelLawrence NMDLiberatiDavid MMS
Wayne State University
VARIABLE IGA PROTEASE ACTIVITY BY BACTERIAL PATHOGENS: EFFECT ON PMN INFLAMMATORY POTENTIAL
Introduction: Secretory IgA (sIgA) is one of the principal antibodies in respiratory and other mucosal secretions. IgA antibody structure is critical for biological properties including the “noninflammatory properties” of antigen binding and interaction with other host defenses including polymorphonuclear (PMN) cells and other myeloid cells. In this regard, sIgA may protect the host from “collateral” damage due to exaggerated inflammatory responses to invasion by luminal pathogens. Loss of intact sIgA due to microbial cleavage may contribute to invasion and an exaggerated inflammatory response by the host. Pseudomonas aeruginosa (Ps) infection causes significant morbidity and mortality; a number of virulence factors are expressed by Ps which contribute to it's pathogenicity. However sIgA cleavage by different Ps strains is not well established. The relative ability of different strains of Ps and other gram negative or gram positive bacteria to cleave sIgA and to modulate PMN inflammatory potential (IP) was studied in vitro.
Methods: Polyclonal sIgA was co-cultured with a non-virulent strain of Ps (clinical strain, CS), a virulent strain of Ps (ExoT,U), Klebsiella pneumonia (Kp), Acinetobacter (Ac) or Staphylococcus aureus (Sa). Cleavage of sIgA was detected by measurement of intact sIgA and the cleaved secretory component (SC) by size exclusion and ELISA. In additional experiments PMNs were challenged with supernatants (sup) obtained from the above coculture and superoxide anion (O2-), elastase release and CD11b expression
Results: Mean ± SD (N = 3 for each group). See table above.
p < 0.001vs.control, $p < 0.001vs.matched group (no IgA).
Conclusion: Intact sIgA decreased PMN inflammatory responses to all bacterial species. Cleavage of sIgA was noted with all gram negative bacteria; however cleavage was significantly greater with the virulent Ps strain. “Cleaved” sIgA was ineffective in modulating PMN responses to the virulent Ps strain. Loss of effective sIgA antibody function may be critical in the establishment of pneumonia and poorer outcome due to pneumonia from virulent Ps strains or other bacteria with significant IgA cleavage potential.
YamakawaKazumaMDMohriTomoyoshiMDKiguchiTakeyukiMDKitayamaJunichiMDMatsudaHirokiMDNakamoriYasushiMDFujimiSatoshiMD
Osaka General Medical Center
TREATMENT EFFECTS OF RECOMBINANT HUMAN SOLUBLE THROMBOMODULIN IN PATIENTS WITH SEVERE SEPSIS: PRELIMINARY HISTORICAL CONTROL STUDY
Introduction: Thrombomodulin (TM) is a transmembrane protein on the endothelial cell, which forms a 1:1 complex with thrombin. The complex enhances the cascade from protein C to activated protein C (APC), which inactivates factors VIIIa and Va under the presence of protein S, thereby inhibiting further thrombin formation. On the other hand, the N-terminal lectin-like domain (D1) of recombinant human soluble TM (rhTM) decreases the levels of high-mobility group box-1 protein (HMGB1) and lipopolysaccharide in the plasma in experimental endotoxemia. However, it is not known how rhTM is working in the patients with disseminated intravascular coagulation (DIC) following severe sepsis.
Design: Single-center, historical control study.
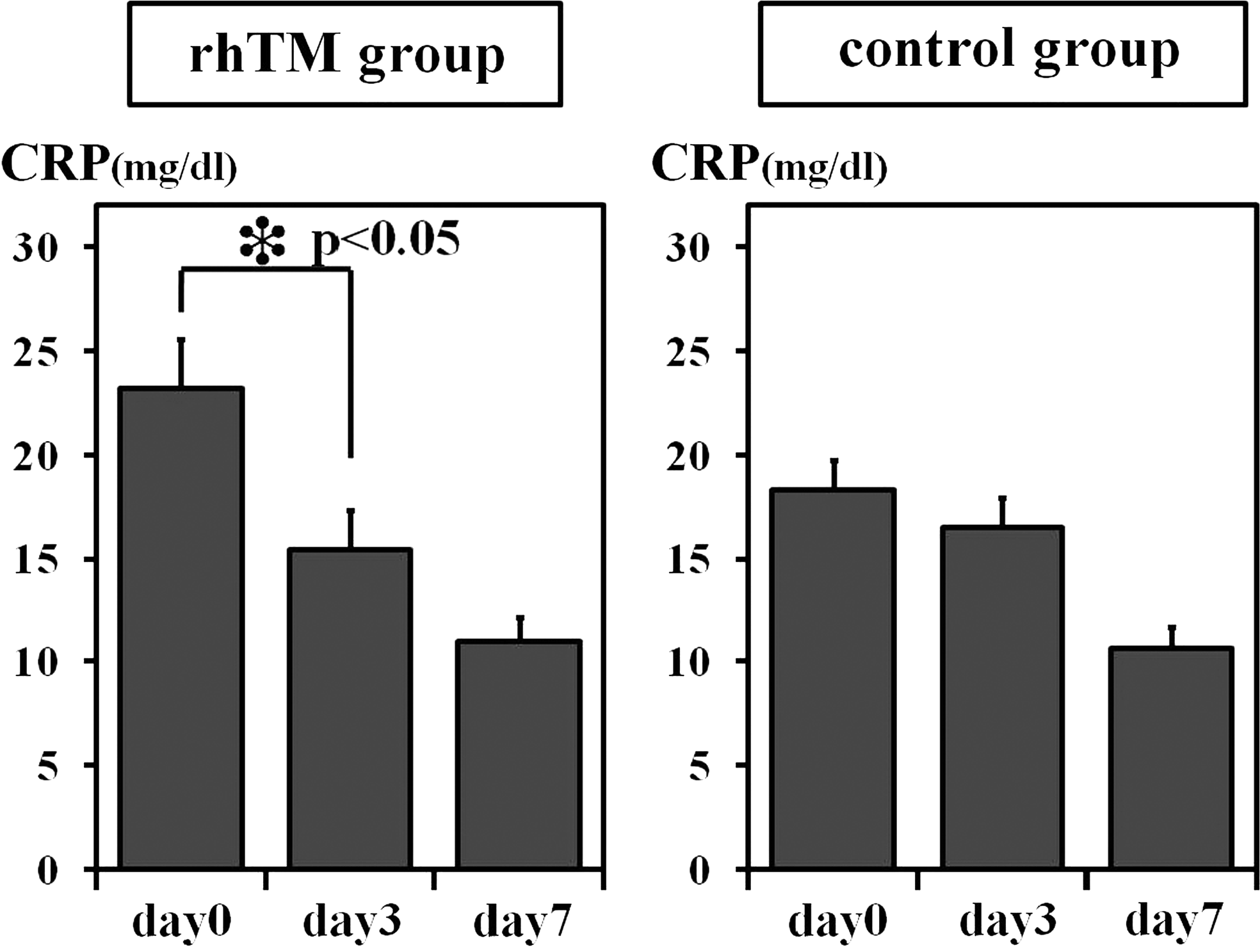
Materials and Methods: 65 consecutive patients with severe sepsis and septic shock with DIC that needed ventilator management were included in this study from Jan. 2006 to May 2009. DIC was diagnosed by using the Japanese Association for Acute Medicine DIC criteria. All patients were treated according to the strategy of Surviving Sepsis Campaign Guideline. Initial 45 patients were not treated with rhTM (control group). Last 20 patients were given rhTM (380U/kg/day) for 6 days after fulfilling the entry criteria showing above (rhTM group). Patients were followed for 28 days after the entry. We measured the platelet number and the levels of CRP and FDP on sequential days. We compared increasing rate of platelet and the reduction rate of CRP and FDP as a base for day 0.
Results: The characteristic was the same in two groups. There was higher survival rate in rhTM group compared to control group (75% vs. 53%, p = 0.09 by the log-rank test). There was no difference of the increasing rate of platelet number in two groups. The levels of FDP and CRP in the rhTM group were dramatically decreased in day 3 compared to day0, while there was not the same tendency in control group.
Conclusions: We found that rhTM administration reduced the levels of CRP in the patients with DIC following severe sepsis. Although the treatment of rhTM did not statistically improve the survival rate, it might have a crucial role to modulate inflammatory responses in severe sepsis as well as to control the coagulant cascade in DIC.
KhadarooRachel GMD, PhD, FRCSC,FortisSpyridonMDStreutkerCathyMD, MSc,ZhangHaiboMD, PhD
University of Alberta
ILEAL FATTY ACID BINDING PROTEIN (I-FABP) A NOVEL BIOMARKER FOR ACUTE INTESTINAL ISCHEMIA AND RESULTANT LUNG INJURY
Background: Acute intestinal ischemia/reperfusion (AII/R) broadly affects critically ill patients in the areas of trauma, transplantation, cardiac surgery, shock, and sepsis. The mortality rates from intestinal ischemia range from 60-80% and has not changed in past 70 years. The high mortality rates from intestinal ischemia are due to the severity of the disease and development of remote organ injury. AII/R results in a remarkable systemic inflammatory response, and lung injury is frequently implicated. However, the mechanisms by which AII/R results in lung injury are not clearly understood. The high mortality rates of intestinal ischemia are also related to the failure to make the diagnosis.
Objective: To search for biomarkers of AII/R that would aid in earlier diagnosis, treatment, and prevention of further systemic injury in critically ill patients.
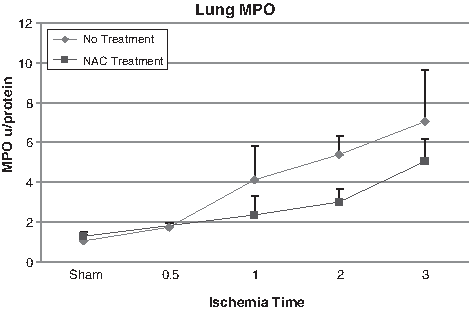
Methods: C57BL/6 mice were subjected to intestinal ischemia by occlusion of the superior mesenteric artery (SMA). A time course of intestinal ischemia from 0.5 to 3h was performed and followed by reperfusion for 2h. In separate experiments, N-acetylcysteine (NAC) was given prior to reperfusion. Intestinal injury was assessed by myeloperoxidase (MPO) levels and serum measurements of neutrophil, lactate, and I-FABP. Lung injury was measured by wet/dry ratio, neutrophil and protein influx in the bronchoalveolar lavage (BAL), and MPO levels. A pathologist, blinded to the study, performed the histopathologic grading of the intestinal and lung tissue.
Results: Neutrophil sequestration (MPO) in the intestine increased from <0.01 U/g to a peak of 0.074 U/g at 2h of intestinal ischemia. Intestinal pathology revealed normal mucosal villi at 0.5h. Pathologic signs of ischemia were then evident at 1h and by 3h of ischemia demonstrated areas of full thickness coagulative necrosis. Importantly, I-FABP was able to identify intestinal ischemia by 0.5h even prior to pathological changes. I-FABP levels directly correlated with ischemia time with levels of 5, 71, 238, and 2295 ng/mL at 0, 0.5, 2, 3h of intestinal ischemia respectively. Intestinal ischemia resulted in evidence of lung injury in a time dependent manor. The neutrophil sequestration in the lung, measured in lung homogenate, directly correlated with intestinal ischemia time. Lung MPO was <2 U/g at 0.5h of intestinal ischemia which increased to >6 U/g by 3h of ischemia (Figure 1). This was confirmed by pathologic examination. Pretreatment with NAC showed a decrease in MPO levels demonstrating oxidants are involved in the process of intestinal I/R induced-lung injury. Serum measurements of I-FABP also directly correlated with lung injury (R2 = 0.88, p = 0.037).
Conclusion: I-FABP predicted AII/R prior to pathological evidence of ischemia and also directly correlated with resultant lung injury. Pretreatment of AII/R with the antioxidant NAC prevented lung injury, suggesting a role for oxidants in this mechanism. I-FABP is a promising biomarker for AII/R and may guide the treatment with antioxidant in early intestinal and distal organ injury.
FranklinAshanti LBA,GunerYigitMDWilliamsMonicaBSUppermanJeffrey SMDGrishinAnatolyPhDFordHenri RMD
Childrens Hospital Los Angeles
HUMAN MILK INDUCES DOSE AND TIME- DEPENDENT P-GLYCOPROTEIN EXPRESSION IN HUMAN ENTEROCYTE CELL LINES
Background: Necrotizing enterocolitis (NEC) is a devastating gastrointestinal emergency that affects premature neonates. Despite recent advances in neonatal medicine, the morbidity and mortality from NEC have not changed appreciably over the last three decades. Risk factors for NEC include very low birth weight (<1,500 g), formula feeding, hypoxia, and bacterial colonization of the gut. Breast milk is highly protective against NEC. P-glycoprotein (Pgp) is an efflux ATP-binding cassette transmembrane transporter that protects against intestinal inflammation by pumping out a broad range of toxins and xenobiotics from enterocytes. Pgp is encoded by the multidrug resistant gene (MDR1). Pgp is found in the liver, brain, kidney, and intestine. Previous studies from our lab have shown that breast-fed, but not formula-fed neonatal rats have increased expression of Pgp in the small intestine, and that rat breast milk induces Pgp expression in rat enterocyte cell lines in vitro.
Purpose: The purpose of this study is to determine the kinetics of (human) breast milk-induced expression of Pgp in Caco-2 and HT-29 enterocytes.
Methods: The human-derived cell lines, Caco-2 and HT-29, were treated with various concentrations (0-20%) of the water-soluble fraction of human breast milk for 0-24 h. Pgp induction was determined by Western blotting with the anti-Pgp antibody, C219. Chinese hamster ovary cell line, CHCR5, which constitutively expresses Pgp, was used as a positive control. To determine which component of breast milk induces Pgp, low molecular weight components (Mr < 10 kD) of human breast milk were separated by gel filtration using Sephadex G-50 column.
Results: Human breast milk induced Pgp in Caco-2 and HT-29 cells in a dose-dependent manner at concentrations ranging from 0.5-20%. Expression of Pgp increased between 2-6 h of treatment and remained elevated for 24 h. Pgp was induced in Caco-2 cells by the high molecular weight fraction of breast milk.
Conclusion: The high molecular weight water-soluble fraction of breast milk induces Pgp in Caco-2 and HT-29 cells in a dose- and time-dependent manner. Induction of Pgp by human breast milk may contribute to the intestinal protection against NEC.
Dose-response Induction of Pgp in Caco-2 Cells.
ChoiChun WMDShankerBeth-AnnMD, MS,CoyleSusette MRN,MacorMarie ARN,CalvanoSteve EPhDLowryStephen FMD
UMDNJ-Robert Wood Johnson Medical School
IMMUNE-RELATED BIOMARKERS AND THE DEVELOPMENT OF NOSOCOMIAL INFECTION IN ICU PATIENTS
Introduction: Critically-ill surgical patients are susceptible to secondary insults, such as nocosomial infections. Current risk stratification of critically-ill patients is largely based on clinical indicators. Efficacy of biomarkers in risk-profiling of these patients has not gained routine clinical applicability. Therefore, we hypothesized that real-time risk analysis can be enhanced by utilizing dynamic markers of inflammation and immune cell activation. This study evaluated the utility of immune-related biomarkers and inflammatory mediators among patients susceptible to nocosomial infection at early time points after surgical ICU admission.
Methods: Forty-four patients considered at risk for subsequent infection were prospectively evaluated from the time of ICU admission until the documentation of an infection. All patients underwent daily clinical surveillance and laboratory analysis to determine activation of polymorphonuclear (PMN) cells (CD11b, CD64) and monocytes (HLA-DR) by flow cytometry. IL-6, TNF levels were assessed by ELISA. Data (mean ± SEM) shown below represent the levels of cell markers in the first 48 hours of ICU admission in those who remained without an infection (-infection) or developed a nocosomial infection (+infection) during the ICU stay.
Results: APACHE II scores at the time of ICU admission were equivalent for the two groups. TNF levels were not significantly different (data not shown). Markers of immune cell activation (CD64, CD11b, IL-6) were higher in patients who developed infections during the ICU course. HLA-DR, a marker of antigen presentation, was inversely related to the development of infection.
Conclusion: The present data suggest critically-ill surgical patients prone to the development of infection exhibit enhanced PMN activation and inflammatory cytokine response as well as decreased monocyte immune surveillance early in the ICU course. This analysis illustrates the clinical utility of real-time biomarker surveys to promote closer scrutiny and possibly earlier intervention in patients at risk for developing nocosomial infections.
Data represent mean ± SEM; RFI: Relative fluorescence intensity.
EnkhbaatarPerenleiMD, PhDZhuYongMD, PhDRehbergSebastianMDYamamotoYusukeMD, PhDSousseLindaBSTraberLillian DRN,HerndonDavidMDTraberDaniel LPhD
University of Texas Medical Branch
PEROXYNITRITE MEDIATES VASCULAR LEAKAGE VIA PROMOTING ANGIOPOEITIN-2 IN METHICILLIN-RESISTANT STAPHYLOCOCCUS AUREUS-INDUCED SEPSIS
Introduction: The incidence of both hospital and community acquired methicillin-resistant Staphylococcus aureus (MRSA) infections is progressively increasing. Previously, we have reported that MRSA-induced sepsis caused more severe vascular leakage and significantly higher plasma levels of nitrite/nitrate compared to Pseudomonas aeruginosa sepsis. The aim of present study was to investigate mechanical aspects underlying MRSA sepsis-related vascular hyperpermeability. We hypothesized that peroxynitrite is primarily responsible for the severe vascular permeability in MRSA sepsis via promoting the angiogenic growth factor angiopoietin-2 (ang-2). We have tested the hypothesis, using our well-established ovine sepsis model and in vitro endothelial cell culture technique.
Method: I. Ovine model. Sheep were instrumented with Swan Ganz, femoral artery, and left atrium catheters to monitor hemodynamics for 24 h. Sepsis was induced by instillation of live MRSA (2.5X10^11CFU) into lungs by bronchoscope under anesthesia. After the injury, sheep were awakened, placed on ventilator, and fluid resuscitated. Urine output was measured via Foley catheter. Groups: 1) control: MRSA instillation, no treatment, n = 5; 2) treated: MRSA instillation + peroxynitrite decomposition catalyst (PDS), n = 5. Continuous i.v. infusion of PDS was started 6 h post-injury with dose of 0.02 mg/kg/h following bolus dose of 0.1 mg/kg.
II. In vitro study. Human umbilical vein endothelial cells (HUVEC) were challenged for 4 h with 105 CFU of live MRSA and pretreated with or without 5 μM PDC and cell permeability (the amount FITC-Dextran that passed through the confluent HUVEC monolayer) and ang-2 mRNA (RT-PCR) were determined. Cells infected with MRSA were also co-incubated with or without ang-2 (5 μg/mL) and its receptor Tie-2 (5 μg/mL) antibodies and cell permeability was determined (n = 4).
Results: Injured animals showed severe hypotension (MAP) and excess fluid retention. Control animals also showed severe hemoconcentration associated with decreased plasma protein and plasma oncotic pressure. However, these pathological changes were attenuated by PDS treatment. MAP (mmHg) was 94 ± 3 at baseline and 66 ± 3 at 24 h in control vs. 93 ± 1 at baseline and 82 ± 10 at 24 h in treated groups. Fluid retention (mL/kg) was 102 ± 32 and 30 ± 8 in control and treated groups at 24 h, respectively. PDC (34 ± 1), and ang-2 (30 ± 1) and Tie-2 receptor (32 ± 1) antibodies reduced HUVEC cell permeability induced by MRSA (73 ± 4) 4 h post co-incubation. PDC reduced ang-2 release from MRSA infected HUVEC cells as well.
Conclusion: It has been shown that interaction of ang-2 and its receptor Tie-2 induces endothelial permeability. Our data strongly indicate that peroxynitrite decomposition catalyst reduces/prevents microvascular hyperpermeability by modulating the ang-2/Tie-2 interaction. Inhibition of reactive nitrogen species should be considered for the future therapy for septic patients.
ZhangLemengPanPinhuaEvankovichJohnCardinalJonBilliarTimothyMDTsungAllanMD
University of Pittsburgh
THE INTERFERON REGULATORY FACTOR-1 REGULATES THE BALANCE BETWEEN APOPTOSIS AND AUTOPHAGY IN ENDOTOXEMIA
Objectives: The pathophysiology of sepsis is complex, and unfortunately poorly understood. Sepsis-induced apoptosis is known to contribute to end-organ injury and ultimately death. Recent evidence suggests that autophagy is also activated in sepsis and is believed to primarily play a protective role in the progression of the disease. In addition, apoptosis and autophagy share a number of common signaling pathways and mediators, and therefore may be linked to one another. However, how the balance between these two cellular processes affects sepsis induced outcomes has not been described. In this study, we show that the transcription factor interferon regulatory factor-1 (IRF-1) is pivotal in regulating the balance between apoptosis and autophagy in a model of endotoxemia.
Methods: Male IRF1-KO and wildtype C57BL/6 mice were injected with a lethal dose of intraperitoneal LPS (35mg/kg). Control mice received injections of sterilized PBS. 96h survival rates were assessed. Splenic,lung and liver tissues were analyzed by Western blot, flow cytometry, immunofluorescent staining, TUNEL staining and transmission electron microscopy. In vitro, murine RAW 264.7 cells were transfected with pEGFP-LC3 and analyzed by immunofluorescent microscopy, western-blot and RT-PCR.
Results: In vivo, IRF-1 knockout mice were significantly protected from endotoxin-induced mortality (p < 0.01). This protection was associated with less end-organ apoptosis as seen with fewer TUNEL postivie cells and decreased cleaved Caspase-3 activation in splenic, lung and liver tissues in IRF-1 knockout mice compared to their wildtype countertypes. Interestingly, IRF-1 knockout mice exhibited evidence of increased autophagic flux with an increase of the active form of LC3, LC3-II, in the same tissues. In vitro, LPS stimulation increase autophagy in both harvested splenocytes and peritoneal macrophages in IRF-1 knockout compared to wildtype cells as measured by LC3 activation and autophagic vesicle formation. Conversely, in response to LPS stimulation, IRF-1 knockout macrophages experienced decreased apoptosis as seen by lower caspase-3 cleavage levels and chromatin condensation. To determine the signaling pathway for LPS induced IRF-1 activation leading to autophagy, we examined the role of the Janus associated kinase (JAK) pathway. IRF-1 activation was induced in a JAK-dependent manner as RAW264.7 stimulated with LPS in the presence of a JAK inhibitor demonstrated decreased induction of IRF-1. JAK inhibition during LPS stimulation in RAW264.7 cells also recapitulated the effects seen in IRF-1 knockout cells with diminished apoptosis and increased autophagy. Furthermore, the mechanism of IRF-1 regulation of autophagy may involve mammalian target of rapamycin (mTOR), a negative regulator of autophagy since JAK inhibition significantly decreased mTOR activation.
Conclusion: Our study defines a novel role for the transcription factor IRF-1 in regulating the balance between apoptosis and autophagy in the setting of endotoxemia. IRF-1 appears to shift this balance in the direction of apoptosis, while IRF-1 knockdown and/or inhibition results in the opposite effect (i.e. promoting autophagy while inhibiting apoptosis). Understanding the regulation of IRF-1 activity may lead to potential targets to improve sepsis related outcomes.
DavisJohn MMDKuoYen-HongScM, MSKuoYen-LiangMDAhmedNasimMD
Jersey Shore University Medical Center
REPORT CARD ON SURGICAL CARE IMPROVEMENT PROJECT (SCIP): NIS INFECTION DATA 2001 THROUGH 2006
Background: In the late 1990's the quality of health care was questioned in two landmark publications, To Err is Human and Crossing the Quality Chasm. Concern about the errors in delivering health care became such a bellwether issue that the Centers for Medicare & Medicaid Services instituted the Surgical Care Improvement Project (SCIP) in 2001 to standardize core measures to improve patient care. The requirement to deliver appropriate antibiotics in a timely fashion and to discontinue postoperatively was one of the first of the SCIP initiatives.
Methods: To determine what impact this program has had on the rates of postoperative surgical infections (POSI) the National Inpatient Sample database was used to evaluate infections in adult patients (age ≥18 years old) for elective cholecystectomies (open: n = 19,706; laparoscopic: n = 72,920) and elective colectomies (n = 90,596) from the years 2001 through 2006. Annual infection rates were determined for each of the operations. Mortality rates and length of stay (LOS) were also assessed.
Results: Postoperative infections increased in colon surgery steadily from 2.60% in 2001, to 2.68% in 2002, to 2.87% in 2003, to 2.99% in 2004, to 3.23% in 2005, and to 4.27% in 2006. This rise in infection was statistically significantly (p < 0.0001). An increase in POSI from 2001 to 2006 was seen in open cholecystectomies surgery from 1.13% in 2001 to 1.94% in 2006 (p = 0.01) and in laparoscopic cholecystectomies from 0.28% in 2001 to 0.55 % in 2006 (p = 0.001). LOS was significantly increased in infected compared to noninfected patients for all three groups (p < 0.0001).
Conclusion: The growing infection rates documented in this study may be due to many reasons rather than noncompliance with the SCIP protocol. These include: 1) a rise in the reporting of infections, 2) a true increase in the infection rate, 3) a weakness of the database, or 4) a problem with SCIP.
RoseAlexanderMDZhaoJingPharm, D,WahbyKristaPharm, D,DotsonBryanPharm, D,TennenbergStevenMD
Wayne State University School of Medicine, Dept. of Surgery
RECONSIDERATION FOR CULTURING VASCULAR CATHETERS FOR SUSPECTED CR-BSI IN THE ICU
Introduction: Catheter-related bloodstream infection (CR-BSI) due to central venous lines is estimated to occur in 80,000 intensive care unit (ICU) patients each year in the USA. While traditional epidemiological criteria require matching catheter and blood cultures, more recent criteria only require bacteremia with the absence of an identified non-catheter source. Most recent clinical practice guidelines now recommend treating Staphylococcus aureus catheter colonization in the absence of bacteremia. Clinically however, bacteremia with any known pathogen will necessitate antimicrobial therapy, regardless of catheter culture results. We therefore sought to determine the clinical utility of vascular catheter cultures in critically ill patients.
Methods: We retrospectively reviewed all positive (>15 colony forming units [cfu] by semiquantitative roll-plate technique) vascular catheter tip cultures (CTCs) from Sept 1, 2006 through mid-November 2009 in the 40-bed, mixed medical-surgical ICU tower of a large university hospital. CR-BSI was defined by a matching positive blood culture obtained shortly before or up to 1 day after the time of catheter removal.
Results: A total of 474 CTCs were obtained. 234 (49%) were negative. 108 (23%) had <15 cfu/roll.
In 47 of 48 (98%) cases of CR-BSI, the positive blood culture occurred + /- 1 day from the catheter's removal and dictated antibiotic therapy. In only 1 of 48 (2%) cases of CR-BSI did the catheter's removal and culture significantly (>1 day) precede the positive blood culture. 23% of positive CTCs had polymicrobial growth at >15 cfu/roll. In comparison, hospital epidemiology surveillance reported 39 cases of confirmed CR-BSI in this patient cohort.
Only 5 cases (4% of all positive CTCs, 1% of all CTCs) of S. aureus catheter colonization (>15 cfu/roll) in the absence of bacteremia were identified. 4 of these 5 patients had been started on vancomycin prior to the index colonized catheter being removed.
The microbiology laboratory costs for the 474 CTCs, organism identification and sensitivity testing were approximately $20,000 and required 205 microbiology technician hours.
Conclusion: In an ICU patient population, only about 1/4 of vascular catheters removed and cultured are positive for significant bacterial colonization. Only about 1/3 of positive CTCs are associated with CR-BSI. 98% of all CR-BSIs can be identified by bacteremia which dictates antimicrobial therapy either prior to or coinciding with catheter removal. Therefore, since CTCs rarely change therapy, our data suggest that routine vascular catheter cultures in suspected CR-BSI in the ICU setting may not be required.
THE NORMALIZATION OF HYPERCORTISOLEMIA POST-BURN WITH KETOCONAZOLE DOES NOT ATTENUATE THE HYPERMETABOLIC CATABOLIC RESPONSE
Background: Hypercortisolemia has been suggested as a primary hormonal mediator of whole body catabolism following severe burn injury. Ketoconazole, an anti-fungal agent inhibits cortisol synthesis. We therefore sought to study the effect of Ketoconazole on post-burn cortisol levels and hyper-catabolic response.
Methods: Forty-nine severely burned pediatric patients with burns >30% total body surface area (TBSA) were enrolled into the study and were block randomized 2:1 to receive standard care (controls, n = 32) or standard care plus ketoconazole (n = 17). Patients were similar in age, and TBSA. Demographics, clinical data, serum hormones, serum cytokine expression profile, organ function, hypermetabolism, muscle protein synthesis, incidence of wound infection sepsis, and body composition were obtained throughout acute hospital course. Statistical analysis was performed using Student's t-test or ANOVA where applicable.
Results: There were no significant differences in demographics between treatment groups. Ketoconazole effectively blocked cortisol production indicated by normalization of the 8-fold elevation of urine cortisol levels (p < 0.05). However, there were no significant differences in the inflammatory response, acute phase proteins, body composition, muscle protein breakdown or synthesis, or organ function between groups. Both groups were markedly hypermetabolic and catabolic throughout acute hospital stay.
Conclusion: Normalization of hypercortisolemia with ketoconazole therapy had no effect on whole body catabolism, or the post-burn inflammatory or hypermetabolic response. The data suggests that hypercortisolemia does not play a central role in the post-burn hypermetabolic, catabolic response.
NamiasNicholasMDHilleDarcy AMS
University of Miami
EFFECT OF BODY MASS INDEX (BMI) ON CLINICAL RESPONSE TO TREATMENT FOR COMPLICATED INTRAABDOMINAL INFECTION (CIAI)
Objective: To determine the effect of BMI on clinical response to the treatment of cIAI.
Methods: This is a post hoc analysis of microbiologically evaluable patients at early follow up assessment (EFA), using the data from a prospective randomized trial of ertapenem vs. piperacillin tazobactam for the treatment of cIAI. Patients were grouped into either normal (<30 kg/m2) or high (≥30 kg/m2 ) BMI to determine the effect of BMI on the proportion of favorable clinical response. . The proportions in the normal and high BMI categories were compared with a 95% exact confidence interval on the difference within each treatment group.
Results: The microbiologically evaluable population at EFA included 231 patients, 123 patients for the ertapenem and 108 patients for the piperacillin/tazobactam treatment groups. The proportion of patients with a favorable clinical response assessment at EFA by BMI and treatment group is shown in the table below. 12 patients did not have BMI recorded and were excluded. Patients receiving piperacillin tazobactam had a nominally lower response rate in the high BMI group.
Proportion of Patients With Favorable Clinical Response Assessments—at EFA (Microbiologically Evaluable Population)
n = favorable clinical response, N = number in subgroup, exact test on difference of two proportions.
Conclusion: Differing antibiotic regimens may yield different clinical response rates for cIAI in patients with a high BMI. Due to the limitations of post hoc analysis and small subgroups, further study is needed.
CuschieriJosephMDSakrSanaPhDWilsonCaseyBSHennesseyLauraRN,ArbabiSamanMD, MPHOKeefeGrantMD, MPHMaierRonald VMD
Univesity of Washington
PLASMA LEVELS OF CHOLESTEROL PREDICT THE DEVELOPMENT OF NOSOCOMIAL INFECTIONS IN TRAUMA PATIENTS
WITHDRAWN
HeffernanDaithi SMD, AFRCSI,MonaghanSean FMDThakkarRajan KMDMachanJason TPhDAyalaAlfredPhDCioffiWilliam GMD, FACS
Department of Surgery, Rhode Island, Brown University
FAILURE TO NORMALIZE LYMPHOCYTE REDUCTION FOLLOWING TRAUMA IS ASSOCIATED WITH INCREASED MORTALITY, INDEPENDENT OF THE LEUKOCYTOSIS PATTERN
Background: Following trauma and SIRS, the typical response is an elevation of the total white cell count (WCC) and a reduction of the lymphocyte count. This leukocytosis typically returns to normal within 48 hours. The persistence of a leukocytosis following trauma is associated with adverse outcomes. Lymphocyte anergy and dysfunction following trauma is associated with increased risk for infection and sepsis, however there is a paucity of data regarding the impact of a persistence of a low lymphocyte count in trauma patients. It is unknown whether lymphocytes return to normal levels with the rapidity of WCC, and whether a persistence of the lowered lymphocyte number impacts mortality. It was our hypothesis that a failure of the lymphocyte count to recover to normal within 4 days following is associated with an increased mortality in trauma patients.
Methods: This is a retrospective review of prospectively collected data from trauma patients collected over the 5 years of September 2003 to September 2008. Patients were included if the Injury Severity Score was ≥ 15, and they survived at least 3 days. Laboratory values for the first 4 hospital days were collected. White cell counts, including the subgroups of absolute neutrophil, bands, and lymphocytes counts, as well as their percentages were collected from the medical records. Demographic data, injury patterns and injury severity, and outcomes were also collected. Proportional hazards regression with time-varying covariates was used to predict time to death based on whether or not cells exited the normal range, and in those that did whether or not they returned to normal.
Results: There were 2448 patients admitted over the 5 years included in analysis. The presence of a leukocytosis following trauma was associated with a 1.7 fold increase in mortality (p = 0.0045). A persistence of the leukocytosis over the 4 days following trauma increased mortality 2-fold (p < .0001) compared with patients who had an elevated white cell count that returned to normal range (4-11). A similar effect was seen with the presence of a bandemia, which was associated with a 1.7-fold increase in mortality (p < .0001), and the persistence of bandemia which independently increased mortality 2-fold (p < .0001). Whilst an initial lowering of the Lymphocyte number did not affect mortality, once lymphocyte count was lowered, a persistently low lymphocyte number over the 4 days was associated with a 1.6 fold increase in mortality (p = 0.0088). This finding was independent of the status of the white cell count, the neutrophils, or the bands.
Conclusion: The neutrophil portion of a SIRS response is well known and generally understood. Whilst lymphocyte anergy and dysfunction is associated with multiple organ failure and infections, there are no data addressing the pattern of lymphocytic loss in SIRS following trauma. This is the first report noting that a failure of lymphocytes to return to normal following trauma is associated with significantly higher mortality. This finding is suggestive of a mechanism whereby patients in SIRS might progress to sepsis and possible death following a traumatic mechanism.
ThakkarRajan KMDMonaghanSean FMDHeffernanDaithi SMD, AFRCSI,AdamsCharles AMD, FACS,ConnollyMichael DMDGreggSheaMDKozloffMatthew SMDCioffiWilliam GMD, FACS
Department of Surgery, Rhode Island Hospital, Brown University
EMPIRIC ANTIBIOTICS PENDING BAL RESULTS IN PATIENTS WITHOUT PNEUMONIA SIGNIFICANTLY ALTERS THE FLORA BUT NOT THE RESISTANCE PROFILE IF A SUBSEQUENT PNEUMONIA DEVELOPS
Introduction: Ventilator-associated pneumonia (VAP) has been reported to occur in up to 25% of mechanically ventilated patients and can have a mortality rate ranging up to nearly 50%. Early diagnosis and empiric antibiotic coverage of VAP are crucial to reducing the mortality. Diagnostic tests can aid in the diagnosis of VAP because clinical findings alone are nonspecific. The clinical pulmonary infection score (CPIS) combines clinical, radiographic, physiologic, and microbiological data in a score to use as an indicator of likely VAP. Given the multitude of pulmonary and radiographic anomalies within trauma patients, culture data is essential for differentiating infective versus non-infective causes of pulmonary dysfunction. Empiric antibiotics are started while awaiting BAL culture data.
We wished to assess the potential impact of empiric antibiotics in trauma patients without pneumonia who then subsequently develop pneumonia during the remainder of their hospital course.
Methods: A retrospective chart review of 436 BAL specimens from 162 patients in our trauma intensive care unit over a 3 year period at a level one trauma center were reviewed. In our trauma intensive care unit once a VAP is suspected patients undergo a bronchoalveolar lavage (BAL) and are started on empiric antibiotic coverage for our institution specific likely organisms. If microbiology data are then negative at 72 hours all antibiotics are then stopped. Pneumonia was definitively diagnosed with microbiology showing >/ = 104 organisms per mL. Institutional review board approval was obtained.
Results: 14 patients with 23 BAL specimens with initial negative BAL specimen subsequently developed a VAP during the same hospital stay. There was a significant increase in percentage of Enterobacter (21% vs 8%) and Morganella (8% vs 0%) VAP in these patients compared to those whose initial BAL was positive for pneumonia. Furthermore the profile of the top two organisms in each group significantly changed. Enterobacter (21%) and Pseudomonas (17%) were the principal organisms in the initial BAL negative group, while the two predominant strains in the initial positive BAL group were Staphylococcus (21%) and Haemophilus (11%). Interestingly, MRSA remained the third most common organism in both groups. Empiric antibiotics did not induce growth of multi-drug resistant organisms. Interestingly, in the empiric antibiotic, initial negative BAL group, there appears to be a trend towards pan-sensitive E. coli and pan-sensitive Pseudomonas.
Conclusion: Ventilator associated pneumonia remains a significant cause of morbidity and mortality in mechanically ventilated patients. The diagnosis and treatment of VAP continues to be a challenge. Once clinically suspected empiric coverage decreases morbidity and mortality. No data exist regarding whether this short course of antibiotics without pneumonia impacts the nature of a subsequent pneumonia. Our data demonstrate that patients who receive empiric coverage with no organism growth are susceptible to a significantly different pathogenic profile compared to those who had an initial positive BAL culture. However, this did not induce multi-drug resistance in these organisms.
KaoLillian SMD, MPH,LewDebbie FMPH,ArabSamer NMDToddS. RobMDCarrickMatthew MMDCorneilleMichael GMDAwadSamir SMDLallyKevin PMD, MS
University of Texas Health Science Center at Houston
LOCAL VARIATIONS IN EPIDEMIOLOGY, MICROBIOLOGY, AND OUTCOME OF NECROTIZING SOFT TISSUE INFECTIONS: A MULTI-CENTER STUDY
Background: Necrotizing soft tissue infections (NSTIs) are rare and highly lethal. An increasing proportion of monomicrobial MRSA infections may be associated with improved outcomes.
Methods: Retrospective chart review of patients with NSTIs treated at 6 academic hospitals (3 county, 2 private, and 1 VA) in Texas (5 in Houston, 1 in San Antonio) between January 1, 2004 and December 31, 2007. Patient demographics, presentation, microbiology, treatment, and outcome were recorded. Analysis of variance, chi-square, and logistic regression analysis were performed.
Results: A total of 296 patients had documented NSTIs (see table). Over half of the infections were monomicrobial (54%), with the most common single pathogen being MRSA. There was a significant difference in the percentage of monomicrobial MRSA infections between hospitals. The etiologies differed significantly between the centers as well; i.e., MRSA infections were associated with intravenous injections and bites. The overall mortality and amputation rates were 16.6% and 8.8% respectively (Table below). Among the hospitals, the lowest rates were associated with higher proportions of MRSA. On univariate analysis, monomicrobial Staphylococcal infections had an OR of 0.32 (95% 0.10-1.07, p = 0.65) for mortality. On multiple regression, independent predictors of mortality included age, shock requiring vasopressors, and renal failure post-operatively.
All (n = 296)
Hospital 1 (n = 68)
Hospital 2 (n = 67)
Hospital 3 (n = 58)
Hospital 4 (n = 60)
Hospital 5 (n = 9)
Hospital 6 (n = 34)
p-value
Mortality (%)
16.6
10.3
11.9
24.1
25.0
22.2
8.8
0.07
Amputation (%)
8.8
16.2
4.5
8.6
11.7
0
0
0.05
Hospital length of stay (days)
27.2 ± 27.4
21.4 ± 19.7
40.7 ± 40.0
24.4 ± 19.9
26.7 ± 22.6
15.3 ± 25.0
21.2 ± 21.6
<0.001
ICU length of stay (days)
16.9 ± 26.0
15.2 ± 21.9
27.1 ± 39.6
12.9 ± 16.0
13.3 ± 17.0
1.7 ± 1.2
10.9 ± 10.1
0.02
Conclusion: Patients with monomicrobial MRSA NSTIs are becoming increasingly common and have improved outcomes compared to other types of NSTIs. Significant differences occur in the etiology, microbiology, and patient outcomes of NSTIs, even within a concentrated region. Collaborative efforts are required to perform multicenter trials of adjunct treatments to improve outcome.
NealMatthew DMDAfraziAminBSSodhiChhinderPhDHackamDavid JMD, PhD
Childrens Hospital of Pittsburgh of University of Pittsburgh Medical Center
TRAFFICKING OF THE TLR4 INHIBITOR IRAK-M VIA NOD2 LIMITS TLR4 RESPONSIVENESS IN INTESTINAL EPITHELIAL CELLS
Introduction: Necrotizing enterocolitis (NEC), a disease characterized by systemic endotoxemia, is the leading cause of death and disability from gastrointestinal disease in preterm infants. Despite this, the pathophysiology is poorly understood. We have established a critical role for toll-like-receptor-4 (TLR4), a receptor whose activity may be inhibited by induction of the cytosolic kinase IRAK-M, in the pathogenesis of NEC (Gribar JI, 2009). Nucleotide oligomerization domain-2 (NOD2), is a pattern recognition receptor that has been linked to intestinal inflammation in Crohn's disease, with mutations in NOD2 leading to an increased susceptibility to Crohn's disease. Based upon this we sought to explore the role of NOD2 in small intestinal inflammation and its interaction with TLR4 a known modulator of intestinal inflammation in NEC.
Methods: TLR4, NOD2, and IRAK-M were assessed by qRT-PCR, SDS-PAGE, and confocal microscopy. IEC6 enterocytes were exposured to LPS (1-50μg/mL) + /− MDP(10-20μg/mL), and we assessed Nf-κB activation by confocal microscopy, IL-6 and iNOS induction by qRT-PCR, and released IL-6 by ELISA. Experimental endotoxemia (5 mg/kg) and experimental NEC (formula gavage and intermittent hypoxia) were induced in wild-type and NOD2-mutant newborn mice + /− MDP, and NEC severity was assessed by blinded pathologist.
Results: IEC-6 enterocytes and murine and human intestinal mucosa expressed TLR4 and NOD2. MDP activation of NOD2 reduced enterocyte TLR4-mediated signaling as measured by attenuated NF-κB translocation and IL-6 induction. MDP did not induce IRAK-M expression in enterocytes, but MDP caused a striking redistribution of IRAK-M within the cell, which formed a complex with TLR4, suggesting a possible mechanism for the inhibitory effects of MDP on TLR4 signaling. Supporting the physiological relevance of these findings, MDP injection reduced mucosal and serum IL-6 release in LPS-injected wild-type mice but not NOD2-mutant mice. Strikingly, administration of MDP significantly attenuated the severity of experimental NEC as compared to mice injected with saline alone. These data reveal a novel pathway by which the NOD2 activator MDP induces IRAK-M to interact with MDP within the cytosol and inhibit TLR4 signaling.
Conclusion: NOD2 activation with MDP attenuates TLR4-mediated signaling in enterocytes, in part through a novel IRAK-M mediated mechanism. These findings shed light on the pathways that lead to intestinal inflammation in diseases of systemic endotoxemia such as NEC.
TungKellyMD, MS,GreenTajia LBSNguyenSally TBSLimDeboraBSChoKihoDVM, PhD,GreenhalghDavid GMD
Shriners Hospitals for Children Northern California/University of California, Davis Medical Center
SINGLE NUCLEOTIDE POLYMORPHISM A829G IN THE TRANSACTIVATION DOMAIN OF THE HUMAN GLUCOCORTICOID RECEPTOR PRODUCES HYPERACTIVITY
Introduction: Inflammation plays a crucial role in the morbidity and mortality of many ill patients. Glucocorticoids and the glucocorticoid receptor (GR) are intricately involved in the inflammatory cascade as a gateway for production of anti-inflammatory molecules. In the care of critically ill patients, treatment algorithms are chosen based on past clinical experience and expectations formed from those experiences. For instance, one would expect that patients of similar health who suffer the same insult would have similar hospital outcomes. However, this is not always the case, thus requiring customization of therapies. The existence of genetic variations in the glucocorticoid receptor causing differential activity in the glucocorticoid pathway could explain the differences in the inflammatory response.
Methods: Previously, we reported from a survey of 100 healthy human volunteers a hyperactive glucocorticoid receptor (HS66-62) containing 3 single nucleotide polymorphisms (SNPs) as well as multiple early termination isoforms exhibiting hypoactivity. In this study, we isolated the 4 SNPs from one of the early termination isoforms, HS22-22, and engineered 2 derivatives from each SNP: one full length GR derivative matching the NCBI reference GR except for the SNP and a truncated GR derivative matching the reference GR except for the SNP and the deletion mutation that caused the early termination. These engineered receptors were cloned into expression vectors and transfected into triplicate sets of TSA201 cells. Luciferase assay was performed to measure the transactivation potential of the GR isoforms.
Results: In the study of the 4 SNPs within HS22-22 (C649T, A829G, G1379A, and T2153G), we unexpectedly identified the full-length GR derivative “A829G” as a hyperactive form with transactivation potential of at least 5 times the reference GR (HS22-14) (p = 0.008) in 7 replicate experiments. Furthermore, the truncated GR derivative of this SNP, “A829G/743,” had a higher transactivation potential (p = 0.003) compared to the truncated GR isoform (GR743) suggesting that the deletion mutation only partially masks the hyperactivity of SNP A829G.
Conclusion: The identification of this novel human GR isoform A829G and its hyperactivity compared with the reference GR, alongside previously identified hyperactive human GR isoforms, further confirm that genetic variations in GR coding sequence can alter transactivation potential. Recognition of patients with these unique GR isoforms can allow for improved customization of anti-inflammatory therapy.
BirdDorothy WMDFordDaleRN, MPH,SulisCarolMDBurkePeter AMDAgarwalSureshMD
Boston University Medical Center
TERMINATION OF HAND HYGIENE SURVEILLANCE IS ASSOCIATED WITH INCREASED NOSOCOMIAL INFECTIONS IN THE SURGICAL INTENSIVE CARE UNIT
Introduction: Hand hygiene is a fundamental yet often neglected aspect of nosocomial infection control in the surgical intensive care unit (SICU). Following a successful hand-washing program at our institution that resulted in dramatically reduced infection rates, our hand-washing surveillance program was terminated. We sought to examine rates of ventilator-associated pneumonia (VAP), catheter-based bloodstream infections (BSI) and Foley-catheter-related urinary tract infections (UTI) since cessation of this program.
Methods: Prospectively-collected data were examined retrospectively from our infection control surveillance database over a 4 month period following termination of hand hygiene surveillance. Our institution is an urban academic level I trauma center with 2 SICUs.
Results: Since cessation of hand hygiene surveillance, VAP has increased from 0.9 to 3.5/1000 ventilator days, BSI has increased from 0 to 0.7/1000 catheter days, and UTI has increased from 2.3 to 6.2/1000 foley catheter days (Figure).
Conclusion: Hand hygiene surveillance is a critical aspect of nosocomial infection control and should be continued, even once excellent results have been achieved, to maintain optimal performance.
ANTIBIOTIC TIME-LAG COMBINATION THERAPY WITH FOSFOMYCIN FOR PATIENTS WITH POSTOPERATIVE INTRA-ABDOMINAL ABSCESS
Introduction: Intra-abdominal abscess is a major complication of gastrointestinal surgery and is often caused by antibiotic-resistant bacteria. The first-line treatment for intra-abdominal abscess is source control. Sometimes, however, source control is too invasive for relatively small abscesses and is not feasible due to the risk of injury to some organs. Based on reports that fosfomycin (FOM) can break up biofilms to enhance the permeability of other antibiotics, we investigated the outcome of treatment of intra-abdominal abscess with FOM administered one hour before the administration of other antibacterial drugs (FOM-TLCT: FOM time-lag combination therapy).
Patients and Methods: We enrolled patients (n = 114) who have intra-abdominal abscess after gastrointestinal surgery at our institution and received FOM-TLCT, between April 1997 and March 2009. Each of the patients enrolled was hospitalized and had failed drainage, reoperation, or sufficient adequate antibiotic therapy to the bacteria isolated from the abscess. We examined the efficacy of FOM-TLCT using the same antibiotic as that which had been used previously (at least 3 days) but had proven ineffective, at the same dosage schedule.
FOM 2.0 g was diluted with infusion fluid and administered by intravenous injection over 30 to 60 minutes. One hour after the end of FOM administration, the previously used therapeutic agents (TA) were restarted. They were administered regardless of whether or not the isolates were sensitive to FOM, except under the condition when the putative pathogenic bacteria were resistant to TA, but sensitive to FOM. FOM was administered before each administration of TA, whether q.d. or b.i.d. The efficacy endpoint determination was carried out as follows: among the SIRS-positive cases even after administration of TA, “Excellent” outcome was defined as a SIRS negative within 7 days of the FOM-TLCT with TA, without the need for other treatment, including other antibiotics or any drainage.
On the other hand, among the SIRS-negative cases after 3 days of TA administration but continued to have high WBC counts (≥10,000) or body temperature (≥37°C), “effective” outcome was defined as a fall of the WBC count and body temperature to 9,000 and 37.0°C or lower, respectively, within 7 days of FOM-TLCT with TA, without more therapies. All the patients underwent a final assessment after a follow-up period of at least 30 days from the start of the FOM-TLCT.
Results: Of the 114 patients enrolled, the data of 104 cases (SIRS-positive: 73, SIRS-negative: 31) were assessed. 10 patients were excluded; 4 had received TA at higher doses, 3 had received different TAs, and 3 were considered to caused by resistant bacterium to TAs.
Among these patients, 89.0% (65/73) of the SIRS-positive cases were “excellent” and 90.3% (28/31) of the SIRS-negative cases were “effective”. The total rate of “excellent” and “effective” were 89.4% (93/104), respectively. The total “no-response” rates were 10.6% (11/104).
Conclusion: FOM-TLCT seems to be effective for the treatment of refractory intra-abdominal abscess.
CarterJeffrey WMDLeukhardtWilliam HMDGolobJoseph FMDFadlallaAdam MPhDClaridgeJeffrey AMD, MS
MetroHealth Medical Center
CHANGES IN LEUKOCYTE COUNT ARE MORE IMPORTANT IN PREDICTING INFECTION THAN ABSOLUTE LEUKOCYTE COUNT IN CRITICALLY ILL TRAUMA PATIENTS
Background: Our previous research has demonstrated that the presence of fever and leukocytosis on a given day is strongly associated with obtaining urine, blood, and respiratory cultures but are not associated with urine, bloodstream, or respiratory infections. We hypothesized that daily changes in white blood cell count (WBC) and maximum temperature (Tm) would be more predictive of infection than absolute daily values.
Methods: Data were prospectively collected on all trauma patients admitted to the Surgical and Trauma Intensive Care Unit (STICU) for >2 days for 20 consecutive months. Data collected included demographics, injuries, daily vitals, daily laboratory results, and culture results. To identify factors associated with infection it was necessary to define both infected patient days and non-infected patient days. Infected days were defined as the day that a positive culture was sent. Non-infected days were defined two separate ways: 1) Strict definition: A patient day when any blood, urine, or respiratory culture was sent and were negative; 2) Liberal Definition: A patient day not within seven days of a confirmed infection day.
Results: Data were analyzed on 750 consecutive trauma patients admitted for >2 days which corresponded to 6277 patient days. The mean ISS and age were 21 and 52 respectively with an average STICU length of stay (LOS) of 9 days. There was a total of 155 infected patient days. Using the strict definition there were 605 non-infected patient days and 5460 non-infected patient days with the liberal definition. Bivariate analysis was preformed to compare infected days to non-infected days using each definition of a non-infected day. There were no associations found when the strict definition of a non-infected day was used. When the liberal definition of a non-infected day was used, bivariate analysis found numerous associations between infected and non infected days (Table).
Infected N = 155
Non-Infected N = 5460
p valure
Age
51.2
51.9
NS
% MALE
72%
71%
NS
ISS
22.2
21.3
NS
ICU day
11.3
10.7
NS
Vent Day
9.9
8.9
NS
Vent
79.6%
62.7%
<0.001
Central line
57.3%
45.2%
0.003
Antibiotics
41.4%
34.9%
0.010
AM Glucose
141
133
0.024
WBC
13.7
12.4
0.063
Tm
38.3
37.7
<0.001
dTm3
1.5
0.4
< .001
dWBC3
18.5
4.0
<0.001
Logistic regression analysis demonstrated that the daily Tm (P < 0.001), morning glucose level (P = 0.015), ventilator status (P = 0.003), change in Tm over 3 days (P = 0.015), and change in WBC count over 3 days (P = 0.001) to be independent predictors of infection.
Conclusion: When non-infection days were liberally defined daily Tm, morning glucose level, ventilator status, change in maximum temperature over 3 days, and change in WBC count over 3 days to be significant variables. These results demonstrate that changes in leukocyte count predict infection better then absolute leukocyte count.
BrownTrevor SPhDHawksworthJason SMDSheppardForest RMDTadakiDouglas KPhDElsterEric AMD
Naval Medical Research Center, Bethesda
THE INFLAMMATORY RESPONSE IN COMBAT WOUNDS IS ASSOCIATED WITH CRITICAL COLONIZATION
Introduction: Modern combat or blast-related injuries are characterized by devastatingly massive zones of injury that violate soft tissue, bone, and neurovascular structures. Up to 80% of surviving victims have sustained major extremity trauma, which accounts for the majority of long-term morbidities, medical expenses, and functional deficits experienced by this patient population. Within our translational research program, we have determined that healing of traumatic combat wounds is dependent on the immune response. While the majority of combat wounds are not critically colonized with bacteria (>105 CFU/gm tissue), there exists a correlation between critical colonization and inflammatory cytokines and chemokines measured in wound effluent or patient serum.
Methods: Patients with penetrating extremity wounds sustained during combat operations were prospectively studied and followed for 30 days after definitive wound closure. Surgical debridement was repeated every 48–72 hours until wound closure, which was at the discretion of the attending surgeon. Serum, wound effluent, and a wound bed tissue biopsy were collected at each surgical debridement. Serum and wound effluent were analyzed with a multiplex assay for cytokines, chemokines, and inflammatory proteases while wound tissue was assessed for microbial colonization with quantitative cultures (QC). Correlations between serum and effluent cytokines and chemokines and the degree of tissue colonization were evaluated.
Results: Samples from 150 wound debridements in 40 wounds (mean size 259 ± 418 cm3) from 26 male patients (mean age 23 ± 5) were investigated. Many of the patients sustained multi-system trauma (mean Injury Severity Score (ISS) 23 ± 13) and were critically ill (mean APACHE II score 8 ± 6). Wound failure occurred in 9 (22.5%) wounds. A marked inflammatory profile was associated with levels of critical colonization (>105 CFU/gm tissue) with increased serum (IL-6, IP-10 IL-10, TNF-α, and MMP-7) and wound effluent (IL-1β, IFN-□, IL-8, IL-10, and MIP-1α) cytokines and chemokines, p < 0.05.
Conclusions: The correlation between the systemic and local inflammatory cytokines with QC suggests that the interplay between the systemic response to injury and the local wound environment is a determinant of outcome. This relationship remains ill defined and requires further investigation in both clinical and pre-clinical studies. Additionally, a biomarker panel reflective of colonization may provide clinically useful, objective criteria indicating when wound closure is appropriate for successful healing.
GerlachAnthony TPharmD, BCPS,MurphyClaire VPharmD, BCPS,ThomasSheelaMS, RD, LD,PourzanjaniLydiaRD, LD,StawickiStanMDSteinbergStevenMDWhitmillMelissaMDCookCharles HMD, FACS, FCCM
The Ohio State University
DOES WITHHOLDING EARLY INTRAVENOUS FAT EMULSION FROM PARENTERAL NUTRITION REDUCE INFECTIONS DURING CRITICAL ILLNESS?
Introduction: Previous published research demonstrated withholding intravenous fat emulsion (IVFE) from parenteral nutrition (PN) for the first 10 days of PN decreases infectious complications (IC) in trauma patients. Based on this observation we began delaying IVFE for the first 7-10 days of PN in all surgical intensive care unit (SICU) patients. Prior to this IVFE was infused at PN onset. The objective of this study was to compare infectious complications in SICU patients receiving PN before and after routinely delaying IVFE.
Methods: SICU patients before and after our change in IVFE onset who received PN for >6 days were included. Patients receiving PN with IVFE prior to SICU admission or other lipid emulsion therapy such as propofol were excluded. Data collected included patient demographics, transfusion requirements, laboratory and microbiology data, and nutritional assessments. Measured IC included blood infections and catheter-related blood stream infections (CRBSI, defined by isolation of the same organisms from central line and peripheral cultures), pneumonia (defined as >10,000 cfu/mL by semi-quantitative non-bronchscopic BAL plus clinical symptoms), and urinary tract infections (>100,000 cfu/ml by urine culture). Statistical analysis was performed using Fisher's exact test, Student's t-test, and multivariate logistic regression.
Results: Sixty-four patients were included for analysis including 3 trauma patients; 30 received IVFE at onset and 34 had delayed IVFE. Both groups had comparable demographics, severity of illness, transfusion requirements, and duration of PN. Overall hospital mortality was 64.0%, and IC occurred in 65.6% of patients (63.3% IVFE at onset vs 67.6% delayed IVFE, p = 0.79). Seventeen patients developed blood infections or CRBSI while on PN (26.7% IVFE group vs 26.5% no IVFE, p > 0.99). Patients who developed bacteremia or CRBSI had a statistically longer duration of PN (32.5 + /-30.3 vs. 14.7 + /-8.1 days, p = 0.013)
Conclusion: Delay of IVFE therapy for 7-10 days does not appear to influence the rates of infectious complications or mortality in SICU patients requiring PN. However, a longer duration of PN was associated with an increased incidence of bloodstream and CRBSI. The benefit of delaying IVFE in trauma patients does not appear to be generalizeable to all critically ill SICU patients.
IVFE @ onset (n = 30)
IVFE delayed (n = 34)
p-value
% at least 1 IC
63.3
67.6
0.79
% Pneumonia
50
55.9
0.80
% UTI
30
32.4
>0.99
% Bacteremia
20
20.6
>0.99
% CRBSI
6.7
11.8
0.68
Mean duration PN, days
19 ± 16.3
22.4 ± 23.1
0.52
Mean Total Kcal
1650 ± 302
1596 ± 317
0.49
Mean gm AA
99.9 ± 23.8
104.8 ± 25
0.40
SunQianMDBilliarTimothy RMDScottMelanie JMD, PhD
University of Pittsburgh
HYPOXIA-INDUCED UPREGULATION OF AUTOPHAGY IN MOUSE HEPATOCYTES IS DEPENDENT ON CASPASE-1
Introduction: Activation of the inflammasome by reactive oxygen species (ROS) produced during ischemia/reperfusion and hemorrhagic shock leads to maturation of caspase-1, which cleaves pro-inflammatory cytokines (IL-1β, IL-18) and causes their subsequent release. It is known that hypoxic conditions can induce autophagy in many cell types. It has previously been shown that autophagy can negatively regulate inflammasome activation, thus playing a protective role in inflammatory bowel disease. However, the correlation between inflammasome activation and autophagy in hepatocytes is unknown. Therefore in this study we investigated the role of caspase-1 in regulating the autoghagic pathway under hypoxic conditions in mouse hepatocytes.
Methods: Hepatocytes from C57BL/6 (WT) and caspase-1-/- mice were cultured for 2, 6, 18 or 24h under hypoxic (1% oxygen) and normoxic conditions. Similar sets of WT hepatocytes were pre-treated with caspase-1 inhibitor (50μM) or DMSO control for 2 h before hypoxia. Cell viability was determined by crystal violet assay. Whole cell lysates were collected and immunoblotted for caspase-1 and autophagic markers (LC3, beclin-1). Experiments were performed in triplicate and have been repeated three times. Statistical significance: p < 0.05 by Student's t-test.
Results: Caspase-1 was activated (cleaved) in hepatocytes after 2 h of hypoxia and in a time-dependent manner indicating inflammasome activation (see figure). LC3 and beclin-1 levels in WT hepatocytes were significantly increased over time under hypoxic conditions. LC3 and beclin-1 levels were significantly lower in caspase-1 -/- hepatocytes in comparison with WT hepatocytes (see figure). Similarly, pre-treatment of hepatocytes with caspase-1 inhibitor prevented the up-regulation of beclin-1 and LC3 in hypoxia. Cell viability was not significantly different between comparable experimental groups.
Conclusion: Our data show that hypoxia induces activation of the inflammasome and caspase-1cleavage, as well as activating autophagy pathways in hepatocytes. Upregulation of autophagy markers beclin-1 and LC3 are also partially dependent on caspase-1 activation. Elucidating mechanisms of autophagy activation and inflammation may help understand the regulation of inflammation after severe trauma and sepsis.
PalacioCarlos HMDMusherDaniel MMDNuilaRicardo EMDSubramanianAnuradhaMDGreenDavid MMD, BS,AwadSamir SMD
Baylor College of Medicine
MRSA CARRIER STATUS OF PATIENTS PRESENTING WITH SKIN AND SOFT TISSUE INFECTIONS
Background: MRSA skin and soft tissue infections (SSTIs) have significantly increased over the past decade. Little evidence exists regarding the MRSA carrier status of patients presenting with SSTIs. Our objective was to study the MRSA nasal carrier status in patients who present with SSTIs. Our hypothesis is that patients who present with MRSA SSTIs will have a higher MRSA carrier status.
Methods: A prospective database of patients presenting with SSTIs who require incision and drainage in the operating room was queried from September 2007 to 2009. Since 2005, all patients admitted to our facility are screened for MRSA carrier status as part of the MRSA prevention bundle. MRSA nasal swabs were performed with the Cepheid GeneXpert® PCR test. For each patient, demographics, comorbidities, admission nasal swab results and wound culture results were collected. All data are presented as mean + /-SEM. Chi square and student t test were used for statistical analysis.
Results: During the study period, 282 patients had both, admission PCR nasal screening as well as wound culture results. The mean age was 59.4 +ߙ/−10 years, 270 (96%) were males and the majority 195 (69.1%) were Caucasian. Of all the nasal swab tests, 105 (37%) were MRSA + . In contrast, 177 (63%) were MRSA − . When both groups were compared, there were no difference in comorbidities except for chronic renal failure (p < 0.01) and smoking (p < 0.003). Of those patients who were carriers of MRSA, 77 (73%) had a + MRSA wound culture. In contrast, patients who were non-carriers for MRSA 29 (16%) had a MRSA + wound culture. The odds of having been an MRSA SSTI was 14 times greater in MRSA carriers compared with non-carriers (95% CI : 7.8-25.2; p < 0.001).
Conclusion: In patients presenting with SSTI, having an MRSA-positive carrier status significantly increases the likeli-hood of having MRSA SSTI. Therefore targeted antibiotics that treat MRSA infections should be initially considered in patients presenting with SSTIs who are MRSA positive on admission screening. Given that MRSA carrier status can be performed using PCR technology with rapid results appropriate targeted antibiotics for MRSA SSTIs can be now be started earlier.
BecherRobert DMDHothJasonMD, PhDNeffLucas PMDReboJerry JPharmD,MartinRobert SMDMillerPrestonMD
Wake Forest University Medical Canter
MULTIDRUG-RESISTENT PATHOGENS AND INITIAL EMPIRIC ANTIBIOTIC THERAPY FOR PNEUMONIA IN THE TRAUMA VERSUS SURGICAL INTENSIVE CARE UNIT
Background: The role of the trauma surgeon is evolving into the acute care surgeon, caring for critically-ill general surgery and trauma patients. These two patient-populations are unique, and infectious complications may need to be addressed differently as causative organisms may not be the same in both groups. To study this, we evaluated ventilator-associated (VAP) and hospital-acquired (HAP) pneumonia in patients in the trauma (TICU) and general surgical (SICU) intensive care units to investigate differences in VAP/HAP pathogens. Our hypothesis was that SICU patients would have a higher incidence of multiple drug resistant (MDR) organisms causing VAP/HAP, possibly contributing to inadequate empiric antibiotic (IEA) coverage.
Methods: Retrospective review of 123 patients admitted to the TICU or SICU at a tertiary medical center over a one year period with a diagnosis of VAP and/or HAP; SICU patients included those from both elective and emergency operations. Culture by bronchial alveolar lavage (BAL) or quantitative deep tracheal aspirate was followed by initiation of empiric antibiotics in both units based upon an antibiotic algorithm derived from trauma patients. Patient-specific risk factors were assessed; MDR organisms were recorded (defined as any organism that was resistant to at least 3 different classes of antibiotics).
Results: 72 patients in the TICU had 85 occurrences of VAP/HAP, and 50 patients in the SICU were diagnosed with 72 occurrences of VAP/HAP during the study period. Of the first pneumonias, 31.9% were caused by MDR organisms in the TICU, while MDR pathogens caused 68% of the VAP/HAP in the SICU (p-value <0.0001). Concomitantly, SICU patients had a significantly higher rate of recurrent pneumonias compared to TICU patients (30.5% versus 15.3%; p-value 0.022). IEA coverage was seen in 42% of first SICU pneumonias and 48.6% of all SICU pneumonias using the trauma-based antibiotic algorithm.
Conclusion: Multidrug-resistent (MDR) bacterial pathogens cause a significantly greater number of VAP/HAP in the SICU compared to the TICU. Associated with this, when using an antibiotic algorithm based on TICU bacterial pathogens, there is an increased likelihood of IEA coverage and recurrent pneumonias in the SICU patient population when compared to the TICU. Our results indicate that these distinct patient-populations have different pathogens causing VAP /HAP and affirm the necessity for population-specific antibiograms to tailor empiric coverage for presumed VAP/HAP.
HranjecTjasaMD, MD,SwensonBrian RMD, MS,DossettLesly AMDMetzgerRosemarieMD, MPHRosenbergerLaura HMDPolitanoAmani DMDPopovskyKimberly ARN,MayAddison KMDSawyerRobert GMD
University of Virginia
SIGNIFICANT DIFFERENCES IN SERUM CYTOKINE LEVELS BETWEEN INFECTED ELDERLY AND YOUNGER ADULTS ADMITTED FOR CRITICAL CARE
Introduction: Immunosenescence, the concept of age-related immune dysfunction, is believed to increase the risk of infections in the elderly and lead to poorer outcomes. We hypothesized that a differential expression and imbalance of anti- and pro-inflammatory cytokines rather than a global decline in the host defense system would characterize the immune response in infected elderly patients when compared to younger patients.
Methods: This five-year study (10/01 to 05/06) included elderly (≥65 y. o.) and adult (<65 y. o.) patients admitted to the surgical intensive care unit for the treatment of infection at two academic, tertiary care hospitals. Demographics, severity of illness (APACHE II score), and microbiological variables were collected at the time of ICU admission. Patients were followed until discharge or death. Blood specimens were collected within 48 hours of ICU admission; cytokine analysis for IL-1, − 2, − 4, − 5, − 6, − 8, − 10, − 12, IFN-γ and TNF-α was performed using ELISA. Means and medians of admission cytokines and cytokines adjusted for initial severity of illness (cytokine level divided by APACHE II score) were compared by using the Satterthwaite/Student's t-test and Mann-Whitney U test, respectively.
Results: 290 infected, critically ill patients had complete cytokine data. The mean APACHE II scores were 21.5 ± 0.7 in elderly and 18.7 ± 0.5 in younger adults (p = 0.0016). The overall, in-hospital mortality rates were 40/87 (46%) and 50/203 (24.6%) in elderly and younger adults, respectively (p = 0.0003). Compared to patients <65 years old, patients ≥65 years old had lower severity of illness adjusted IL-12 levels, but higher adjusted and non-adjusted levels of IL-4 and TNF-α. Other cytokine levels were relatively similar between groups.
Conclusion: Infected, critically ill, elderly patients have a different cytokine response to infection when compared to younger adults. The elderly may exist in a state of physiologic imbalance with disequilibrium between pro- and anti-inflammatory cytokines. While the elderly have a tendency to secrete higher concentrations of the anti-inflammatory cytokine IL-4 in response to infection, levels of pro-inflammatory cytokines show a mixed profile. Understanding these differences in immune response between younger and older patients may allow for future interventions to decrease mortality among the aged.
MargreiterChristianMDBergerNatalieMDKafka-RitschReinholdMDMargreiterRaimundMDSteurerWolfgangMDPratschkeJohannMDMarkWalterMDBonattiHugo JRMD
Surgery, Innsbruck Medical University
SPECTRUM OF PATHOGENS ASSOCIATED WITH INTRAABDOMINAL INFECTION AFTER PANCREAS TRANSPLANTATION WITH ENTERIC DRAINAGE
Background: Intraabdominal infection (IAI) represents a serious complication after pancreas transplantation (PTx) with enteric drainage (ED).
Patients and methods: 45 out of 217 patients (20,7%) undergoing PTx between March 1997 and August 2004 at our center developed IAI. Immunosuppression included ATG, Tacrolimus, MMF and steroids.
Results: One-year survival of patients with peripancreatitis was 79% as compared to 90% for those individuals without IAI (p = 0.046). Three of the 45 patients with IAI died during follow up unrelated to peripancreatitis from myocardial infarction (n = 2) and invasive aspergillosis (n = 1), one with a functioning graft. Another eleven patients (24%) lost the pancreas graft, eight directly due to the peripancreatitis and another who underwent resection of the necrotic tail of the graft during the later course. Two patients lost the graft due to rejection and non-compliance. In the remaining 36 cases (80%), IAI was successfully managed by antimicrobial therapy and percutaneous drainage (n = 8) and laparotomy (n = 30). A total of 138 organisms were cultured including gram-positive cocci (n = 69), gram-positive rods (n = 6), gram-negative rods (n = 35), non fermentative bacilli (n = 13), anaerobes (n = 7), and fungi (n = 8). Median donor age of patients with IAI was 36 years as compared to those without IAI with 28 years (p < 0.0001), whereas recipient age and cold ischemic time did not differ. Addition of fluconazole to the antimicocrobial prophylaxis and switch from amoxicillin/clavulanic acid to Piperacillin/tazobactam both significantly reduced the incidence of IAI. CMV match and rejection episodes did not influence the rate of IAI.
Conclusion: IAI represents a serious complication after PTx with enteric drainage, with a diverse spectrum of pathogens. Meticulous microbiological surveillance is recommended. Percutaneous drainage or laparotomy should be generously indicated. By this approach the vast majority of grafts can be salvaged.
GoettlerClaudia EMD, FACS,SchlitzkusLisaMDSagravesScott GMD, FACS,HastyChristopher CMDRotondoMichael FMD
East Carolina University, Brody School of Medicine
ORTHOPEDIC INJURIES-–IT DOESN'T COME OUT IN THE WASH
Introduction: Though early washout of open fractures is considered optimal, there is controversy as to timing and necessity depending on injury grade. As the only major trauma care provider in a large rural area, long times between injury and arrival at our center results in an essentially randomized time to washout, allowing us to evaluate this as a factor in orthopedic complications.
Methods: Patients and each fracture were retrospectively reviewed over 6.5 years (3/00-7/07) evaluating for demographics, injury severity, location & mechanism, Gustilo fracture grade, time from injury to initial washout, and were compared to orthopedic wound-related complication rates.
Results: 1,487 open fractures were reviewed in 1,278 patients. Time from injury to washout was 26 to 4,749 minutes (510 mean) with no washout in 48 patients. Overall 8.2% (122) of fractures had an orthopedic complication, rates of which increased with high severity (ISS, AIS & Gustilo classifications) blunt injuries, not related to time to washout. Penetrating injuries likewise showed no difference in complication rates based on time to washout. Lower extremity fractures had a higher rate of complication compared to upper extremity (OR 2.2), likely due to grade of fracture. On multiple regression analysis, only fracture grade, RTS and male gender were independent predictors of wound complication; penetrating trauma was predictive of low risk. Time to washout was not an independent predictor of wound complication.
Conclusion: While grossly contaminated fractures should not be left unattended, degree of initial injury based on fracture grade and physiology (RTS) was predictive of orthopedic wound complications, while time to washout was not. Hence, there is little benefit to washout in Gustilo grade 1/AIS 1 fractures or penetrating injuries, regardless of grade, and adherence to a specific time to washout is also not beneficial.
LapchakPeter HMSc, PhD,KarianPeterRaniPoonamMSc,KannanLakshmiPhDLuccaJurandir J DalleMDTsokosGeorge CMD
Beth Israel Deaconess Medical Center and Harvard Medical School
PLATELET FACTOR 4 (PF4; CXCL4) PROMOTES REMOTE LUNG INJURY FOLLOWING MESENTERIC ISCHEMIA AND REPERFUSION
Introduction: Ischemia reperfusion (I/R) injury is a leading cause of morbidity and mortality and is characterized by platelet dysfunction with increased platelet aggregation, destruction of villi and intestinal integrity, and by immune cell infiltration into the intestinal lumen. Few studies have addressed whether platelets and their products play a principal role in the host response to I/R injury. One platelet protein, platelet factor 4 (PF4) comprises over 3% of alpha granule proteins, is chemotactic for neutrophils and induces neutrophil and monocyte arrest on vascular endothelium. We tested the hypothesis that mesenteric I/R injury results in platelet activation, the release of PF4 from alpha granules, PF4-mediated monocyte and neutrophil recruitment and arrest which lead to remote (lung) tissue damage.
Methods: Wild type (WT; C57BL/6J) and WT mice depleted of platelets underwent mesenteric ischemia for 30 minutes and reperfusion for various times. Intestinal and lung injury were evaluated by histology. Platelet deposition and PF4 levels in intestine and lung were determined by immunocytochemistry.
Results: Wild type mice that underwent mesenteric I/R injury had increased tissue damage over time after reperfusion. However, no increase in platelets was observed in intestines nor was PF4 present. Lung tissues were next evaluated for remote injury. There were increased numbers of platelets, monocytes and neutrophils in the lung vasculature and associated with vascular endothelium within lung with increased reperfusion times ranging from 1.5-20 hours. PF4 levels were significantly increased in lung after I/R injury and further increased with time. There were increased numbers of intravascular neutrophils and monocytes early and their arrest on vascular endothelium later was associated with PF4 levels. Platelet-deficient WT mice did not present with intestinal or lung tissue damage, did not have significant numbers of intravascular monocytes and neutrophils or significant levels of PF4.
Conclusions: These findings suggest that platelets, which become activated during mesenteric I/R injury, sequester in the lung vasculature where they orchestrate remote tissue injury. Release of platelet-derived PF4 recruits monocytes and neutrophils to the lung where they participate in mediating remote tissue injury. PF4 represents a suitable therapeutic target to limit remote tissue injury.
LeonCarlos A TacheMDHranjecTjasaMDBrianSwensonMDPopovskyKimberly ARN,SawyerRobert GMD
University of Virginia
TWELVE-YEAR EXPERIENCE WITH SEVERE CANDIDA INFECTIONS: DECREASING MORTALITY, EVOLVING EPIDEMIOLOGY, AND EMERGENCE OF NEW ANTIFUNGALS
Background: During the last two decades, the clinical significance of systemic fungal infections has become painfully apparent, and candidiasis in particular is a challenge in the patient with intra-abdominal infection, receiving parenteral nutrition, or on renal replacement therapy, diabetic, post-transplant, and sometimes even in those without mayor risk factors. Clearly associated with high mortality and poor outcomes it seems appropriate to take a closer look at our institutional experience.
Methods: We performed a retrospective review of all documented episodes of severe Candida infections, with microbiology confirmation, between December of 1996 and December of 2008. All these patients were treated in the surgical units at the University of Virginia Health System. The data have been collected prospectively in our institutional infectious diseases database. Non-albicans isolates were compared with the documented instances of Candida albicans, with mortality as our primary outcome variable. The information was analyzed chronologically, dividing the whole data set in periods of 1 year of duration.
Results: A total of 1112 cases of candidiasis in adults where evaluated. Our patients' mean APACHE II score was 16 (SD 0.2), throughout the whole period; we found an equal distribution among sexes, and average age of 55 years old (SD 15.9). The presence of albicans vs non-albicans isolates did not result in different outcomes, with overall mortality of 20% in both groups. On the other hand, over the 12 years of data we clearly observed a statistically significant decline in mortality from 29% to 16% (p < 0.001), specially since the introduction of echinocandins such as caspofungin first and then anidulafungin to the clinical practice. The incidence of C. albicans isolates decreased from 68% to 49% over time with increase in the relative (and absolute) frequency of C. glabrata and other species.
Conclusion: The changes in the epidemiology of Candida infections, along with the severity and number of associated conditions of our patients, present a formidable challenge in our daily practice. Newer agents, and the overall improvement in the care of the critically ill, have allowed us to treat and save patients that didn't stand a chance in the past, but we are also seeing the emergence of resistance to antifungals, and more complex clinical scenarios, making it mandatory to maintain our vigilance decreased from 68% to 49% over time with increase in the relative (and absolute) frequency of C. glabrata and other species.
DuaneTherese MMDBrownHollyBSWolfeLuke GMS,MalhotraAjai KMDAboutanosMichel BMD, MPH,IvaturyRao RMD
Virginia Commonwealth University
BLADDER PRESSURE MEASUREMENTS ARE AN INDEPENDENT PREDICTOR OF UTI IN TRAUMA PATIENTS
Introduction: Nosocomial infections are associated with significant increases in morbidity and mortality. Blood stream infections (BSI), ventilator-associated pneumonia (VAP), and urinary tract infections (UTI) in critically injured patients result in increased resource utilization and decreased survival. Many institutions have successfully incorporated ICU protocols to decrease these infections. At our institution we have demonstrated a significant drop in both BSI and VAP; however, we have continued to struggle with high UTI rates.
Hypothesis: The purpose of this trial was to determine risk factors for UTI specific to trauma patients to assist in the development of infection control protocols.
Methods: Data were collected prospectively from 1/03 until 12/05 by a dedicated epidemiology nurse and combined with data from the trauma registry at our Level 1 trauma center. All trauma patients admitted to the surgical trauma ICU (STICU) with and without UTI's were compared for demographics, injury severity (ISS), and epidemiologic data including foley use and bladder pressure measurements (BPM). CDC definitions were used to diagnose UTI. BPM were performed when there was a concern for intra abdominal hypertension. An open system was used in which the Foley was disconnected from the bag to insert 50 cc of saline into the bladder and then an 18-gauge needle was inserted into the foley itself to measure pressures.
Results: A total of 938 patients were included in the trial. There were 50 patients with no Foleys or UTIs,
836 patients with Foleys but no BPM with 36 having a UTI (4.31%) and 52 patients who had Foleys and BPM of whom 12 had UTIs (23.08%) (p < 0.0001). As shown in Table 1 patients with UTIs were more likely to be more severely injured older women.
No UTI
UTI
P value
Age
40.1 ± 18.6
48.5 ± 20.8
0.0083
% Female
26.4 (235/890)
45.83 (22/48)
0.007
ISS
19.3 ± 11.3
26.2 ± 11.6
<0.0001
Ventilator LOS (days)
1.5 ± 4.9
6.9 ± 12.2
0.0069
ICU LOS (days)
6.6 ± 10.4
22.6 ± 31.8
<0.0001
Hospital LOS (days)
13.4 ± 15.3
48.9 ± 45.0
<0.0001
Using logistic regression, BPM was an independent predictor of UTI with it being 7 times more likely to occur in these patients (OR: 6.99, 3.087-15.827). Along with age (OR: 1.039, 1.024-1.054), and ISS (OR: 1.081, 1.056-1.106), having BPM was an independent predictor of mortality (OR: 2.475, 1.191-6.328).
Conclusion: Our findings are consistent with other trials that demonstrate that severely injured women are more likely to develop UTIs. However, this is the first study that demonstrates increased risk of UTI with BPM using the open technique independent of gender or degree of injury. Given these findings and a previous trial demonstrating no difference in UTI rates with a closed circuit for BPM, our institution has incorporated a closed circuit technique into its infection control protocol. This protocol is currently being studied with the hope that its findings will help refine further BPM protocols resulting in decreased UTIs and improved outcomes.
Poster Presentation Abstracts
KusachiShinyaMD, PhDTakahashiYoshikiMD, PhDKatoKoumeiMD, PhDOdaShigetoMD, PhDTakeyamaHiromitsuMD, PhDMashitaKeijiMD, PhDKobayashiShinichiPhDSumiyamaYoshinobuMD, PhD
Japan Society of Surgical Infection
A MULTICENTER, RANDOMIZED,CONTROLLED CLINICAL TRIAL COMPARING CIPROFLOXACIN WITH MEROPENEM FOR TREATMENT OF POSTOPERATIVE INFECTIONS, FINAL REPORT OF POSTOPERATIVE INFECTION TREATMENT STUDY GROUP OF JAPAN SOCIETY FOR SURGICAL INFECTION
Introduction: Despite numerous reports on injectable ciprofloxacin (CIP) for the treatment of severe infections, the usefulness of CIP with the Japanese dosage regimen (300 mg b.i.d.) for the treatment of postoperative infections has not been clearly determined. The aim of this study was therefore to compare the efficacy and safety of CIP with injectable meropenem (MEPM) in patients with postoperative infections.
Methods: Thirty-nine medical centers in Japan participated in the study and enrolled 205 patients from Jun 2005 through May 2008. Patients were randomized to receive either CIP (300 mg b.i.d.) or MEPM (500 mg b.i.d.) for empirical treatment of postoperative infections after elective gastroenterological surgery followed by administration of prophylactic antibiotics. Postoperative infection was defined as: Surgical site infection, remote infection, SIRS-positivity, or suspected SIRS-positivity. The primary endpoints were clinical and bacteriological responses and adverse drug reactions. Clinical efficacy was comprehensively assessed based on clinical signs and symptoms and laboratory findings. The secondary endpoints were period of treatment with antibiotics and relapse rate.
Results: There were no significant differences in any 3 primary or 2 secondary endpoints between the two treatment groups. At the end-of-study assessment, the overall clinical response rate for the per-protocol (PP) set was 85.3% (64/75 patients) in the CIP group and 89.6% (69/77 patients) in the MEPM group. Both groups exhibited good clinical response, but it could not demonstrated that CIP is not inferior to MEPM; (difference, − 4.3% 95% CI, − 14.8 to 6.2%). On bacteriological assessment, a clinically significant pathogen was isolated in 69 of 152 PP patients (45.4%, 36 in CIP group, 33 in MEPM group). Overall bacteriological efficacy was 78.1% (25/32 patients) in the CIP group and 55.2% (16/29 patients) in the MEPM group. The incidence of adverse drug reaction was 7.0% (7/100 patients) in the CIP group and 7.8% (8/103 patients) in the MEPM group. The mean treatment period for PP patients was 8.0 ± 6.1 days (±SD) in the CIP group and 7.3 ± 7.7 days (±SD) in the MEPM group. The rates of relapse of infection after successful treatment were 3.1% (2/64 patients) in the CIP group and 2.9% (2/69 patients) in the MEPM group
Conclusion: The above findings suggest that empirical monotherapy with CIP is useful for postoperative infections after gastroenterological surgery.
HoVanessa PMDBariePhilip SMD, MBASteinSharon LMDTrenchevaKoianaMSMilsomJeffrey WMDLeeSang WMDSonodaToyookiMD
Weill Cornell Medical College
ANTIBIOTIC REGIMEN AND TIMING OF PROPHYLAXIS ARE IMPORTANT FACTORS FOR LIMITING SURGICAL SITE INFECTION (SSI) IN ELECTIVE ABDOMINAL COLORECTAL SURGERY (eCRS)
Background: Surgical site infections (SSI) cause morbidity after eCRS, and antibiotic prophylaxis can decrease SSI. This study hypothesized that antibiotic administration factors (AAF) reduce the risk of SSI.
Methods: Retrospective review from a prospective database of a random sample of patients with eCRS with anastomosis. Antibiotic regimens, initial dose timing (IDT), and redosing were evaluated. Appropriate regimens (APC) covered gram-positive cocci, gram-negative bacilli, and anaerobes. IDT was proper if given <30 min prior to incision; redosing parameters were determined pharmacokinetically for each agent. The main outcome was SSI (CDC definitions). Sequential logistic models were generated: Model 1 assessed AAF, Model 2 controlled for patient and clinical factors^; α = 0.05*.
Results: 605 patients (292 male (48.3%), mean age 59.7 (SD 17.8) years) were included; diagnoses included cancer (235, 38.8%), IBD (133, 22.0%) and diverticulitis (107, 17.7%). 76 patients (12.6%) had incisional SSI and 54 (8.9%) had organ/space SSI. Regimens included cefazolin (CZL) + metronidazole (MET) in 219 (36.2%), cefoxitin (FOX) in 214 (35.4%), and levofloxacin (LFX) + MET in 48 (7.9%); 124 (20.5%) utilized other regimens (OTH). 55 (9.1%) received insufficient coverage, 356 (58.8%) had proper IDT, and 401 (66.3%) regimens were redosed properly. In Model 1, OTH regimens increased SSI risk, and proper IDT was protective (Table). After adding clinical factors (Model 2^), IDT remained protective; but increased OTH risk approached significance.
Conclusions: Appropriate antibiotic selection and timing of administration for prophylaxis are most crucial to limit SSI in eCRS.
disease, surgeon experience, transfusion, wound class, type of surgery, history of radiation, [albumin], comorbidities, intraoperative factors [Temp, PO 2], glycemic control, ICU admission
FinkDavidMDRomanowskiKathleenMDBabrowskiTrissaMDValuckaiteVestaMDZaborinAlexPhDPoroykoValeriyPhDMorozovaIrinaMSZaborinaOlgaPhDAlverdyJohnMD
University of Chicago
MEASURING SPATIAL DIFFERENCES IN PSEUDOMONAS AERUGINOSA DISTRIBUTION AND VIRULENCE ACTIVATION RELATED TO INTESTINAL ISCHEMIA-REPERFUSION INJURY
Background: The precise mechanism by which intestinal microbes influence the development of sepsis leading to mortality remains to be elucidated. Although altered barrier function and systemic absorption of microbes and their products is hypothesized to be an important element of this process, equally important may be the degree to which intestinal microbes express enhanced virulence both in the gut and remote organs. In the current study, we have developed a comprehensive approach to this problem using photon-camera-based detection of propagation (growth), dissemination, and virulence expression of intestinal bacteria using two strains of bioluminescent bacteria.
Methods: The Xenogen system was used to capture images of luminescent strains of Pseudomonas aeruginosa. Mice (n = 3 per group) underwent either sham laparotomy or 15 minutes of intestinal ischemia reperfusion (IIR) via superior mesenteric artery occlusion. At surgery, either XEN41 (constitutively luminescent strain of P. aeruginosa) or PAO1/lecA::lux (inducible expression of barrier disrupting lecA protein) were injected into the terminal ileum. 12 hours post-operatively animals were sacrificed and their organs immediately imaged ex-vivo using the Xenogen system. Spatial regions of interest were defined around each organ or portion of the gastrointestinal tract and the total photon count from each area was quantified. In reiterative experiments, mouse mortality was followed.
Results: Xenogen analysis of propagation and distribution of constitutively luminescent P. aeruginosa XEN41 demonstrated that intestinal IIR had a significant effect on the regional distribution of bacteria whereby P. aeruginosa was found to migrate from the site of injection (distal ileum) toward the site of injury (jejunum) (3.82 fold increase IIR versus Sham). Bacterial growth was not affected by IIR. Intriguingly, we found a lower dissemination rate of P. aeruginosa following IIR versus Sham where mesenteric lymph node (MLN) photon counts were 49% lower in IIR compared to Sham. Virulence expression using inducible PAO1/lecA::lux demonstrated that despite lower total number of bacteria in organs from IIR mice, the “virulence signal” was 10.56 times higher in the IIR mice compared to sham. Increased virulence of P. aeruginosa was associated with enhanced lethality of 15 min of IIR mice (data not shown).
Conclusion: Approaches assessing both bacterial counts, dissemination, and site-specific virulence expression using constitutively and inducible bioluminescent bacterial strains may shed new light on how intestinal microbes contribute to sepsis and mortality.
Average Photon Counts Per Organ
IIR XEN
Sham XEN
IIR/Sham
GI Tract
2.92 × 107
2.38 × 107
1.23
Colon
3.32x106
2.19 × 106
1.52
Cecum
3.35 × 106
1.11 × 107
0.30
Ileum
1.13 × 107
7.59 × 106
1.49
Jejunum
8.02 × 106
2.10 × 106
3.82
Stomach
8.56 × 105
7.76 × 105
1.10
MLN
3.66 × 106
7.12 × 106
0.51
IIR lecA
Sham lecA
IIR/Sham
MLN
1.24 × 105
1.17 × 104
10.56
CarchmanEvie HMDZuckerbraunBrian SMD
University of Pittsburgh Medical Center
THE INFLUENCE OF iNOS ON THE AUTOPHAGIC RESPONSE IN SEPSIS
Introduction: Sepsis results in the exuberant production of nitric oxide (NO) secondary to inducible NO synthase (iNOS). This overproduction of NO is thought to contribute to mitochondrial dysfunction, bioenergetic failure and organ dysfunction. Adaptive cell signaling responses, such as autophagy, prevent the accumulation of dysfunctional mitochondria and other organelles, preventing cell death and organ dysfunction. The purpose of these experiments was to test the hypothesis that sepsis-induced autophagy is dependent on iNOS and subsequent reactive oxygen species (ROS) cell signaling.
Methods: Hepatocytes were harvested from C57BL/6 mice and iNOS knockout mice and treated with 100 ng of LPS for 12 hours. Cells were then either fixed for immunohistochemistry or cell lysates prepared for Western blotting. LC3 protein levels were measured on Western blot analysis and punctate LC3 was used as a marker of autophagy on immunohistochemistry, both well-known methods of measuring autophagy. Hepatocytes were also treated with or without EUK-134, a superoxide dismutase/catalase mimetic that acts as a ROS scavenger, and LC3 protein levels were then measured from whole cell lysates. ROS production was determined by DCF fluorescence in primary hepatocytes as well as the HepG2 cell line or mitochondrial-deficient (rho zero) HepG2 cells. For experimental sepsis, C57BL/6 and iNOS knockout mice underwent cecal ligation and puncture (CLP). Sham animals underwent laparotomy and bowel manipulation without CLP. Liver tissue samples were then examined by immunohistochemistry or protein extraction done for Western blot analysis. Immunohistochemistry and Western blot analysis were done for LC3.
Results: In vivo, CLP results in increased hepatic autophagic signaling as determined by electron microscopy and immunofluorescence. iNOS knockout mice had a decreased autophagic signaling compared to wild type animals in this model of sepsis. As expected, LPS significantly induced iNOS protein expression in C57BL/6 hepatocytes as determined by Western blot analysis and immunohistochemistry. LPS induces autophagic signaling in hepatocytes as determined by Western blotting and immunohistochemical evaluation for autophagic proteins, including LC3; however this induction was significantly attenuated in iNOS knockout hepatocytes. LPS or NO donor, PAPA-NONOate (10 uM) results in increased hepatocyte ROS production as determined by DCF fluorescence. This ROS production was absent in rho zero cells, indicating that ROS are produced by the mitochondria. Moreover, hepatocytes treated with EUK-134 had no evidence of autophagic induction after LPS stimulation, suggesting that induction of this pathway is dependent on ROS signaling.
Conclusion: These data suggest that sepsis-induced iNOS/NO leads altered mitochondrial function and ROS production. These reactive molecules may induce protective adaptive signaling such as autophagy. The contribution of NO to adaptive signaling and autophagic induction, as well as the elucidation of the role of autophagy in organ dysfunction requires further investigation.
BabrowskiTrissa AMDRomanowskiKathleenMDFinkDavidMDLiuDonaldMD, PhDZaborinaOlgaPhDAlverdyJohnMD
University of Chicago
IS THE MORBIDITY OF SECONDARY PERITONITS A RESULT OF THE PATHOGENS EXPRESSING ENHANCED VIRULENCE?
Despite aggressive interventions, mortality rates for secondary peritonitis, which often occurs as a complication of abdominal surgery, remain high. The aim of this study was to develop a novel animal model of intra-abdominal infection that would determine whether micro-environmental factors present in the intestine of a surgically stressed host play a role in the observed high mortality rates.
Methods: In order to expose a human hospital pathogen to the local microenvironment of the intestinal tract in the presence of surgical injury, 7-week male C57BL6 mice were anesthetized and randomly assigned to undergo either sham laparotomy (Sham) or 30% hepatectomy (Hep) with simultaneous inoculation of 107 CFU of Pseudomonas aeruginosa directly into the cecum. 24 hours later all animals were euthanized and their cecal contents collected for subsequent intraperitoneal injection into a separate group of mice. To accomplish this, 0.03 g cecal contents collected from either sham-operated mice (Sham) or hepatectomy mice (Hep) were then implanted into the right lower quadrant of na?ve 7-week male C57BL6 mice subjected to either sham laparotomy (Sham) or 30% hepatectomy (Hep).
Animals were followed for mortality and sacrificed once moribund. Cecal contents were also plated for culture to determine the concentration of bacteria in the stool.
Results: Sham-operated mice intraperitoneally inoculated with cecal contents from sham-operated animals whom had previously been intestinally inoculated with P. aerugionsa (Sham → Sham) were all alive (100% survival) at 24 hours. Mice undergoing hepatectomy (Hep) and intraperitoneal inoculation with cecal contents from sham operated animals previously exposed to intestinal P. aeruginosa (Sham → Hep) had a slightly lower survival rate (66%) (P = NS). However when mice were intraperitoneally inoculated with cecal contents collected from mice undergoing hepatectomy and prior intestinal exposure to P. aeruginosa (i.e. Hep → Sham or Hep → Hep), all mice died of sepsis (100% mortality) (n = 6, p < 0.05). Stool culture from the two groups demonstrated P. aeruginosa incubated in the mouse gut exposed to hepatectomy (Hep), displayed denser growth and expressed a more virulent phenotype, as judged by the production of pyocyanin.
Conclusion: This study presents a new approach to investigate intra-abdominal sepsis by exposing hospital pathogens to the intestinal environment in the presence of surgical injury with subsequent re-introduction of these organisms to the peritoneum of na?ve mice. A more complete understanding of the local microenvironmental cues that shape the virulence of pathogens associated with secondary peritonitis can now be advanced.
LiuQuin YMDMittalRahulPhDGrishinAnatolyPhDFordHenri RMDPrasadaraoNemani VPhD
Childrens Hospital Los Angeles
PROTEIN KINASE C PLAYS A ROLE IN ENTEROBACTER SAKAZAKII-INDUCED INTESTINAL EPITHELIUM PERMEABILITY
Introduction:Enterobacter sakazakii (ES) is a gram-negative bacterium that has been linked to severe outbreaks of necrotizing enterocolitis (NEC) in neonates. Previous studies from our lab demonstrated that ES induces apoptosis in intestinal epithelial cells in a rat model of NEC. We have also shown that ES strains isolated from humans exhibit higher binding affinity to intestinal epithelial cells and lead to greater permeability of intestinal monolayers than ES strains isolated from non-human sources. However, the mechanism by which ES induces tight junction disruption is unknown.
Objective: Because protein kinase C (PKC) has been shown to play a role in intestinal permeability, we sought to determine if PKC mediates the observed increase in intestinal epithelium permeability and alteration in tight junction morphology induced by ES.
Methods: Caco-2 cell monolayers were grown in transwells and treated with either the PKC activator, Phorbol 12-Myristate 13-Acetate (PMA), or the PKC inhibitor, Gö 6983, followed by inoculation with ES and horseradish peroxidase (HRP). The transepithelial electrical resistances (TEER) and HRP leakage were then measured at different time points. In addition, the activity of PKC was measured by non-radioactive PepTag assay in the total cell lysates of Caco-2 cells.
Results: Our data show that exposure to ES increased Caco-2 monolayer permeability (decreased TEER and increased HRP leakage). High-binding ES increased PKC activity by two-fold compared to low-binding ES (20.07 units of kinase/mL compared to 10.4 units of kinase/mL). The PKC activator, PMA, decreased the TEER of the Caco-2 monolayers by 21 – 26% over 4 hours while the PKC inhibitor, Gö 6983, increased the TEER by 9 – 12%. Treatment with the PKC inhibitor, Gö 6983, helped preserve epithelial barrier integrity in Caco-2 monolayers exposed to high-binding ES strains, as evidenced by a decrease in TEER of 18% with Gö 6983 treatment vs. 52% without, and HRP leakage of 230 picograms with Gö 6983 vs. 323 picograms without.
Conclusion: This study suggests that high-binding ES increases Caco-2 cell monolayer permeability by enhancing the activation of PKC, possibly via tight junction disassembly. The isoform of PKC involved in this phenomenon has yet to be determined.
BadalRobertBSBouchillonSamuelMDHackelMeredithPhDJohnsonAaronBS
IHMA, Inc.
COMPARISON OF ANTIMICROBIAL SUSCEPTIBILITY AND INCIDENCE OF EXTENDED-SPECTRUM BETA-LACTAMASE-PRODUCING ISOLATES IN MEDICAL INTENSIVE CARE UNITS VERSUS SURGICAL INTENSIVE CARE UNITS: RESULTS FROM SMART 2008–2009
Introduction: The Study for Monitoring Antimicrobial Resistance Trends (SMART) is a global longitudinal surveillance program that tracks antimicrobial susceptibility of aerobic gram-negative pathogens from intra-abdominal infections (IAI) to ertapenem, imipenem-cilastatin, amikacin, ampicillin-sulbactam, cefepime, cefotaxime, cefoxitin, ceftazidime, ceftriaxone, ciprofloxacin, levofloxacin, and piperacillin-tazobactam. Data from this program can help in development and updating of therapy guidelines as bacterial resistance to many drugs increases. This report compares incidence of extended-spectrum beta-lactamase (ESBL) producing isolates and the susceptibility of IAI pathogens recovered from surgical ICUs (SICU) to those of isolates from medical ICUs (MICU).
Methods: 120 hospitals in 35 countries collected 1,596 isolates representing 34 species from patients in SICU (713) or MICU (883) in 2008–2009. All isolates were sent to a central lab in the US for identification, confirmation of ESBL production, and susceptibility testing using CLSI methods. Only the 9 species with > 10 isolates recovered from both SICU and MICU were included in this analysis. Fisher's Exact Test was used to determine statistical significance.
Results: In 21 drug/species combinations a difference of > 10% susceptibility between MICU and SICU was seen: Proteus mirabilis had 7, Enterobacter aerogenes 5, Citrobacter freundii 4, Acinetobacter baumannii and Pseudomonas aeruginosa 2 each, and E. cloacae 1. SICU %S values were generally lower for A. baumannii, E. aerogenes, and E. cloacae, while MICU %S values were usually lower for C. freundii, P. mirabilis, and P. aeruginosa; however, in only 3 cases were the differences significant (P < .05), and only one of those, P. mirabilis vs. ciprofloxacin, had potential clinical significance. ESBL rates (%) in MICU/SICU for Escherichia coli, Klebsiella pneumoniae, K. oxytoca, and P. mirabilis were 24/28, 38/35, 12/9, and 21/4, respectively; however none of the differences in ESBL rates between MICU and SICU were significant (P > .05). Only ertapenem, imipenem, and amikacin maintained %S values > 85 in both MICU and SICU for all species except A. baumannii and P. aeruginosa, while amikacin did so for all species except A. baumannii and C. freundii. No other drug did so in more than 3 species.
Conclusions: Although there were some differences observed between MICU and SICU regarding drug susceptibilities and ESBL incidence, most were not statistically significant. Among the agents included in SMART, ertapenem, imipenem-cilastatin, and amikacin had the most in vitro activity against IAI pathogens in both MICU and SICU.
CEFTAROLINE ACTIVITY AGAINST CLINICAL ISOLATES OF STAPHYLOCOCCUS AUREUS, INCLUDING METHICILLIN-RESISTANT STRAINS (MRSA), FROM UNITED STATES (USA) HOSPITALS
Introduction: Ceftaroline (CPT) is a novel, parenteral, broad-spectrum cephalosporin exhibiting bactericidal activity against gram-positive organisms, including MRSA and multidrug-resistant Streptococcus pneumoniae (MDRSP), as well as common gram-negative pathogens. CPT is in late-stage clinical development for treatment of complicated skin and skin structure infections (cSSSI) and community-acquired bacterial pneumonia. S. aureus is the main cause of cSSSI. We assessed the activity of CPT tested against S. aureus from USA hospitals.
Methods: 6,626 unique clinical S. aureus strains, consecutively collected from 40 USA medical centers in 2008–2009, plus 10 molecularly characterized USA300-0114 strains (from cSSSI) were tested for susceptibility (S) against CPT and various comparator agents by CLSI broth microdilution methods.
Results: 53.4% of S. aureus were MRSA. CPT was very active against methicillin-S strains (MSSA) and MRSA with MIC90s of 0.25 and 1 μg/mL, respectively. All MRSA were inhibited at <2 μg/mL of CPT (see Table). CPT was eight- to 16-fold more potent than ceftriaxone (MIC50/90, 4/4 μg/mL) and cefepime (MIC50/90, 2/4 μg/mL) against MSSA. MRSA showed high resistance rates to erythromycin (92.5%), levofloxacin (71.3%) and clindamycin (34.7%), but remained 100.0% S to linezolid (MIC50/90, 2/2 μg/mL), vancomycin (MIC50/90, 1/1 μg/mL) and daptomycin (MIC50/90, 0.25/0.5 μg/mL). CPT was four- to eight-fold more active than linezolid or vancomycin and showed activity similar to daptomycin when tested against MRSA. All USA300-0114 strains were PVL positive, had SCCmec type IVa, and were highly CPT-S (MIC range, 0.5–1 μg/mL).
Conclusions: CPT was highly active against a large collection of MSSA and MRSA strains recently isolated in USA hospitals, including representative strains of the pandemic USA300 clone. CPT represents a very promising therapeutic option for treatment of cSSSI infections, including those caused by MRSA.
PROPRANOLOL SUPPRESSES APOPTOSIS AND PRODUCTION OF INFLAMMATORY CYTOKINES IN LPS-STRESSED HUMAN MACROPHAGE-LIKE THP-1 CELLS
Introduction: Propranolol (β-blocker) decreases the incidence of sepsis and improves mortality of critically ill patients. The aim of the present study is to determine the effects of propranolol on cell survival, cell activity, apoptosis and pro-inflammatory response in a human macrophage-like cell line (THP-1 cells) stressed with lipopolysaccharide (LPS).
Background: We showed before that high dose of LPS treatment induces apoptosis in differentiated THP-1 cells. In addition, propranolol attenuates the systemic inflammatory response in endotoxemic as well as in thermally injured rats by decreasing the pro-inflammatory and increasing the anti-inflammatory cytokines. However, there is little knowledge about the effect of propranolol on macrophages.
Methods: Differentiated THP-1 cells were stressed with LPS in the presence of (or without) propranolol. Cell viability was analyzed by MTT assay and Trypan blue staining, and caspase-3 activity was measured by the fluorescence of Z-DEVD-R110. JC-1 assay and terminal deoxynucleotidyl transferase-mediated nick end labeling staining was also used to confirm apoptosis. Tumor necrosis factor (TNF) and interleukin-1β (IL1-β) were measured to determine the effect of propranolol on pro-inflammatory cytokine expression.
Results: MTT assay and Trypan blue exclusion suggest that propranolol increases cell viability in LPS-treated THP-1 cells. Because caspase-3 plays a major role in apoptotic signaling, we measured the enzyme activity of caspase-3 by fluorescent substrate. We confirmed that the addition of propranolol-suppressed caspase-3 activation induced by high dose of LPS to almost control level in a dose dependent manner (range: 10–100μM; Figure). Propranolol also significantly decreased TNF and IL1-β in differentiated THP-1 cells.
Conclusion: Our results indicate that propranolol exerts anti-apoptotic effects in differentiated THP-1 cells, and it may reduce the expression of pro-inflammatory cytokines and apoptosis in endotoxemic human macrophages. Thus, application of propranolol to patients suffering sepsis after traumatic injuries may be beneficial by improving survival of macrophages meanwhile calming down inflammatory responses.
SifriZiad CMDMohrAlicia AMDHorngHelen SPharmDLaveryRobertMSLivingstonDavid HMD
UMDNJ-New Jersey Medical School
DO BLOOD STREAM INFECTIONS AFFECT OUTCOME IN TRAUMA PATIENTS?
Introduction: Blood Stream Infection (BSI) is a well known complication following trauma. However the timing of BSI, microbiology and its impact on outcome are not well described. The goal of this study was to examine the incidence, outcome, and predictors of BSI in adult patients admitted to a level-I urban Trauma Center.
Methods: Retrospective review of trauma patients who developed a BSI was performed from 1/07 to 12/08. Patients were excluded if they were discharged within 24 hours of admission. Demographic data, injury severity, transfusion requirements and microbiology were reviewed. Outcome included ICU and hospital length of stay (LOS), ventilator days and death. A student t-test, chi-square test or a Wilcoxon rank-sum test was used as appropriate.
Results: 2055 adult patients were admitted during a 48-month period. 66 patients (3%) sustained 105 episodes of BSI, 62 (59%) were GM (+), 38 (36%) were GM (-) and 5 were (5%) fungi. The most common pathogen was a Coagulase (-) S. aureus. No identifiable source occurred in 41/105 (39%) episode of BSI, in remaining 64 the source of infection was the lung (33%), central line (24%), abdomen (20%), soft tissue (14%), urine (6%), others (3%). Time of the first BSI was 16 days ± 21 (median 8 days) with 31(46%) of the initial BSI occurring the first week following injury. Patients with a BSI had a higher mean ISS (26 ± 11 vs. 15 ± 19, p = 0.001), higher mean # of units of PRBCs transfused (22 ± 27.4 vs. 6 ± 7.4, p = 0.001). There was no difference in age or gender between both groups. Patients with a BSI had a higher mortality (15% versus 4%, p < 0.0001), hospital LOS (50 ± 49 vs. 10 ± 14, p = 0.001), ICU LOS (24 ± 17 vs. 8 ± 8, p = 0.001) as well as vent days (22.1 ± 16.3 vs. 6.7 ± 7.4, p = 0.001). Logistic regression revealed that BSI was not an independent predictor of death. Multiple episodes of BSI were seen in 21 patients.
Conclusion: Incidence of BSI in trauma patients was 3%. BSI was more frequently seen in patients with higher ISS and higher transfusion requirements. Mean time to develop a BSI was 2 weeks, however half occurred in the first week following trauma. Patients who developed a BSI had higher mortality, longer vent days, ICU and hospital stay, but BSI was not an independent predictor of death. Gram-positive microorganisms were responsible for more than half of all BSI and Staphylococcus aureus was the most common pathogen. More than half of BSI had an identifiable source and in this group the 3 most common sources are lungs, central line and abdomen. Although BSI did not influence mortality we believe it's a marker for impaired immunity rather than a primary cause of mortality.
KraftRobertMDAl-MousawiAhmed AMDHerndonDavid NMDJuquanSongMDJeschkeMarc GMD, PhD
University of Texas Medical Branch, Galveston
QUANTITATIVE WOUND CULTURES: AN IMPORTANT MONITORING FACTOR IN CLINICAL PRACTICE?
Introduction: Detection and quantification of bacterial wound infections is crucial in surgical ICU patients. Recently however, the importance of quantitative evaluation of bacterial count has become controversial. Several clinical score systems require the evaluation of microbiological samples according to their bacterial load, although the value of this qualitative examination is sometimes underestimated on the clinical side. We hypothesized that bacterial count from wound tissue samples is highly relevant when monitoring for clinically significant complications including multi-organ failure, septic events, length of stay, and mortality.
Methods: Three-hundred and eleven pediatric burn patients with bacteria-positive tissue samples were evaluated retrospectively with regards to clinical course and outcome. Patient demographics, length of stay, infections, and number of burn operations were recorded. Patients were assigned to groups according to their highest bacterial count in the examined tissue samples [ > 10^2 (n = 7), > 10^3 (n = 16), > 10^4 (n = 34), > 10^5 (n = 311)]. Multi-organ failure (MOF) was assessed according to the DENVER2 score and the incidence of sepsis recorded based on clinical diagnosis and according to the ACCP consensus conference. Statistical analysis was performed by Student's t-test, ANOVA corrected with Bonferroni`s post-hoc test, Chi-square test and forward stepwise logistic regression, with statistical significance set at p < 0.05.
Results: All study groups were similar in age, gender, burn type and size. Length of stay increased significantly with the bacterial count (p < 0.05). Forward stepwise logistic regression revealed a statistically significant correlation between a bacterial count of >10^5 for sepsis and >10^3 for MOF (p < 0.05).
Conclusion: The results of our study demonstrate the importance of quantification of bacterial infections. We found that bacterial count is indeed an important indicator for clinical complications and patient outcome in the burn ICU setting.
AhmedNasimMDKuoYen-HongScM, MSKuoYen-LiangMDDavisJohn MMD, FACS
Jersey Shore University Medical Center
IMPACT OF TIMING OF TRACHEOSTOMY IN THE INCIDENCE OF PNEUMONIA FOLLOWING SEVERE HEAD INJURY
Background: Studies have shown that the early tracheostomy decreases ventilator and intensive care days. However, there are conflicting reports whether there is any impact of early tracheostomy in the incidence of pneumonia following severe head injury. The purpose of this study was to see any association of timing of tracheostomy in the incidence of pneumonia following severe head injury patients.
Methods: Patient information was retrieved from the National Trauma Data Bank Research Data Set v7.1. The inclusion criteria were: Blunt cerebral contusion injury at street and highway. Sever head injury was identified via the Abbreviated Injury Scale (AIS) codes with the AIS score >3, age between 18 and 89 years, and survived for 48 hours and underwent tracheostomy. Pneumonia during the course of treatment was the primary outcome. Wilcoxon rank-sum test and chi-square test was used to compare the continuous variables. Multiple logistic regression models were used to assess the association between the timing of the tracheostomy and pneumonia while controlling for potential confounding factors.
Results: Data from 656 TBI patients admitted during 2002–2006 were evaluated. The overall incidence rate of pneumonia was 23.6%. Patients who had developed pneumonia were similar to those who did not develop pneumonia in terms of age (mean[SD]: 39.7[17.2] vs. 39.3[17.2] years, P = 0.73), female gender (22.6% vs. 29.5%, P = 0.09), Injury Severity Score (ISS) (32.3[11.0] vs. 32.7[12.5], P = 0.94) and initial Glasgow Coma Scale Score (6.1[4.1] vs. 6.1[4.4], P = 0.67). However, patients who had developed pneumonia had a significantly delayed timing of tracheostomy (11.0[7.1] vs. 9.3[7.0] days, P = 0.0006). From a multivariate logistic regression model, late tracheostomy (>7 days) had a higher chance of developing pneumonia (odds ratio = 1.88, 95% confidence interval: [1.19, 2.95], P = 0.006).
Conclusion: Early tracheostomy reduces the incidence of pneumonia following severe head injury.
Pneumonia: 23.6% (155/656)
Pneumonia
Variable
No
Yes
P-value
Age
39.3 (17.2)
39.7 (17.2)
0.73
Female
29.5%
22.6%
0.09
Race
0.88
African
13.2%
11.6%
American
White
68.7%
69.7%
Others
18.2%
18.7%
ISS
32.7 (12.5)
32.3 (11.0)
0.94
Total GCS
6.1 (4.4)
6.1 (4.1)
0.67
Days to Tracheostomy
9.3 (7.0)
11.0 (7.1)
0.0006
Discharge alive
90.2%
92.9%
0.31
MonaghanSean FMDThakkarRajan KMDTranMai LBSHuangXinPhDCioffiWilliam GMD, FACSAyalaAlfredPhDHeffernanDaithi SMD
Rhode Island Hospital/Alpert Medical School of Brown University
CAN WE FIND BETTER MARKERS FOR IMMUNE AND PHYSIOLOGICAL DYSFUNCTION IN THE CRITICALLY ILL? THE CASE FOR PD-1
Background: Programmed Death 1 (PD-1) is an inhibitor protein receptor for the immune system and has been shown to be up-regulated in animal models of sepsis and after trauma and burn in humans. PD-1 may play a role in the immune dysfunction following these insults. However while prior studies have associated changes in PD-1 expression with altered immune cell function, it is not known if a correlation with clinical status exists.
Methods: Blood from daily laboratory draws was collected from both the surgical and trauma intensive care units. These samples were then processed by flow cytometry to look at various cell surface markers including CD3 and PD-1. In addition, clinical data was obtained such as presence of SIRS or sepsis, hospital mortality, and the calculated APACHE II score at the time of the blood draw. Chi square, t test, and one-way ANOVA statistics were used. The institutional review board approved this study.
Results: Thirty-two patients were included in the study resulting in 52 separate samples. Eleven samples were drawn as SIRS had resolved, 20 had SIRS, and 21 had sepsis at the time of their blood draw. Twenty-four patients had APACHE II > 20, 28 were under twenty. White blood cell count and percentage of CD3 + cells were not significantly different between patients with SIRS or sepsis or when comparing patients with APACHE II above or below 20, but tended to increase with worsening illness. The percentage of CD-3+PD-1+ cells was significantly higher in patients with an APACHE II > 20 (61.5% vs 41.4%, p = 0.001). A trend towards an increase was seen in PD-1 expression when comparing patients that ‘resolved SIRS’ vs ‘SIRS unresolved’ and ‘sepsis' (44.7% vs 50.3% vs 54.2%, p = 0.564). As expected, those who died had significantly higher APACE II (22.11 vs 16.39, p = 0.003). However, no significant difference in PD-1 expression relative to survival was seen.
Conclusion: These data indicate that the expression of PD-1 on T-cells can also be related to the extent of patient injury/physiological dysfunction. Thus, it is tempting to speculate that changes in the PD-1 expression alone or together with other markers could be a valuable diagnostic tool in delineating the development of not only immunological but also pathophysiological morbid status in the critically ill.
HeilbronOscarMDJimenezMaria FMDSanchezElioMDGilFabianMsCRiveraAuraMDNiñoNelsonMDAyalaJuanMDSanchezAlvaroMD, MsCPuyanaJuan CMD
PPPontificia Universidad Javeriana
TEMPORARY ABDOMINAL CLOSURE IN PATIENTS WITH SEVERE INTRAABDOMINAL INFECTION: A COHORT STUDY
Background: Definitive abdominal closure in the management of severe intra-abdominal infection remains controversial due to the paucity of data comparing several management strategies. The simplest approach continues to be the use of the Bogotá Bag, originally described for the management of catastrophic penetrating abdominal trauma. Nowadays a popular, but expensive alternative is the use of a commercially available negative pressure dressing with reported fascia approximation success up 88% in non-comparative studies. We designed hospital-made innovative, low cost abdominal vacuum system (Bogotá Vacuum) using generic sterile polyurethane foam for open abdomen management.
Objective: The aim of the present analysis is to compare the rates of delayed primary closure, fistula formation, and outcomes between patients who underwent temporary abdominal closure with Bogotá Bag (B. Bag) vs. our innovative Bogotá abdominal vacuum (B. Vacuum) system in patients with severe intra-abdominal infection. The primary end points were the rate of delayed primary fascial closure and enteral fistula rates. Secondary end points were time to delayed primary closure, ICU and hospital length of stay, and mortality.
Methods: We performed a retrospective cohort study of patients who underwent temporary abdominal closure with B. Bag or B. Vacuum pack system at an Acute Care Surgery unit from July 2007 to July 2008.
Results: 664 laparotomies were performed. Ten percent of them (63 consecutive patients) resulted in an open abdomen. B. Bag (26) and B. Vacuum (37) patients were equivalent in age, sex and severity of illness (APACHE II). Delayed primary closure for survivors (25.0% vs. 26.1%, p = 0.504), enteral fistula (3.4% vs. 13.5%, 0.387), ICU LOS (7.9 ± 6.8 vs. 10.3 ± 9.5 days, p = 0.426), LOS (23.5 ± 16.9 vs. 28.2 ± 21.5, p = 0.493) were not statistically different with the B. Bag or B. Vac system. The time to delayed primary closure (Log-rank test for equality of survivors function) was also not significant (p = 0.67)
Conclusions: Our rates of delayed primary abdominal closure are similar to a recent randomized controlled trial in a trauma population (1). We confirmed previous reports where the success for abdominal closure falls in peritonitis-only series. In this cohort, B. Bag and B. Vacuum techniques were not significantly different in the rates or the time for delayed primary closure. However, our results indicate a trend toward an increased fistula rate in the B. Vacuum compared with the B. Bag system. This study confirms the need for randomized controlled trials comparing temporary abdominal closure systems.
AckermanBruce HPharmDPhillipsKristenGuildayRobert EMDPattonMary LMDHaithLinwood RJrMD
Crozer-Chester Medical Center
IS THERE A RELATIONSHIP BETWEEN ELEVATED VANCOMYCIN TROUGH CONCENTRATIONS (VT) AND INCREASED EFFICACY OR TOXICITY?
Introduction: Recently observed increased isolation of methicillin-resistant Staphylococcus aureus with minimum inhibitory concentrations (MIC) > 2 mg/L has caused some to advocate increasing the VT to 10–15 mg/L or even higher for increased efficacy. Normally, only a VT is obtained however for 68 patients 116 vancomycin peak (VP) and VT were obtained. We evaluated serum concentration time data for toxicity and efficacy.
Methods: Using these VP and VT data, serum concentrations at 0.25, 1, 1.5, 2, 4, and 6 hours and midway through the dosing interval were estimated using 2-compartment pharmacokinetic data published by Rotschafer et al. in 1982. These estimates and the VP and VT concentration were computer fitted with less than a 5% change in each VP and VT and an r-value in excess of 0.988. Patient data were stratified by increments of 50 mL/min creatinine clearance from <50 to 250 mL/min and by VTs of <5, 5–10, and >10 mg/L.
Results: Resulting pharmacokinetic parameters were compared with the 1982 data. Time to negative sputum cultures, duration of therapy, time to normal white blood cell count, temperature and surface area burned did not differ among the stratified VTs (F < 1; p > 0.05). Chi-square analysis noted no risk of nephrotoxicity with rising VT (X2 = 5.555; p = 0.06). Pharmacodynamic parameters such as the percent time over MIC (MIC = 1.75) interquartile range (IQR) 89.82 to 93.34 predicted nearly 100% clinical response while the area under the serum concentration time curve divided by the MIC of 1.75 showed an IQR of 235.8 to 412.5, predicting no more than 25% clinical response in these 68 patients. Using time to normal temperature, white blood cell count, and heart rate, vancomycin therapy outcome was assessed and showed no difference using analysis of variance (F < 2 for all parameters; p > 0.05).
Conclusion: These data indicate that there is no clear prediction of vancomycin success or nephrotoxicity following analysis of the obtained vancomycin peak and trough concentrations and subsequent exhaustive pharmacodynamic analysis.
T½alpha
T½beta
Vdbeta
TBC
Rotschafer
0.5 ± 0.3
2.7–13.4
15.6–110
13.3–183
NSRBTC
0.2 ± 0.06
3.08–13.62
14.6–95.49
14.6–273
RomanowskiKathleen SMDKammAlaineAPNBaileyAlexBSRogginKevin KMDMatthewsJeffery BMD
University of Chicago
PHYSIOLOGIC LEUKOCYTOSIS IS NOT PHYSIOLOGIC FOLLOWING NON-TRAUMA SPLENECTOMY
Background: According to classical teaching, splenectomy is associated with a postoperative increase in platelet count (PC) and white blood cell count (WBC). The “physiologic” leukocytosis (above 15 × 109/μL) following splenectomy is thought to complicate interpretation of the WBC as an indicator of early postoperative infection. In trauma patients, a persistently elevated WBC (above 15 × 109/μL) or a ratio of PC/WBC < 20 has been proposed as markers of infection. This concept has not been validated outside of the trauma population. We hypothesize that there is no “physiologic” leukocytosis following non-trauma splenectomy and that the PC/WBC ratio is not applicable to the non-trauma patient.
Methods: With approval by the Institutional Review Board, we completed a retrospective chart review of the clinical course of all patients who underwent non-trauma splenectomy from January 2000 to January 2009. As most of the included patients underwent splenectomy associated with distal pancreatectomy, patients who underwent distal pancreatectomy alone served a control group. All relevant clinical information was collected. PC, WBC, and PC/WBC ratios were collected and calculated daily until post-operative day 20. Infectious complications were defined using the 2008 CDC guidelines. ANOVA analysis of the data for statistical significance (p < 0.05) was conducted with SPSS software.
Results: Chart review identified 183 eligible patients. Non-trauma, non-hematologic splenectomy was performed in 171 patients (splenectomy + /− other organ resection) while 12 patients underwent a spleen-preserving distal pancreatectomy. Forty-eight patients (28.4%) had a total of 70 surgical infections (23 intra-abdominal abscess, 15 bacteremia, 12 UTI, 11 wound infection-superficial, 7 wound infection-deep and 2 pneumonia). In the absence of infection, there was no difference in the postoperative WBC for patients under going splenectomy or splenic preservation. In patients with a documented infection, a leukocytosis was significant when observed in POD 3–7 (p < 0.05). Postoperative thrombocytosis (PC > 500) was evident in all patients who underwent splenectomy irregardless of their infection status. In patients who underwent spleen-preserving distal pancreatectomy, postoperative thrombocytosis developed only in patients with infection. PC/WBC ratio did not predict infection in non-trauma splenectomy patients on any post-operative day.
Conclusion: Postoperative elevation of WBC should raise suspicion of infection and not be attributed to a “physiologic” response to splenectomy. We found no evidence of non-infectious postoperative leukocytosis in non-trauma splenectomy patients. The post-splenectomy thrombocytotic response is not different between patients with or without infection, and the postoperative PC/WBC does not reliably predict infection in non-trauma splenectomy patients.
OHanleyPeterPhD, MD, MPHBeausoleilChristopherCCRPOHanleyKellyMD, MPH
Steve Stephens, Exoxemis Inc
E-101 SOLUTION, A NOVEL ANTISEPTIC INTENDED FOR DIRECT APPLICATION WITHIN A SURGICAL WOUND TO PREVENT SURIGICAL SITE INFECTION: BLINDED, CONTROLLED PHASE 1 SKIN IRRITATION STUDY IN HEALTHY VOLUNTEERS
Introduction: For many surgical procedures, surgical site infections (SSI) are much too common and are increasingly caused by highly virulent and multi-drug resistant microorganisms. An additional approach to SSI prevention is needed. E-101 Solution is a topical antimicrobial intended for application within a surgical wound to prevent SSI. It is novel both in terms of its mechanism of action and its intended use. The enzymatic activity of glucose oxidase produces a steady state of hydrogen peroxide that enables porcine myeloperoxidase (p-MPO) in E-101 Solution to catalyze the oxidation of chloride to hypochlorous acid and tyrosine to the tyrosyl radical and the disproportionation of hydrogen peroxide to singlet oxygen. These end-products are highly microbicidal against bacteria, viruses, fungi, yeasts, and prions in a concentration-dependent and time-dependent fashion. In animal models, E-101 Solution is considered safe, causing no deleterious effects on wound healing when administered directly into an experimental surgical wound.
Background: Prior to clinical testing of E-101 Solution on patients who are at high risk for SSI, it is necessary to ascertain its safety in healthy adult volunteers. Evaluation of the skin irritation potential of E-101 Solution is considered an important indicator of topical drug safety.
Methods: A well-accepted, FDA-recommended cumulative irritation Phase 1A study protocol was used to assess the safety of E-101 Solution during and after 21 consecutive days of topical exposure at dosage levels of 100 GU/mL and 300 GU/mL, compared to that of both 0.9% physiological saline (negative control) and 0.1% sodium lauryl sulfate (positive control). This study was subject-blinded and evaluator-blinded. A total of 30 subjects received all four treatments applied to both abraded and non-abraded target skin sites. Safety was assessed by visual inspection and scoring of skin irritation using a standardized irritation scoring scale, monitoring for adverse events, and laboratory tests.
Results: The table summarizes the mean cumulative irritation produced by the study drugs.
Skin irritation scores from abraded and non-abraded skin were lower (p < 0.05) in response to E-101 Solution exposure than those of the positive control. All notable E-101 Solution-related skin reactions were completely resolved within 48 hours after the last drug exposure. There were no clinically significant adverse patterns evident from conventional laboratory safety tests among the treated subjects and no adverse events.
Study Test Article
Mean Cumulative Irritation Score: Non-Abraded Skin
Mean Cumulative Irritation Score: Abraded Skin
Physiological saline (negative control)
13.90
20.63
E-101 Solution – 100 GU/mL
18.23
25.53
E-101 Solution – 300 GU/mL
20.10
32.33
Sodium lauryl sulfate (positive control)
38.77
47.80
Conclusions: The results of a conventional cumulative irritation Phase 1 study demonstrate E-101 Solution to be safe for application to human skin.
SongJuquanMDKraftRobertMDZhangXiaojunMDHerndonDavid N.MDBoehningDarrenPhDJeschkeMarc GMD, PhD
Shriners Hospitals for Children and the University of Texas Medical Branch, Galveston
THE REDUCTION OF HEPATIC ALBUMIN EXPRESSION IS ASSOCIATED WITH ER STRESS DEACTIVATED EEF2 AFTER BURN INJURY
Introduction: Severe burn induces hepatic damage and dysfunction and is associated with alterations of protein synthesis. eEF2k/eEF2 plays a key role in regulating elongation step of protein synthesis. The aim of the present study was to determine the molecular signalling mechanism that lead to an altered hepatic protein synthesis post-burn.
Methods: Sprague-Dawley rats received a full thickness burn of 60% of their total body surface area. Liver tissue was processed for Western blotting to determine eEF2k/eEF2 alterationn after burn injury in vivo. To mimic calcium alteration and subsequent ER stress after burn injury, Human hepatocellular liver carcinoma cell (HepG2) was treated with sarcoendoplasmic reticulum calcium ATPase (SERCA) inhibitor thapsigargin (TG). Cells were labeled with L-ring-13C6-Phenelylyne stable isotope and protein fractional synthetic rate (FSR) was measured by GC-MS. Protein signals were detected by SDS-PAGE and western blots, and intracellular calcium homeostasis was evaluated by calcium imaging in vitro.
Results: Burn injury caused an elevation of eEF2 kinase (eEF2K) activity by decreased its phosphorylation, leading to eukaryotic translation elongation factor 2 (eEF2) deactivated. The expression of hepatic derived albumin decreased 24hr postburn. Severe burn elevated cytosolic calcium concentrations by ER calcium depletion and caused subsequent ER stress. In an in vitro Hepg2 model, we found that calcium elevated in cytosol from ER and ER stress signals including p-IRE-1, Bip and p-JNK activated with 24 TG treatment, phosphor-eEF2k significantly decreased and phosphor-eEF2 correspond increased with TG treatment, protein FSR significantly decreased indicating the inhibition of hepatic protein synthesis.
Conclusion: Severe burn injury interrupts hepatic protein synthesis and is associated with eEF2k/ eEF2 signal pathway.
UramatsuMasashiMDMatsumotoTetsuyaMDTatedaKazuhiroMDMiyazakiShuichiMDHorinoTetsuyaMDTanabeMasaskiMDShibuyaKazutoshiMDSatoJunkoMDShinyaKusachiMDYamaguchiKeizoMD
The Third Department of Surgery, Toho University Ohashi Hospital
INVOLVEMENT OF ENDOTOXIN IN THE MORTALITY OF MICE WITH GUT-DERIVED SEPSIS DUE TO METHICILLIN RESISTANT STAPHYLOCOCCUS AUREUS
Introduction: Methicillin-resistant Staphylococcus aureus (MRSA) is an important pathogen causing a wide diversity of diseases ranging from benign skin infections to life-threatening diseases such as sepsis. However, there have been few reports of the pathophysiology and mechanisms of sepsis resulting from gut-derived origin of MRSA. Therefore, we established a murine model of gut-derived sepsis with MRSA and factors of MRSA sepsis that cause deterioration.
Method: We separated mice into three groups according to the antibiotic treatment as follows, 1) ampicillin (ABPC) 40 mg/kg; 2) ceftazidime (CAZ) 80 mg/kg; and 3) saline-treated control groups. Gut-derived sepsis was induced by intraperitoneal injection of cyclophosphamide after colonization of MRSA strain 334 in the intestine. The survival of mice was monitored and various organs were obtained during the infection for further analysis.
Results: After the induction of sepsis, significantly more CAZ-treated mice survived in comparison with ABPC-treated and control group of mice. MRSA were detected in the blood and liver among all groups. Endotoxin levels were significantly lower in CAZ-treated group compared to other groups. Inflammatory cytokine levels in the serum were lower in the CAZ-treated group compared to other groups. Fecal culture showed a lower level of colonization of E. coli in CAZ-treated group compared to other groups.
Conclusion: We found that CAZ-treatment ameliorates the infection and suppresses endotoxin level by the elimination of E. coli from the intestinal tract of mice. These results suggest endotoxin release from the resident E. coli in the intestine is involved in clinical deterioration resulting from gut-derived MRSA sepsis.
ANTIMICROBIAL ACTIVITY AND SPECTRUM OF THE NOVEL CEPHALOSPORIN CEFTAROLINE TESTED AGAINST BACTERIAL ISOLATES CAUSING SKIN AND SKIN STRUCTURE INFECTIONS IN USA MEDICAL CENTERS
Introduction: Ceftaroline (CPT) is a novel, parenteral, broad-spectrum cephalosporin exhibiting bactericidal activity against Gram-positive organisms, including methicillin-resistant S. aureus (MRSA), and multidrug-resistant S. pneumoniae (MDRSP) and common gram-negative pathogens, including non-ESBL-producing Enterobacteriaceae (ENT). CPT is in late-stage development for treatment of complicated skin and skin structure infections (cSSSI) and community-acquired bacterial pneumonia. We evaluated the activity of CPT and comparator agents tested against cSSSI pathogens.
Methods: Unique (1 per patient) clinically significant isolates were consecutively collected from cSSSI in 25 USA medical centers in 2008–2009. Each medical center contributed approximately 50 strains each year and the most frequently isolated organisms were analyzed. Susceptibility (S) testing was performed by reference CLSI broth microdilution method (M07-A8; M100-S20) against CPT and numerous antimicrobials currently available for cSSSI treatment.
% inhibited at <2 μg/ml for CPT. NA = not applicable. βHS = beta-haemolytic streptococci; EF = E. faecalis; KSP = Klebsiella spp., ESP = Enterobacter spp. PSA = P. aeruginosa
Results: More than 2,000 strains were tested and the 8 most common organisms are shown in the Table. The most frequently isolated organisms were MRSA (31.9%), methicillin-S S. aureus (MSSA; 27.8%) and E. coli (9.3%). 53.5% of S. aureus were MRSA. CPT was very active against MSSA and MRSA with highest MIC being 0.5 and 2 μg/mL, respectively. CPT (MIC90, 1 μg/mL; 100% inhibited at <2 μg/mL), linezolid (MIC90, 2 μg/mL; 100% S) and vancomycin (MIC90, 2 μg/mL; 100% S) were the most active compounds tested against MRSA. Levofloxacin (LEV; 44% S) and clindamycin (80% S) showed limited activity against MRSA. CPT was 8-fold more potent than ceftriaxone (CRO) against MSSA. Against Enterobacteriaceae, CPT and CRO showed similar spectrum with 80–90% and 79–92% S rates, respectively (see Table). LEV showed variable activity against ENT species; only 69% of E. coli was LEV-S. P. aeruginosa (PSA) showed high resistance (R) rates to most antimicrobials; the most active agents were piperacillin/tazobactam (88% S) and imipenem (IMI; 89% S). PSA and CRO-R ENT generally exhibited elevated CPT MIC values.
Conclusions: CPT was highly active against gram-positive and ENT pathogens recently isolated from cSSSI in USA medical centers, including MRSA. CPT spectrum against gram-positive pathogens was similar to those of LZD and vancomycin; while against gram-negative organisms CPT showed spectrum comparable to CRO. CPT appears to be a valuable agent for the treatment of organisms causing cSSSI.
EngstromStefanNorrisPatrick RDebelakKenneth AMernaughRaymond LValentiSarah DJenkinsJudith MDalyMichael BMayAddison KBoczkoErik M
Vanderbilt University
SEASONALITY OF PATHOGENS: A 7-YEAR STUDY OF CULTURE RESULTS FROM A SURGICAL ICU
Introduction: Certain pathogens are more prevalent at certain times of the year [1,3]. While resistance patterns are currently incorporated into antibiotic rotations, seasonality, or variation in pathogen incidence by time of year, is not. Furthermore, relationships between virulence, antibiotic resistance and seasonality are not well understood. We sought to characterize seasonal variation in a dataset of inpatient microbiology culture results derived from the day-to-day operation of a surgical ICU.
Methods: All final microbiology culture results from surgical intensive care (SICU) patients over a complete 7-year period were obtained (2002-01-01–2008-12-31). Cultures were identified by site, organism, and date of collection. Incidence of infectious organisms was stratified by month regardless of year.
Results:
Out of an estimated 12,800 total SICU patients, 1622 had one or more positive cultures with 141 different pathogens or pathogen classes represented.
Variations over the year from the overall mean behavior are present in many species. One interesting example is Acinetobacter baumannii (Figure) where the spring months present a significant deficit of positive cultures [2].
Our data reject the null hypothesis that that the spring months (Feb–May) are no different from the overall mean (binomial test, p < 0.05).
Grouping the data in chunks of two years allows the 12-month periodicity to be marginally detected by an autocorrelation (p < 0.05).
Certain pathogens were not present in sufficient numbers to make strong inferences about the seasonality, or lack thereof.
Conclusion: The seasonal variation observed may be consistent with the nature of Acinetobacter as a soil pathogen. Increased vigilance for certain pathogens, especially those that may be highly resistant to antibiotic therapy, may be warranted at certain times of the year.
References:
FreemanJ, AndersonD, SextonDJ. 2009. Emerging Evidence for Seasonality of Gram-Negative Bacterial Infections. Infect Control Hosp Epidemiol, 30,8:813–814.a-89
McDonaldLC, BanerjeeSN, JarvisWR. Natl Nosocomial Infections Survey. 1999. Seasonal variation of Acinetobacter infections: 1987–1996. Clin Infect Dis, 29,5:1133–1137.a-92RetailliauHF, HightowerAW, DixonRE, AllenJR. 1979. Acinetobacter calcoaceticus: a nosocomial pathogen with an unusual seasonal pattern. J Infect Dis., 139:371–375.a-90DriscollIan RMDDe CastroGerard PMDBochicchioGrant VMD, MPH, FACSZhuShijunPhDEdeikenSara MBochicchioKellyRN, MSIlahiObeid NMDJoshiManjariMDScaleaThomas MMD, FACS
Walter Reed Army Medical Center
ANTIBIOTICS PRIOR TO PEG PLACEMENT SIGNIFICANTLY REDUCES SURGICAL SITE INFECTIONS IN CRITICALLY INJURED TRAUMA PATIENTS
Introduction: To our knowledge, there is an absence of data evaluating the impact of pre-operative fever and leukocytosis as well as perioperative antibiotics (Abx) (prophylactic or scheduled) given prior to percutaneous endoscopic gastrostomy (PEG) on the incidence of surgical site infections in critically injured ICU patients.
Methods: Prospective data was collected on 215 trauma patients admitted to the Intensive care unit (ICU) of a major urban Level I trauma center who had undergone PEG placement in the ICU. Any use of prophylactic Abx for PEG placement and concurrently scheduled systemic Abx therapies were recorded. Maximum temperature and white blood cell count in the 24 hours prior to surgery were recorded. Fever was defined as temperature >101.4oF and leukocytosis was defined as a white blood cell count >11,000 K/μL. The diagnosis of a surgical site infection (PEG site) and resulting treatment were recorded. Fisher's exact tests were performed to assess the relationship of antibiotic use, fever, and leukocytosis to surgical site infections.
Results: 215 patients were enrolled in the study in which an equal number of patients received antibiotics (n = 107 or 50%) or no antibiotics (n = 108 or 50%). Of the patients receiving antibiotics, 27 patients (25%) received only prophylactic antibiotics prior to PEG placement, 73 patients (68%) received only scheduled systemic Abx (no additional), while 7 patients (7%) received prophylactic antibiotics in addition to their scheduled systemic antibiotics. The majority of the study population had a documented fever (n = 119 or 55%) or leukocytosis (n = 127 or 59%) in the 24 hours prior to PEG placement. The overall incidence of surgical site infections was 5.1% (n = 11). There was a four-fold decrease in the surgical site infection rate (1.9% vs. 8.3%) among patients who received antibiotics (prophylactic, scheduled systemic, or both) compared to those who did not. In addition, none of the patients who received prophylactic antibiotics (alone or in addition to scheduled systemic antibiotics) were diagnosed with a surgical site infection. The incidence of surgical site infections was not significantly increased in patients with pre-operative fever (p = 0.117) and/or leukocytosis (p = 0.762).
Conclusion: The incidence of surgical site infections is significantly decreased in trauma patients receiving Abx at the time of PEG placement. Pre-operative fever and/or leukocytosis is not a contraindication prior to PEG placement.
Positive cultures of A. baumannii per month in the SICU 2002–2008 (dark grey bars). As a comparison, the Mac-Donald et al. (1999) data set is shown in the lighter bars. The fitted curve is a 3-component Fourier description of the latter set.
PolitanoAmani DMDMammenTonyMDCostibileRaymond AMDLysiakJeffrey JPhDTurnerTerry TPhD
University of Virginia Department of Surgery
THE DEVELOPMENT OF RETROGRADE BACTERIAL EPIDIDYMITIS FOLLOWING VASECTOMY
Introduction: Epididymitis is a common urologic disease with possible severe consequences such as abscess formation, testicular infarction, recurrent infection, chronic pain, spread of infection to sexual partners, and infertility. Clinical epididymitis is often treated with antibiotics in the absence of culture-proven bacterial infection. Bacterial epididymitis most likely arises from retrograde inoculation of the epididymis via the vas deferens in the setting of urinary tract infection. Can retrograde infection of the epididymis occur in men who have undergone vasectomy? The objective of this study was to determine if infection of the epididymis can occur via retrograde progression from the lower urinary tract following vasectomy.
Methods: Twenty-one adult Sprague Dawley rats were divided into three groups: Bilateral sham vasectomy followed by left-sided sham inoculation (Group A); bilateral sham vasectomy followed by left-sided inoculation of Escherichia coli into the vas deferens (Group B); and bilateral vasectomy followed by left-sided inoculation of E. coli into the vas deferens (Group C). Three days after inoculation animals were sacrificed and the distal epididymidies contiguous with the proximal vas deferens were removed for routine histology. In other animals the epididymidies and proximal vas deferens were removed for protein isolation. Protein samples were assayed for nine cytokines including IL-1α, IL-1β, IL-2, IL-4, IL-6, IL-10, TNFα, INFγ, and GM-CSF via solution phase multiplex.
Results: Histologically, the proximal vas of vasectomized inoculated animals (Group C) was unchanged compared to sham-operated, sham-inoculated (Group A). Injection of E. coli into the vas deferens of sham-vasectomized animals (Group B) resulted in the presence of leukocyte infiltrates in the proximal vas. The levels of the assayed cytokines were unaffected by vasectomy alone or vasectomy plus E. coli (Group C); however, IL-1β, and IL-4 were significantly elevated in the E. coli inoculated patent system (Group B). Further, in no case did injection of E. coli induce an inflammatory response in the contralateral epididymis/proximal vas.
Conclusion: Bacterial epididymitis in the rat results in the upregulation of the proinflammatory cytokines IL-1α, IL-1β, and IL-4, and vasectomy limits the retrograde transmission of infection to the epididymis. The incidence of bacterial epididymitis in a vasectomized population has not been addressed. The current data suggests that bacterial epididimitis following vasectomy is unlikely, and treatment with antibiotics should be limited.
S-S is sham vasectomy with sham inoculum; S-E is sham vasectomy with injection of E. coli; V-E is vasectomy with E. coli injection. All values are in pg/μl ± standard error. Values labeled “a” do not differ from other values labeled “a” but do differ from values labeled “b”, p < 0.05.
WagnerPatrick LMDEachempatiSoumitra RMDHydoLynnMBAPieracciFrederic MMD, MPHBartholdiMarieUmunnaBen-Paul NShouJianMDBariePhilip SMD, MBA
NewYork-Presbyterian Hospital/Weill Cornell Medical Center
CONTEMPORARY PREDICTORS OF CONVERSION FROM LAPAROSCOPIC TO OPEN APPENDECTOMY
Introduction: Predictors of conversion to open appendectomy during laparoscopic appendectomy (LA) are poorly defined in the modern era in which most patients undergo CT scanning prior to surgery.
Methods: Retrospective review of 940 consecutive LAs for suspected appendicitis in a single institution (2000–2006). Patient demographics, history and physical exam findings, WBC and differential, CT findings, surgeon identity, and operative findings were assessed. Surgeon identity was assessed by comparing the ten most frequent attending surgeons, collectively accounting for 85% of cases, versus those who rarely performed LA. [Stats: chi square and student t tests, binary logistic regression analysis with conversion as the dependent variable, p < 0.05].
Results: 39 (4.1%) patients required conversion; the rate did not vary over the course of the study. Factors related to conversion on univariate analysis included advanced age, male gender, ASA > 2, longer duration of symptoms, abdominal rigidity, greater % neutrophils on WBC differential, extraluminal air on CT, surgeon identity, retrocecal appendix, gross necrosis or perforation, or turbid/purulent ascites. By multivariable analysis, older age, male gender, ASA > 2, attending surgeon's identity, and retrocecal appendix were independently and significantly associated with conversion (see table).
Conclusions: Despite increasing experience with laparoscopic appendectomy, ∼4% of patients continue to require conversion to an open procedure. Advanced age, male gender, ASA score >2, frequency with which the surgeon performs LA, and retrocecal location of the appendix are factors significantly and independently associated with conversion. These factors may help identify cases in which strong consideration should be given to proceeding directly with open appendectomy, potentially leading to reduced operative time and number of incisions.
KimPeter KMDArumugamDena G.BAChoStanley SMPHNosikStanislavMDBootheHughPhD
Jacobi Medical Center
ANTIBIOTIC USE AND SURGICAL MANAGEMENT IN 217 PATIENTS WITH MRSA SKIN AND SOFT TISSUE INFECTIONS
Introduction: Skin and soft tissue infections with methicillin-resistant Staphylococcus aureus (MRSA) have increased in frequency and severity in most hospitals resulting in greater need for admissions and surgical management.
Background: We hypothesized that a lack of awareness for the presence of this infection compounded by a prolonged period before cultures could identify this drug-resistant pathogen has led to inadequate therapy and increased length of stay.
Methods: We retrospectively reviewed the management of all 217 patients with skin and soft tissue infections that cultured MRSA in two inner-city hospitals from January 2008 to October 2009. Patients were assessed for age, gender, antibiotic use during inpatient hospitalization, time to appropriate antibiotic therapy, surgical management (incision and drainage; excisional debridement), and length of inpatient hospitalization.
Results: The age range for the patients was 1 month to 95 years (mean age = 39.6 years) with a male:female ratio of 1.8:1. Five patients infected with MRSA never received any antibiotics, and three of those patients underwent surgical drainage without antibiotic therapy. Of patients with MRSA culture-positive soft tissue infections who were treated with antibiotics, 73 (34%) were initially treated with an antibiotic that did not cover MRSA. Twelve patients never received appropriate antibiotic coverage during their hospitalization. For the 61 patients who were changed to an antibiotic that covered MRSA, the average time to appropriate therapy was 67.5 hours (95% C.I. 59.5–75.6). Of 169 patients treated with surgical management, 47 (28%) patients received delayed surgical therapy defined as greater than 24 hours after initial hospital presentation. The inpatient length of hospitalization was increased for those patients who received delayed surgical management of MRSA soft tissue infections (12.3 days; 95% CI 7.2–17.3) compared to patients who received timely surgical drainage or debridement (7.5 days; 95% CI 5.9–9.2). Of the 43 pediatric patients (age <18 yrs) who received antibiotic therapy, 14 (32%) initially received antibiotics that did not cover MRSA; of those 14 patients, 4 patients never received antibiotics that covered MRSA during their entire hospitalization. The mean time to appropriate therapy for the other 10 pediatric patients was 43.2 hours (95% CI 38.7–47.8). Of 32 pediatric patients treated surgically, 11 (32%) patients received surgical therapy in a delayed fashion.
Univariate analysis
Multivariable analysis
Variable
LA
Conv
p
Odds Ratio
95%CI
p
Age (yrs)
39 + 18
53 + 18
<0.01
1.03
1.001–1.05
0.04
Male gender
47%
64%
0.04
2.4
1.03–5.8
0.04
ASA > 2
5%
30%
<0.01
4.1
1.2–13.7
0.02
Days of symptoms
1.4 + 1.0
2.1 + 2.1
<0.01
Rigidity
1%
5%
0.02
% neutrophils
79 ± 11
83 ± 10
0.03
CT free air
2%
20%
<0.01
Surgeon Identity
0.01
6.8
2.7–16.9
<0.001
Retrocecal
27%
47%
0.02
3.4
1.5–7.8
0.004
Necrosis
13%
54%
<0.01
Perforation
8%
44%
<0.01
Purulent ascites
19%
44%
<0.01
Conclusion: Many patients with MRSA skin and soft tissue infections receive inappropriate antibiotic and delayed surgical therapies. Appropriate management of these infections, particularly in the pediatric population, may lead to decreased length of hospitalization. Prospective evaluation of a larger patient population will provide further data on this topic, and earlier diagnosis may lead to improved awareness and treatment of MRSA soft tissue infections.
EvansHeather LMD, MSWarnerKeir JBSBulgerEileen MMDShararSam RMDMaierRonald VMDCuschieriJosephMD
Harborview Medical Center, University of Washington
PREHOSPITAL INTUBATION FACTORS AND VENTILATOR-ASSOCIATED PNEUMONIA IN TRAUMA PATIENTS
Introduction: We previously reported ventilator-associated pneumonia (VAP) in emergently intubated trauma patients was associated with blunt injury, higher injury severity, and intubations >24 hours, but among these, only higher injury severity was independently predictive of VAP diagnosis. A subset of prehospital (PH) intubations subject to ongoing quality improvement data collection were re-examined to identify possible intubation factors associated with subsequent VAP.
Methods: Using an existing dataset of all consecutive adult trauma patients intubated prior to inpatient admission at a Level I trauma center between July 2007-July 2008 (excluding PH surgical airways, deaths and discharges within 48 hours), PH intubations with quality improvement data were identified. Intubation details were recorded including vital signs, medications, experience of intubating personnel, bag-valve mask (BVM) ventilation, and presence of material in the airway. The diagnosis of VAP was made by quantitative bronchoalveolar lavage (BAL) cultures (104 CFU), or by clinical assessment when BAL was impossible. Baseline data, injury characteristics and circumstances of intubation of patients with and without VAP were compared by univariate analysis.
Results: Detailed data were available for 114 PH intubated patients; 17 (15%) developed VAP on average 6 ± 0.7 days after admission. There was no difference in age, sex or comorbid diseases except diabetes which was more common in VAP (3 [17.7%] vs. 3 [3.1%], p = 0.01). There was a trend toward more blunt injury in VAP patients (14 [82.4%] vs. 59 [60.8%], p = 0.09) and higher injury severity as measured by both ISS (32.2 ± 2.9 vs. 22.6 ± 1.5, p = 0.01) and chest AIS (2.7 ± 0.4 vs. 1.4 ± 0.2, p = 0.01). No patients with stab wounds (25 [25.8%]) or pedestrians struck by vehicles (12 [12.4%]) developed VAP. GCS < 8 was the most common indication for intubation in both groups (8 [47.1% vs. 42 [43.8%], p = 0.71). Preintubation vital signs and level of consciousness did not differ, and medications and BVM ventilation were administered prior to intubation at a similar rate (Table 1). Senior medics performed more of the intubations with subsequent VAP, but this was not significant (15 [88%] vs. 71 [73.2%], p = 0.38). No patient with >1 recorded attempt prior to successful intubation developed VAP. Of those noted to have aspirated, 2 of 4 patients with emesis developed VAP, compared to only 1 of 13 with blood in the airway (p = 0.05).
Conclusion: Patient injury factors, rather than PH intubation circumstances, appear to be associated with development of VAP. Future prospective examinations of emergent intubation factors in trauma patients should focus on risk, timing, and character of aspiration.
VAP (n = 17)
No VAP (n = 97)
P value
Systolic BP (mm Hg)
113.8 ± 13.5
121.9 ± 3.7
0.43
Pulse (beats/minute)
95.9 ± 7.6
99.9 ± 2.5
0.55
Resp (per minute)
19.1 ± 2.1
18.5 ± 0.7
0.79
GCS
9.1 ± 1.2
10.2 ± 0.5
0.40
BVM
7 (41.2%)
42 (43.8%)
0.84
NMB
17 (100%)
95 (98.9%)
0.67
Sedation
14 (82.4%)
77 (80.2%)
0.27
(VAP = ventilator associated pneumonia, BP = blood pressure, GCS = Glasgow Coma Score, BVM = bag valve mask ventilation, NMB = neuromuscular blockade)
EfronPhilip A.MDNacionalesDina C.MDKelly-ScumpiaKindraPhDCuencaAlex G.MDDelanoMatthewMD, PhDAngDarwin N.MD, PhD, MPHMoldawerLyle L.PhD
University of Florida
BLOOD TRANSFUSION INDUCES LATE CHANGES IN SPLEEN LEUKOCYTES
Introduction: Blood transfusion is associated with increased morbidity and mortality in the critically ill. The variables contributing to this pathophysiology are unclear, including when increased susceptibility to infection occurs. In addition, the roles of blood storage duration and allogenicity have not been adequately defined. We hypothesize that innate and adaptive immunity are altered in the recipient almost one week after blood transfusion.
Methods: Female C57Bl/6 mice underwent a 100 μL (8% blood volume) tail vein hemorrhage followed by a 200 μL retro-orbital injection of either 1 day-old (DO) syngeneic (SYN) C57Bl/6 packed red blood cells (PRBC), 1 DO allogeneic (ALL) Balb/c PRBC, 21 DO SYN PRBC, 21 DO ALL PRBC, or PBS (n = 3–4/group). Whole blood was placed in CPD and Adsol™ preservative solutions, centrifuged and stored at 4°C to create PRBC. Spleens were harvested 6 days post transfusion. T helper cells/CD4 + , T effector cells/CD8 + , B cells/CD19 + and neutrophils/CD11bLy6G + were studied using flow cytometry. Data is presented as mean ± SEM. Statistics were performed by one-way ANOVA.
Results: Transfusion of 1 DO PRBCs induced significant increases in T effector cells (ALL 21.5 ± 1.4, SYN 23.4 ± 1.0, PBS 16.8 ± 0.1; p = 0.03) and B cells (ALL 39.9 ± 3.8, SYN 27.0 ± 1.5, PBS 27.7 ± 0.04; p = 0.03), with only ALL PRBCs altering the latter. This is consistent with increased activation of adaptive immunity. Additionally, there was a significant decrease in neutrophils following transfusion of any PRBC genotype (ALL 2.4 ± 0.58, SYN 4 ± 0.18, PBS 8.7 ± 0.9; p = 0.001). Transfusion of 21 DO blood had both similar and differing effects as 1 DO PRBCs on splenic leukocyte populations. B cells expanded while the neutrophil population contracted (ALL 2.4 ± 0.03, SYN 3.2 ± 0.03, PBS 4.2 ± 0.06; p = 0.04) with the transfusion of any blood genotype. However, only 21 DO ALL PRBCs decreased the T helper cell population (ALL 10.9 ± 0.6, SYN 15.9 ± 2.2, PBS 17.0 ± 0.9; p = 0.05). Although 21 DO PRBC induces multiple changes, these alterations are mostly consistent with the suppression of both adaptive and innate immunity. There were no significant changes in total splenic WBC counts, implying percent differences reflected absolute changes.
Conclusion: Transfusion of PRBC induces late alterations in the recipients' splenic leukocyte populations. Transfusion of young blood is associated with immune activation, while receiving PRBC that has undergone prolonged storage appears to induce a setting of immune suppression. Allogenicity appears to amplify certain affects, including splenic B cell expansion. Interestingly, any PRBC transfusion is associated with a loss of splenic neutrophils. In conclusion, PRBC transfusion generates WBC changes that may explain why recipients of these products are more susceptible to infection. We believe these alterations are consistent with immune suppression and activation demonstrated by other inflammatory insults such as sepsis.
SealJohnMDAlverdyJohnMDBabrowskiTrissaMDFinkDavidMDRomanowskiKathleenMDZaborinaOlgaPhDAnGaryMD
University of Chicago
MECHANISTIC COMPUTATIONAL REPRESENTATION OF PATHOGEN RESPONSE TO MICROENVIRONMENT CHANGES DURING HOST STRESS
Introduction: The pathogenesis of microbe-mediated diseases involves complex interactions between the host and pathogen. Many microbes are able to sense stress-related changes in the host microenvironment and respond with virulome expression and phenotype shifts. Understanding the coordination, expression and population characteristics of these sense and response mechanisms is a formidable challenge that exceeds the traditional methods of constructing a pathogenesis paradigm. We propose that agent-based modeling (ABM), an object-oriented computational modeling method, is well-suited to dynamically represent knowledge of pathogen and host interactions in an in silico experimental platform.
Methods: An ABM for sense and response mechanisms in Pseudonomas aeruginosa was constructed using NetLogo. Sense and response mechanisms for iron and phosphate depletion, host systemic inflammatory mediators and opioid stress response, and changes in the mucous environment were included. Agents representing individual cells interact in a virtual host milieu to model the response to changes in the mucous microenvironment during host stress. Rules governing agent interactions were extrapolated from published experiments and results from our collaborating lab group. Pathogen virulence mechanisms include mucinases, PA-1 lectin (gut permeability), and toxins directed against host epithelial cells and endogenous flora. Changes in the availability and distribution of nutrients and host signals are modifiable to account for variability in host stress response. Representations of microbial constituents within the mucous layer include endogenous flora and opportunistic pathogens.
Results: Host stress was modeled with simulated combinations of ischemia/inflammation and nutrient depletion. Gene sequences for bacterial virulence were represented as both individual modules and as bundled, co-regulatory groups simulating hierarchical packets of virulence expression. Simulation results demonstrated that heterogenous populations of pathogens with variable sense and response capabilities produced the most robust population dynamics. Furthermore, different initial distributions of virulence factors led to different stable and meta-stable outcomes corresponding to varied health and disease states, suggesting that the baseline “virulence potential” of an endogenous bacterial population has significant implications regarding the development and trajectory of microbial-influenced disease.
Conclusion: The challenge of understanding and representing complex interactions in the mucous microenvironment during host stress can be mitigated with dynamic and modifiable instantiation of mechanistic relationships within an ABM. This ABM of the pathogen sense and response mechanisms in response to host stress integrates the knowledge derived from multiple experimental environments into an overall dynamic representation, and allows the performance of in silico “function” knock-outs to parse the contribution of different components of the overall pathogen population response to host stress.
De CastroGerard PMDHsuJuneMPHBochicchioGrant VMD, MPH, FACSBochicchioKellyRN, MSScaleaThomas MMD, FACS
University of Maryland School of Medicine
EVALUATION OF THE APACHE II, SOFA, SIRS, & ISS SCORING SYSTEMS IN PREDICTING OUTCOME IN CRITICALLY ILL TRAUMA PATIENTS
Introduction: Several scoring systems including APACHE II, the Sequential Organ Failure Assessment, the Systemic Inflammatory Response Syndrome, and the Injury Severity Score have been developed to grade the severity of illness in critically ill trauma patients with the goal of predicting clinical outcomes in these patients. These systems have been studied independently, or in comparison with another system, in their ability to predict clinical outcome. However, a study comparing all 4 systems simultaneously has not yet been reported. Our objective was to prospectively evaluate the ability of these 4 scoring systems in predicting 5 primary outcomes (mortality, nosocomial infection, ICU days, hospital days, and ventilator days) and to determine which scoring system is best at predicting a specific outcome in the first week.
Methods: Prospective data were analyzed on trauma patients admitted to the ICU of the primary adult trauma center in the state of Maryland over a 2-year period. APACHE II, SOFA, and SIRS scores were calculated for each patient on admission and then daily for 1 week. An ISS score was calculated at time of discharge. Each scoring system was evaluated as an independent predictor of the mentioned outcomes on the day of admission up to day 7. Additionally, each of the 5 outcomes were analyzed to determine which scoring system was a better predictor for the specific outcome.
Results: The prospective study cohort consisted of 816 patients. Table 1 displays the scoring systems that significantly (p < 0.05) predicted a particular outcome on a specific day (Odds Ratio, p-value). On the day of admission, SIRS and ISS scores significantly predicted infection, ICU days, ventilator days, and hospital days. APACHE II, SOFA, and ISS scores were better predictors of mortality than the SIRS score at admission. Between days 2 – 6, no scoring system was significantly better than another in predicting clinical outcomes. On day 7, APACHE II, SOFA, and SIRS scores significantly predicted infection, ventilator days, hospital days, and ICU days while APACHE II and SOFA scores significantly predicted mortality.
Conclusion: In general, all scoring systems were better at predicting clinical outcomes at the time of admission and on day 7. On admission, SIRS and ISS scores are best used to predict infection, ventilator days, hospital days, and ICU days, while the APACHE II, SOFA, and ISS scoring systems are better at predicting mortality. With regards to infection, SIRS score appears to be superior, particularly on days 1, 6, and 7. The use of these scoring systems between days 2 to 5 appears to demonstrate little utility in predicting outcome in critically injured trauma patients. Further research is warranted for better prediction models during this period.
Admission
Day 2
Day 3
Day 4
Day 5
Day 6
Day 7
Mortality
APACHE II (1.07, 0.002) SOFA (1.21, 0.000) ISS (1.03, 0.000)
APACHE II (1.1, 0.047)
APACHE II (1.15, 0.001) SOFA (1.41, 0.000)
Infection
ISS (1.03, 0.000) SIRS (1.3, 0.000)
SIRS (1.287, 0.014)
SOFA (1.25, 0.000) APACHE II (1.07, 0.006) SIRS (1.45, 0.000)
Days Vented
SIRS (1.2, 0.005) ISS (0.23, 0.000)
APACHE II (0.35, 0.001) SOFA(0.42, 0.051)
SOFA(0.818, 0.01)
APACHE II (0.49, 0.000) SOFA (0.92, 0.001)SIRS (1.84, 0.002)
Hospital Days
SIRS (1.76, 0.000) ISS (0.23, 0.000)
APACHE II (0.434, 0.000)
SIRS (1.27, 0.044)
APACHE II (0.525, 0.000) SOFA (0.629, 0.045)SIRS (2.37, 0.000)
ICU Days
SIRS (1.07, 0.005) ISS (0.2, 0.000)
APACHE II (-0.28, 0.003)
SOFA(0.489, 0.04) SIRS (-1.12, 0.03)
SIRS(1.15, 0.028)
APACHE II (0.37, 0.002) SOFA (0.896, 0.000)SIRS (1.76, 0.001)
COMBINATION THERAPY WITH CASPOFUNGIN AND VORICONAZOLE IN INVASIVE ASPERGILLOSIS IN SURGICAL PATIENTS
Background: Invasive aspergillosis is still associated with a high mortality. Thus far little data on combination therapy using voriconazole and caspofungin in surgical patients are available.
Patient and methods: Between January 2002 and December 2008, 21 surgical patients received combination therapy of caspofungin and voriconazole for treatment of proven invasive aspergillosis. Immunosuppressive status was found in nineteen patients due to solid organ transplantation (n = 16) and malignancies (n = 3).
Results: In 16 cases the site of infection was the lung (14 were lung transplant recipients), four patients had Aspergillus pleural empyema and one patient developed an Aspergillus liver abscess following open abdominal treatment in the course of streptococcal gangrene of the abdominal wall complicating cesarean section. Caspofungin was given for induction between 4 and 32 days, voriconazole was started intravenously and switched to oral and given up to 166 days. In four patients with Aspergillus pleural emyema following pneumonectomy for previously diagnosed pulmonary aspergillosis, surgical debridement was performed and a thoracostoma closed during a second surgical procedure in two of them. These two patients received two courses of antifungal therapy. Two lung recipients had recurrent pulmonary aspergillosis and received additional courses of treatment. Infection was cleared clinically and microbiolocically in 17 patients, in four patients aspergillosis was ongoing. Nine patients died during follow up (invasive penicillinosis 1, sepsis 1, tumor recurrence 1, PTLD 1, pneumonia 1, suicide 1 and recurrent aspergillosis 3).
Conclusion: Caspofungin/voriconazole combination therapy was found highly active in the treatment of invasive aspergillosis in this pilot study. A prospective trial is urgently needed to establish guidelines for the use of these new agents.
MOTOR VEHICLE BLUNT SPINAL CORD TRAUMA AND POSTTRAUMATIC INFECTION: WHO IS AT RISK?
Introduction: Spinal cord trauma patients suffer a variety of concomitant injuries that can significantly contribute to the development of various complications. Post-injury infectious complications substantially increase poor outcomes in these patients and increase hospital resource utilization. The objective of this study was to identify risk factors for infectious complications after motor vehicle blunt spinal cord injury [SCI] and to evaluate the impact of associated injuries in the development of posttraumatic infection [PTI].
Methods: Persons age 18 years and older suffering blunt trauma injuries were selected from the Nationwide Inpatient Sample (2003–2007) utilizing ICD9-CM diagnosis codes. The study population was categorized according to the level of SCI: Cervical, thoracic, lumbar and sacral; cases with combinations were excluded from analysis. Associated injuries were also identified: Cerebral, thoracic, small bowel, colon, splenic, kidney, ureteral/bladder, long bone and pelvic fractures. PTI complications included: Pneumonia (PNA), urinary tract infections (UTI), sepsis, and surgical site infections (SSI). Data were analyzed with univariate (chi-square) and multivariable logistic regression analyses.
Predictors of PTI
Odds Ratio 95% CI
Females
1.14 (1.01–1.28)
Hispanics
1.46 (1.21–1.74)
Level of SCI:
Cervical
2.70 (2.17–3.36)
Thoracic
1.94 (1.54–2.44)
Associated injuries:
Pelvic fractures
1.58 (1.29–1.93)
Thoracic
1.45 (1.27–1.66)
Cranial
1.38 (1.14–1.66)
Results: 10,783 patients were identified: 6,186 (57.4%) in the cervical group, 3,173 (29.4%) thoracic, 1,167 (10.8%) lumbar, and 257 (2.4%) sacral. Males predominated by a ratio of 3.5:1 (8,410 vs. 2,373). Whites accounted for 72.5% of study population; Blacks (12.9%), and Hispanics (9.1%). 2,373 (22.0%) cases were complicated by PTI. The greatest rate of infection was found in the cervical group (24.7%), followed by thoracic (21.8%), sacral (11.5%), and lumbar (10.6%). Adjusting for age, gender, race, level of SCI, and associated injuries, a logistic regression model was created with PTI as the outcome; females and Hispanics were more likely to develop PTI (see Table). Compared to patients with trauma of the lumbar spine, patients with injuries in cervical and thoracic areas were significantly more likely to experience PTI. Among associated injuries, the greatest likelihood of developing PTI was found in patients with pelvic fractures, thoracic, and cerebral injuries.
Conclusion: Infection rates after traumatic spinal injuries were significantly associated with gender, race, level of spinal cord injury, and associated injuries. Patients at greatest risk for developing posttraumatic infectious complications after spinal trauma were females and Hispanics. Injuries most associated with the development of infection after blunt spinal cord injury were cervical injury and associated pelvic fractures. Further analysis of high risk patients suffering blunt spinal cord injury may lead to preventive strategies to reduce infectious complications.
Table *References: males, whites, patients with injuries in lumbar spine and those without associated injuries. PTI-posttraumatic infection. SCI-spinal cord injury.
KananZiadMDPeytonJamesMSGardnerSarahBSCheadleWilliam GMD
University of Lousville
MACROPHAGE GENETIC REPROGRAMMING DURING CHRONIC PERITONITIS IS AUGMENTED BY LPS PRETREATMENT
Introduction: In response to chronic peritonitis from Klebsiella pneumoniae, we have observed peritoneal macrophage reprogramming that is dependent on intraperitoneal (IP) concentration of bacteria over time. Such tolerance may lead to resolution of the early innate response, and may be responsible for incomplete bacterial clearance and a chronic inflammatory state. The hypothesis is that LPS pre-treatment of chronic peritonitis will induce early macrophage tolerance at the transcriptional level.
Methods: 24 hours after IP LPS (0.01 mg/g) or saline, C57BL/6 mice were given 103 colony-forming units of K. pneumoniae IP. Gentamicin was then given BID. Peritoneal exudate cells were obtained through peritoneal lavage and RNA was isolated (n = 3) at 4, 24, and 48 hours following infection. SA Bioscience RT2 Profiler PCR array mouse Toll-like receptor signaling pathway (PAMM_018A) data were analyzed by Ingenuity Pathway Inc. analysis (IPA). Student's t-tests were used to calculate fold change and IPA for pathway significance.
Results: Of the 84 genes studied, 26 were significantly dysregulated (fold change >2.0 and p-value <0.05) in the saline-pretreated group at 4, 24, and 48 hours. All of the dysregulated genes were up regulated. In the LPS pretreated group, 35 genes were significantly up regulated (fold change >2.0 and p-value <0.05). Of the 35 significantly regulated genes in LPS pretreated mice, 13 (Cd86, Clec4e, Fos, Ikbkb, Il1a, Nfkb1, Nfkbia, Nr2c2, Pglyrp1, Rel, Rela, Ripk2, and Tlr2) were not increased in the saline group. This left 22 genes dysregulated in common. At 4 hours, of these 22 genes 6, (Chuck, Hmgb1, Hspd1, Irak2, Ly96, and Tlr4) were further 2-fold increased in the LPS pretreatment compared with saline pretreatment. Only Irak2 is 2-fold increased at 24 hours. By 48 hours no LPS effect was seen. The 22 common regulated genes are: Btk, Cd80, Chuck, Hmgb1, Hras1, Hrb, Hspd1, Irak2, Jun, Ly96, Map3k7, Peli, Eif2ak2, Ticam, Tirap, Tlr4, Tlr6, Tlr7, Tlr9, Tnfrsf1a, Traff6, and Ube2v1. When applying IPA analysis to the above data, 6 main canonical pathways were constantly dysregulated, and in the same significance order, in both the saline and LPS group at 4, 24, and 48 hours. These are: Toll-like receptor and NF-KB signaling, hepatic cholestasis, interleukin-6 and LPS mediated MAPK signaling pathways, and pattern recognition receptors of bacteria pathway.
Conclusion: Peritonitis increased PEC gene expression associated with sepsis and a pro-inflammatory response, which was further augmented by LPS pretreatment over 24 hours only. Prior exposure to LPS did not induce PEC gene tolerance to subsequent infection with Klebsiella. Up-regulated pathways were common to the early innate response, and macrophage reprogramming occurs at the genetic level. Lack of bacterial clearance in this model is due to an inadequate innate response that resolves despite incomplete clearance of intraperitoneal bacteria.
EngstromStefanNorrisPatrick RDebelakKenneth AMernaughRaymond LValentiSarah DJenkinsJudith MDalyMichael BMayAddison KBoczkoErik M
Vanderbilt University
MAKING SOUND USE OF SCARCE DATA: EXAMINING THE IMPACT OF REPEAT POSITIVE CULTURES IN A DATASET OF MICROBIOLOGY FINDINGS
Introduction: Multiple culture reports from a patient during a hospital stay can inform us of new infections. However, it is also possible that the same infection is being monitored and repeated results could bias an analysis that has other aims than immediate patient care. Simple techniques such as dropping repeat positives are in common use but discards precious data. We present a method to weight successive positive cultures in the same patient without the drawback of complete information loss. The weighting approach is compared to two alternatives: An all-inclusive analysis and the more conservative approach of discarding data.
Methods: All final microbiology culture results from surgical intensive care patients in five isolation room beds over a 53 month period were collected and stratified by bed occupied. We considered two common cases: (1) repeated, duplicate findings within N days of one another and (2) a non-specific finding followed by a specific one. The following scheme was used to reduce the impact of repeat cultures, while retaining evidence of their existence:
Repeated findings of a particular organism, spanning D days, in which there was no time gap between findings longer than N days, were ordered chronologically.
For each sequence we assign a weight of 1 to the first observation. Each subsequent observation is weighted by a monotone function fw(d) that satisfies fw(0) = 0 and fw(N) = 1, where d is the number of days to the preceding observation. For the purpose of this study we used N = 7 days, and a nonlinear fw(d) = (Exp(d2/N2)−1)/(Exp(1)−1).
We then renormalized the weights so that they sum to (D + N)/N. If N = 7 days and D = 25 days then we allow a total of 4.57 observations within this period.
Results: Out of 904 unique patients, 397 had one or more positive cultures.
When the data are processed without weighting we obtain a total of 2,473 entries in a contingency table that tabulates number of observations for the beds in our sample. The overall null hypothesis that the incidence of positive cultures does not vary by room is firmly thrown out (p < 10−30) by this all-inclusive scheme.
In contrast, the sample weighted to not allow more than a sum of more than one unit per week for any given species produces a total weight of 1407 for otherwise equivalent conditions. This approach more marginally rejected (p < 0.01) the null hypothesis.
A conservative method is to consider only “new” observations where a pathogen is discarded if it is less than 7 days since it was last observed, resulting in 1,159 entries for the contingency table. This approach does not reject the null hypothesis (p = 0.053).
Conclusion: Whether or not repeat cultures are taken into account can lead to different interpretations of historical microbiology culture data. We have described a straightforward method to model the degree to which a subsequent positive culture represents an independent result, without discarding data. Our method leads to increased utility of clinical culture datasets for research and quality-improvement efforts.
HarbrechtBrian GMDSmithJason WMDFranklinGlen AMDRichardsonJ DavidMD
University of Louisville
ACUTE APPENDICITIS- NOT JUST FOR THE YOUNG
Introduction: Appendectomy for acute appendicitis is the most common general surgical emergency procedure. Acute appendicitis is generally considered a disease of youth. The incidence of AA is thought to be highest in the second and third decade of life. As the proportion of older patients increases, the number of elderly patients with AA is likely to increase. The effect of an aging population on the demographics and utilization of resources related to acute appendicitis is unknown. We evaluated the statewide experience with acute appendicitis in elderly patients to assess the effect of this common disease on health care resources.
Methods: A state database was queried for all patients with acute appendicitis by ICD-9-CM codes (540–541) for 2007. Subjects admitted to rehabilitation hospitals, patients transferred to a second facility, patients with inflammatory bowel disease, or those undergoing incidental appendectomy were excluded. Procedures were defined as open appendectomy, laparoscopic appendectomy or complicated open procedures (colectomy, abcess drain). Data are presented as the mean ± SD.
Results: Young patients ( < 29 years) comprised 45% of subjects with appendicitis which was the same proportion as middle-aged patients (30–64 years) (Table). Total hospital charges increased significantly with increasing age of patients with appendicitis and the youngest patients accounted for only 37.6% of all charges (Table). Elderly patients ( > 65 years) comprised 9.3% of all appendicitis patients but accounted for 14.2% of health care charges related to acute appendicitis. While the proportion of laparoscopic appendectomy was high in all age groups, length of stay and percentage of complicated procedures significantly increased with age (Table).
Conclusion: Acute appendicitis is no longer strictly a disease of the young. Older patients with acute appendicitis represent a substantial proportion of cases and a disproportionate share of health care resources related to acute appendicitis. Acute appendicitis as a cause of abdominal pain or abdominal symptoms should be considered as a potential etiology for patients of all age groups.
KuoYen-HongScMMSAhmedNasimMDKuoYen-LiangMDDavisJohn MMD
Jersey Shore University Medical Center
ALCOHOL ABUSE INCREASED POSTOPERATIVE INFECTION AND LENGTH OF HOSPITAL STAY ON ESOPHAGEAL CANCER RESECTIONS
Background: Excessive alcohol consumption has a negative effect on the immune system. However, its impact on the surgical outcomes following esophageal/esophageal-gastric resection for cancer is unknown. The purpose of this study was to assess the association between the chronic alcohol abuse and the surgical outcomes following esophageal cancer surgery by using a population-based discharge database.
Methods: A retrospective cohort study was conducted to include adult patients (>18 years) who were diagnosed with malignancy of esophagus and underwent esophagectomy or gastrectomy during 2002–2006 by using data from the US Nationwide Inpatient Sample. Postoperative infections and length of hospital stay were the outcomes of interest. Multiple logistic regression models were used to assess the association between the chronic alcohol abuses with postoperative infection while controlling for confounding factors. Kaplan-Meier curves were constructed and compared by using the log-rank test.
Results: A total of 2,247 patients had esophageal cancer resections. The overall postoperative infection rate was 6.1%. The patients with co-morbid alcohol abuse (5.1%) were younger (mean [standard deviation]: 60.6[9.7] vs. 63.4[11.0] years, P = 0.006), less likely to be female (10.7% vs. 18.7%, P = 0.03), and had a similar mortality rate (11.6% vs. 7.5%, P = 0.11) as compared to the patients without the history of alcohol abuse. However, the postoperative infection rate was significantly higher (12.5% vs. 5.8%, P = 0.004). From a multivariate logistic regression model, history of alcohol abuse was significantly associated with increased postoperative infection (odds ratio: 1.95, 95% confidence interval: [1.03, 3.66], P = 0.04), when controlling for age, gender and diabetes. In addition, alcoholic patients had a significantly longer length of hospital stay (median: 16 vs. 12 days, P = 0.02).
Conclusion: This study demonstrated that patients with co-morbid alcohol abuse had a higher chance of postoperative infection and a much longer length of hospital stay following surgery for esophageal cancer.
ClarkeCallisia NMDMiaoYunMD, PhDRistagnoRossMDAhmadSyedMDSolomkinJosephMD
University of Cincinnati
ROLE OF RESISTANT GRAM-POSITIVE BACTERIA IN TREATMENT FAILURE FOR PERCUTANEOUS DRAINAGE OF POST-OPERATIVE COMPLICATED INTRA-ABDOMINAL INFECTION (CIAI)
Background: Complex post-operative infections, defined as cIAI lacking a straightforward surgical alternative, are commonly managed with percutaneous drainage. Absent physical tissue manipulation and debridement, it is not known whether standard rules of antimicrobial therapy, in particular, early presence of antimicrobial therapy covering all pathogens subsequently identified on culture, pertains. We therefore chose to review patients with these complex intra- abdominal infections treated at our institution to explore the effect of adequate empiric antibiotic therapy on outcomes.
Methods: A retrospective review of patients with intra-abdominal infection and severe complicating illnesses treated from January 2007 through February 2008 was conducted. Treatment failure was defined as conversion to open debridement, persistent positive infection greater than 5 days from initial procedure, or death from overwhelming sepsis.
Results: 94 patients met inclusion criteria. Demographics showed a male to female ratio of 1.5:1 with an average age of 50 years. Infections occurring after bowel resection (16), pancreatic resection (12), liver resection (11), acute pancreatitis (11) and bowel perforations (7) accounted for over 60% of all cases.
Gram-positives were most commonly isolated from initial drainage procedures (56%), followed by gram-negatives (41%) and Candida (3%). Antibiotic therapy for gram-negative organisms was active against all encountered. However, in 2 of 5 patients with methicillin-resistant Staphylococcus aureus (MRSA) initial therapy did not include vancomycin. For 8 patients with vancomycin-resistant Enterococcus (VRE), none were initially treated.
Twenty-five patients required repeated drainage more than 5 days after the initial procedure. VRE and MRSA were the most commonly isolated organisms in patients requiring repeat drainage procedures (53%). Six patients (6.4%) died despite maximal medical management.
Conclusion: Appropriate percutaneous drainage of fluid collections is a viable method of source control in patients with complex post-operative intra-abdominal infections. Our data support the notion that antimicrobial therapy remains an important adjunct for optimal medical management in these patients. VRE and MRSA are major pathogens associated with treatment failure.
HardinMark OMDRitchieJohn DMDFreemyerJosiah DWhiteChristopher EMD
U.S. Army Institute of Surgical Research, San Antonio
MUCORMYCOSIS IN A BURN ICU
Introduction: Invasive fungal infection remains one of the most morbid problems facing the burned patient.
Background: Our center had previously reported a 10-year experience with fungal burn wound infections from 1979–1989. The overall mortality rate from all fungal infections was 75%. In this study, mucormycosis occurred in 9.0 per 1000 burn admissions. Previous case reports of mucormycosis suggest an extremely high mortality with this condition. The impact of modern antifungal agents and burn wound care on the incidence and mortality of mucormycosis is unclear.
Methods: From January 2003 to November 2009, a case series of patients admitted to our adult burn center who were diagnosed with mucormycosis during their admission was assembled.
Results: During the period of interest, 2453 patients were admitted to the burn center. Of these patients, 15 were diagnosed with mucormycosis (6.1 per 1000 admissions). The median age of these patients was 23 (IQR 22–25), and the median total burn surface area (TBSA) was 56 (IQR 43–72). Of the 15, 12 were military wounds from Operations Enduring Freedom and Iraqi Freedom and the remaining 3 were civilian patients. These patients were diagnosed by physical examination of wounds with wound biopsy and culture of concerning wounds. The extremities were the most frequent site of involvement (66% of cases), followed by head and neck (33%) and trunk (27%). One patient with an open abdomen developed mucormycosis of the small bowel and colon; however, no patients had evidence of disseminated mucormycosis. These wounds were treated with antifungal therapy in 93%, local debridement alone in 67%, and debridement with amputation in 27%. One patient was transitioned to comfort care based on the diagnosis of mucormycosis and died. Overall, the mortality in patients with mucormycosis was 73% with 45% of the deaths attributed to the fungal infection. There did not appear to be an association between treatment modality and overall or fungal-related mortality. TBSA appears associated with mortality with survivors having a low TBSA (0% to 36%) compared to non-survivors (50% to 93%).
Conclusion: The incidence of mucormycosis has decreased at our institution over the last 20 years (6.1 vs. 9.0 per 1000 burn admissions). However, the overall mortality is unchanged (73% vs. 75%). Mortality directly attributable to mucormycosis is significantly less than total mortality with many patients dying from other causes (e.g., gram-negative sepsis). Aggressive surgical debridement to include amputation was not associated with improved outcomes.
LitvinAndrey A.MD, PhD
Gomel Regional Clinical Hospital, Gomel State Medical University, Belarus
USE OF DATA MINING FOR PREDICTION OF INFECTED PANCREATIC NECROSIS
Introduction: Infected pancreatic necrosis is associated with high morbidity and mortality and is mandatory for surgical or radiosurgical intervention.
Background: The aim of this study was to construct and validate a data mining (DM) algorithm to predict infected pancreatic necrosis (IPN).
Methods: All patients who presented with severe acute pancreatitis from January 1996 to December 2007 were reviewed. Presentation data on admission and at 48 hours were collected. Acute Physiology and Chronic Health Evaluation (APACHE) II and Glasgow severity (GS) score were calculated. A Data Mining (Artificial Neural Networks (ANN) and Support Vector Machine SVM)) algorithm was created and trained to predict development of IPN and mortality from AP; 25% of the data set was withheld from training and was used to evaluate the accuracy of the DM. Accuracy of the DM in predicting infected pancreatic necrosis was compared with APACHE II and GS scores.
Results: A total of 1460 patients with acute pancreatitis were identified of whom 320 (21.9%) fulfilled the clinical and radiological criteria for severe pancreatitis and 91 patients died (6.2%). Median APACHE II score at 48 hours was 6 (range, 0 to 23). DM (ANN and SVM) was more accurate than APACHE II or GS scoring systems at predicting infected pancreatic necrosis (P < .05 and P < .01, respectively).
Conclusion: A DM was able to predict development of infected necrotizing pancreatitis with considerable accuracy and outperformed other clinical risk scoring systems. Further studies are required to assess its utility in aiding management decisions in patients with severe acute pancreatitis.
Lomas-NeiraJoannePhDThakkarRajanMDMonaghanSeanMDCarterNicholasBAAyalaAlfredPhDHeffernanDaithiMD
Rhode Island Hospital, Alpert School of Medicine at Brown University
IS ANGIOPOIETIN-2 ELEVATED IN TRAUMA PATIENTS WITH EXTRAPULMONARY ALI/ARDS?
Introduction: Acute lung injury (ALI), and the more severe acute respiratory distress syndrome (ARDS), are respiratory conditions associated with significant ICU mortality. Current published statistics for the U.S. report 74,000 deaths in 190,000 cases of ALI/ARDS and it is anticipated that as the U.S. faces the inevitability of an aging population, the annual incidence will rise. The underlying pathology of ALI/ARDS is differentiated into direct and indirect, based on precipitating factors. Direct (pneumonia, aspiration and lung trauma) accounts for 57% of total cases, while indirect lung injury, including extrapulmonary sepsis and multisystem trauma, represents 43%. However, compared with direct ALI/ARDS, the pathophysiology of indirect is much less well understood, possibly due to the involvement of multiple systemic factors. Endothelial cell (EC) dysfunction/loss of barrier function is a major component in the pathogenesis of ALI/ARDS based on the increased lung mircovascular hyperpermeability, pulmonary edema and impaired lung function observed in patients that develop ALI/ARDS. Angiopoietin-2 (Ang-2) is an EC specific growth factor believed to play a role in angiogenesis by promoting vessel destabilization, inflammation and pulmonary leakage through its interaction with the EC specific receptor tyrosine kinase, Tie2. While we have recently shown in our shock/trauma mouse model that Ang-2 may play a role in the development of extrapulmonary ALI (Ang-2 levels increase) via its mediation of neutrophil/EC interactions, it is not known to what extent trauma patients with ALI/ARDS show such a change in Ang-2 expression. To begin to address this question, plasma Ang-2 was measured in a random sampling of surgical and trauma ICU patients (n = 16) and healthy human volunteers (n = 3). We hypothesized that Ang-2 would be significantly elevated in patients with ALI/ARDS.
Methods: Ang-2 was measured in plasma from de-identified trauma and surgical ICU patients using a commercially available human Ang-2 ELISA kit in an IRB-approved study. Corresponding de-identified patient data for ALI/ARDS (PaO2:FIO2), extra vs. intrapulmonary infection source, sepsis/SIRS and mortality was collected and compared with patient's plasma Ang-2 level.
Results: Our findings support the hypothesis that plasma Ang-2 is elevated in trauma patients with ALI/ARDS in a fashion similar to that seen in rodents. Additionally, those patients with extrapulmonary associated SIRS/sepsis appear to have higher levels of plasma Ang-2 when compared to those with intrapulmonary/pneumonia (5887 ± 571 pg/mL vs. 3931 ± 691 pg/mL, p < 0.05). In our small sample group, however, elevated plasma Ang-2 could not be correlated with mortality. These findings support not only the further investigation into the dynamics of plasma Ang-2 levels in the traumatized patient, but also the value of the mechanistic studies of Ang-2 we are carrying out in a relevant model of shock/sepsis induced ALI in mice.
KimPeter K.MDUmHeesun C.PharmDAhmadSalMDCoyleChristinaMDTepermanSheldonMDBootheHughPhD, PharmD
Jacobi Medical Center
INTRACOLONIC VANCOMYCIN FOR SEVERE CLOSTRIDIUM DIFFICILE COLITIS
Introduction: Severe colitis from infections with Clostridium difficile that fails to respond to standard therapy with oral vancomycin and intravenous metronidazole require surgical exploration and subtotal colectomy. Historical controls report a mortality rate >50% for patients who require colectomy and may be associated with an increase in incidence of cases with C. difficile that produce high toxin levels.
Background: We initiated a protocol in our inner-city hospital where inpatients with severe C. difficile colitis infection were treated with intracolonic vancomycin (500 mg in 500 mL normal saline via rectal tube every 6 hours) and aggressive monitoring for potential surgical resection. We hypothesized that adjunct therapy with intracolonic vancomycin would decrease mortality and the need for surgical colonic resection.
Methods: We retrospectively reviewed all 47 patients with C. difficile-positive colitis treated with intracolonic vancomycin from January 2007 through October 2009 in a large inner-city hospital. We analyzed the cohort for age, gender, comorbidities, history of recent hospitalizations or nursing home stay, previous history of infectious colitis, previous antibiotic use, APACHE II severity score, resolution of colitis, incidence of surgery, and mortality.
Results: The average age of patients was 65 years (range 22 to 97) and 62% were female. Ninety-two percent of patients had significant comorbidities, and more than half were nursing home residents. Seventy percent had received antibiotics previously and 74% had been hospitalized within the past year. Twenty-three percent of patients were recurrent episodes. All patients had high APACHE II severity scores (Mean 24, Range 14–47). After treatment with adjunct intracolonic vancomycin, thirty-three of 47 (70%) patients showed complete resolution, and 14 of 47 (30%) demonstrated incomplete resolution of their colitis. Ten of 47 patients (21%) treated with intracolonic vancomycin expired. Nine of 47 patients (19%) who received intracolonic vancomycin required surgery. Seven patients (78%) who underwent surgery survived and two patients (22%) expired. Of 38 patients treated with intracolonic vancomycin without surgery, eight expired (21%) and 30 survived (79%). There were no complications attributable to intracolonic vancomycin.
Conclusion: Intracolonic vancomycin should be considered an adjunct method to treat fulminant C. difficile colitis that may decrease the need for colectomy and improve mortality when used in addition to standard therapy with oral vancomycin and intravenous metronidazole. Some patients may progress to needing subtotal colectomy, and careful monitoring by a surgical service is incumbent. Further studies are necessary to identify patients who would benefit from earlier combination therapy or surgery.
ReigartCynthia LBSNAckermanBruce HPharmDStair-BuchmanMeghanBSNHerderDianeLPNAdamsPamelaMT, ASCPYoungChristineMT, ASCP, CIC, MBAGuildayRobert EMDPattonMary LMDHaithLinwood RJr.MDRavrebyWilliam DMD
Crozer-Chester Medical Center
MULTIDISCIPLINARY PERFORMANCE IMPROVEMENT (PI) TASK FORCE PROJECT MARKEDLY REDUCED AND ELIMINATED RESISTANT ACINETOBACTER BAUMANII/HAEMOLYTICUS (AB)
Introduction: Over a 15-year period, our burn treatment center noted a pattern of AB resistance suspicious for a specific resistance clone and its' variant. AB resistance was addressed via development of a multidisciplinary team to investigate and propose solutions to this problem.
Methods: An outside hospital epidemiologist consultant assessed infection control practices at an on-site visit of the burn treatment center and the intensive care units. The following recommendations were made: 1) establish AB control goals, 2) collect data on antibiotic use and AB isolation, 3) continue surveillance cultures, 4) redesign of the burn treatment center, and 5) redesign the hydrotherapy area. Immediate changes included: 1) contact isolation procedures according to the Centers for Disease Control, 2) cohorting AB patients, 3) individualization of all patient care equipment, 4) evaluation of cleaning solutions in use, and 5) if necessary total unit terminal cleaning.
Results: Comparison of multi-year cycles demonstrated a random process of “high” and “low” AB isolation (See Figure). The low yield of environmental and health care workers hand cultures did not correlate with AB recovery from patient cultures. Routine surveillance cultures of patient care areas sought out a potential nidus of AB. Surveillance cultures recovered multi resistant organisms with rare isolation of AB. Modification of behaviors and revision of cleaning practices improved environmental culture results.
Conclusion: Initiation of stringent hand washing and adherence to infection control guidelines eliminated both clones of AB. Chlorhexidine for handwashing is impaired by organic contaminates and may explain the low level persistence of AB in properly washed hands. Our successful approach and progressive control of the organism did not require closing of the burn unit. Although we never found the “one” source, we did identify and eliminate the sites that revealed positive cultures and modified likely processes that promoted contamination. Ultimately, we were successful in eliminating our resistant AB clones.
SchillerDarylPharmDRezaiFariborzMDMeadowsMichael CMDGrayEdward HDOFlessKristinMDChamberlainRonald SMD, MPAYodicePaul CMD
Saint Barnabas Medical Center
OUTCOMES ASSOCIATED WITH PROLONGED INFUSIONS OF PIPERACILLIN-TAZOBACTAM IN CRITICALLY ILL PATIENTS
Introduction: Piperacillin-tazobactam (P-T) exhibits time-dependent bactericidal activity but due to a short half-life, a prolonged infusion duration may be more efficient at achieving active concentrations.
Hypothesis: Critically ill patients who receive a prolonged infusion of P-T may have better outcomes compared to standard infusions.
Methods: Standard dosing of P-T in a medical/surgical intensive care unit was changed to a 4-hour infusion. Data from 3 months prior and 4 months after the intervention was collected and analyzed.
Results: Patients receiving P-T prolonged infusion, compared to standard infusion, demonstrated a trend towards a shorter ICU length of stay (7.92 vs 5.51 days, p = 0.13). Patients were then matched by APACHE II scores, separated into high (>17) and low (<17) scores, and then analyzed according to standard or prolonged infusions. Only critically ill patients with high APACHE II scores demonstrated a significantly shorter LOS with a prolonged, compared to standard, infusion (7.29 vs 3.38 days, p = 0.006). Additionally, there was a 1 gm per patient per day savings, which was associated with nearly $12,000 saved per year.
Conclusions: More consistent serum levels may allow more rapid recovery from an infection leading to a shorter ICU length of stay, earlier discharge and significant cost savings.
AckermanBruce HPharmDAdamsPamelaMT, ASCPYoungChristineMT, ASCP, MBAReigartCynthia LBSNGuildayRobert EMDPattonMary LMDHaithLinwood RJrMDRavrebyWilliam DMD
Crozer-Chester Medical Center
ASSESSMENT OF THE TREATMENT OF ACINETOBACTER BAUMANNII FOLLOWING THE OUTBREAK OF A MULTI-RESISTANT CLONE AND A VARIANT CLONE IN A BURN TREATMENT CENTER
Introduction:Acinetobacter baumannii is a non-fermentive Gram-negative cocciobacillus with multiple resistance genes isolated with increasing frequency in intensive care units.
Methods: Electronic microbiology records were inquired for thermal injury patients with isolation of A. baumannii (AB) from sputum, blood, or wound cultures. Patients were designated as “colonized”(COL) if a single AB culture was obtained and considered “infected” (INF) if AB isolates were obtained from 2 or more sites or at 2 or more time periods. INF patients were then evaluated for whether or not they had been treated with antibiotics for which the isolate was sensitive.
Results: Isolates (N = 8729) from INF (N = 308) demonstrated susceptibility to ciprofloxacin, cefepime, imipenem cilastatin (IC), ampicillin-sulbactam (AS), colistin, and tigecycline. Chi-square analysis as “eradicated,” “persisting,” and “failure” for these six antimicrobial agents did not differ (X2 = 5.2873; p > 0.05). T-test comparison of the 45 COL versus 308 INF demonstrated no difference in age, height, weight, or initial laboratory tests. Day to first A. baumannii culture also did not differ between COL and INF. As expected, total body surface area burn (T = 4.28256; p < 0.05) and length of stay (T = 4.0475; p < 0.05) were greater in INF. All 45 COL survived; however only 207 INF survived (76.9%). T-test analysis of INF survival status noted that non-survivors were older (T = 2.1207; P = 0.03), had larger burns (T = 3.1157; p < 0.05), had lower serum albumin levels (T = 2.0214; p = 0.04), and had positive cultures sooner (T = 2.9108; p < 0.05). For INF, inhalation injury did not predict increased mortality (X2 = 0.5535; p > > 0.05). Stratification by mg/kg dose and renal function of IC and AS demonstrated no difference in eradication, persistence, or failure for doses <40 mg/kg and <250 mg/kg and for doses >40 mg/kg and >250 mg/kg for IC (X2 = 2.47; P > 0.5) and AS (X2 = 4.39; P > 0.05), respectively. Difference in time to eradication and a few other parameters remain to be assessed.
Conclusion: These initial data indicate that the chosen antibiotic and dose had no impact on AB eradication. For these multi-resistant AB INF patients nearly 25% succumbed to infection. Early isolation of AB was associated with increased risk of mortality, as was larger burns, older age, and lower albumin. AB in thermal injury patients was a persisting opportunistic INF with low virulence and high antimicrobial agent resistance for which patients “died with,“ rather than “died of” AB.
CLOSTRIDIUM DIFFICILE INFECTION MAY REQUIRE SURGICAL MANAGEMENT IN CHILDREN
Introduction:Clostridium difficile (C. difficile) is the main cause of nosocomial and antibiotic-associated diarrhea in adults and represents a major public health issue. C. difficile infection in children, initially considered clinically unimportant, has recently been seen to have an increased incidence in hospitalized children. Both healthy children without significant risk factors and children with complex medical problems have been reported to suffer significant morbidity from C. difficile infections. We sought to characterize the patient population requiring surgical intervention for C. difficile infection at a tertiary-care pediatric hospital.
Methods: Children (<18y) admitted to a single tertiary care pediatric hospital, between 1/1/2003 and 12/31/2008 were eligible for this study. Case status was determined by the presence of an International Classification of Diseases, Ninth Revision, Clinical Modification code for C. difficile infection (code 008.45). Only cases with billing for a C. difficile toxin assay and an initial dose of antimicrobial therapy were included. This project was reviewed and approved for exemption by the University of Pittsburgh Institutional Review Board.
Results: We identified 767 patients with C. difficile infection over a 5 year period out of 77,455 hospital admissions (0.99%). Of these, 7 patients (0.91%) required surgical therapy for management of their C. difficile colitis. The average age of these patients was 10.3 years (range 5 months to 16 years) with an average length of stay of 23 days. Two of these patients had undergone solid organ transplantation (1 liver and 1 isolated small bowel transplant). The only death was due to liver failure in the patient with a prior liver transplant. Four of the 7 patients received subtotal colectomies, 2 required ileocecectomies, and the small bowel transplant patient required a small bowel resection. Prior to undergoing subtotal colectomies, 2 of the patients developed abdominal compartment syndrome.
Conclusion:C. difficile infection is a recognized problem in the pediatric population; however, fulminant C. difficile colitis requiring surgical intervention appears to be rare. Specific risk factors are unclear, although solid organ transplant recipients due seem to be disproportionally represented. Unlike our observation in adult patients where the presence of hypervirulent strains did not correlate with severity (Muto et al. JID 2009 and Zuckerbraun unpublished observation), future studies would be required in the pediatric population. Diarrhea in pediatric patients should prompt evaluation for C. difficile and initiation of therapy as indicated.
CathroHelen PMDSifriCosti DMDKeithDouglasMDSawyerRobert GMDPruettTimothy LMDBraymanKennethMD, PhDBonattiHugo JRMD
University of Virginia
CLINICAL IMPLICATIONS OF VIRUS-ASSOCIATED NEPHROPATHY AFTER RENAL TRANSPLANTATION
Background: The development of powerful immunosuppression has resulted in a decline of rejection rates of kidney allografts; however, the incidence and prevalence of opportunistic infections has risen accordingly. Polyoma virus-associated nephropathy (PVAN) has become a common complication; cytomegalovirus (CMV) and adenovirus also cause graft nephritis.
Patients and Methods: Sixteen cases of biopsy-proven graft nephritis from a single center were retrospectively reviewed (diagnosed 2003–2008). Standard immunosuppression consisted of anti-thymocyte globulin induction followed by tacrolimus, mycophenolate-mofetil and a steroid taper. Renal biopsies were obtained after graft dysfunction and were evaluated for rejection according to BANFF criteria. Viral immunohistochemical stains were performed.
Results: A single case of adenovirus nephritis was diagnosed after living-donor re-transplantation (Tx). Two cadaveric graft recipients (one re-Tx) developed CMV-associated nephritis. PVAN was diagnosed in 13 cases (all were first Tx, seven living and six cadaveric grafts; two with simoultaneous pancreatic grafts). Graft nephritis developed at a median 16.4 mn (range 2.5 - 47.1) post-Tx; 71% of patients had undergone prior treatment for rejection. Immunosuppression was tapered; the CMV nephritides were treated with ganciclovir, but both grafts were lost. The adenovirus nephritis resolved after reduction of immunosuppression; however, long-term graft function is poor. PVAN was treated with low-dose cidofovir in 11 cases and leflunemide in two cases, and nine patients received immunoglobulins. In nine cases therapy resulted in improvement of graft function, five patients lost their graft (one after PVAN relapse).
Conclusion: Renal allograft nephritis is most commonly caused by polyoma virus. Although previous studies have suggested that 75% of polyoma virus infections occur during the first year post-transplantation, 77% of PVAN occurred after the first year at our institution. Long-term monitoring for viral nephritides should therefore continue after the first year post-tranplantation.
RosenbergerLaura HMDHranjecTjasaMD, MSMetzgerRosemarieMD, MPHSwensonBrian RMD, MSSawyerRobert GMD
University of Virginia
COHORTING AND SUPERISOLATION IN A SINGLE INTENSIVE CARE UNIT IN AN EFFORT TO REDUCE PATIENT-TO-PATIENT TRANSMISSION
Introduction: Cohorting patients in dedicated hospital wards or wings during infectious outbreaks has been shown to reduce the transmission of infection, yet this may not be feasible in a hospital frequently over capacity, especially in the Intensive Care Units (ICU).
Hypothesis: Cohorting isolation patients in one geographic location in a single ICU and using enhanced isolation procedures for infected patients (“superisolation”) can prevent the further spread of highly resistant multi-drug resistant bacterial organisms (MDRO).
Materials and methods: At one moment in time in a twelve-bed Surgical Trauma Burn Intensive Care Unit (STBICU), six patients had active infections with carbapenem-resistant, non-clonal gram-negative MDRO, including Klebsiella pneumoniae (KPC), Citrobacter freundii, Stenotrophomonas maltophilia, Aeromonas hydrophilia, Proteus mirabilis, Pseudomonas aeruginosa, and Providencia rettgeri. All six were colonized with VRE. Three were admitted to the ICU following complications from liver transplantation, one with 55% total body surface area burns, one after the development of multiple enterocutaneous fistulae, and one following a shotgun wound to the chest & abdomen. Initially the six patients were interspersed throughout the unit, many of whom had a nurse also providing care for a non-isolation patient. Under threat of unit closure and after all standard isolation procedures were enacted, the patients with multi-drug resistant bacteria were cohorted into the front six beds of the unit. The main front entrance was closed and all traffic was redirected through the back entrance of the unit. Nursing staff was assigned to either two isolation or two non-isolation patients. Per Semmelweis, rounds were conducted so as to end at the patients' rooms cohorted to the front of the unit with the most highly-resistant bacterial infections. Procedures and diagnostics were performed at the bedside (without transporting out of the unit) unless absolutely necessary.
Results: Two months after these interventions, all six patients have been discharged from the ICU (three alive and three dead). No new cases of infection with any of the previously isolated pathogens (based on species and antibiogram) or VRE have occurred.
Conclusion: Cohorting patients to one area and altering work routines to minimize contact with patients with MDRO (essentially designating a high-risk zone) may be beneficial in stopping patient to patient spread of highly resistant bacteria without the need for a dedicated isolation unit.
AhmedNasimMDKuoYen-HongScM, MSKuoYen-LiangMDDavisJohn MMD
Jersey Shore University
IMPACT OF TRAUMA CENTER LEVEL IN THE INCIDENCE OF PNEUMONIA FOLLOWING SEVERE HEAD INJURY
Background: The purpose of this study was to see any association of state designation level of trauma center in the incidence of pneumonia following severe head injury patients.
Methods: Patient information was retrieved from the National Trauma Data Bank Research Data Set v7.1. The inclusion criteria were: Blunt cerebral contusion injuried at street and highway. Severe head injury was identified via the Abbreviated Injury Scale (AIS) codes with the AIS score >3, age between 18 and 89 years, and survived for 48 hours and underwent tracheostomy at the Level I or II trauma centers. Pneumonia during the course of treatment was the primary outcome. Wilcoxon rank-sum test and chi-square test was used to compare the continuous variables. Multiple logistic regression models were used to assess the association between the trauma center level and pneumonia while controlling for potential confounding factors.
State Designation Level
Variable
I (n = 375, 69%)
II (n = 167, 31%)
P-value
Age
39.3 (17.1)
40.5 (17.1)
0.39
Female
30.7%
22.2%
0.04
Race
0.11
African
16.5%
10.8%
American
White
67.2%
67.7%
Others
15.3%
21.6%
ISS
32.9 (12.3)
32.4 (12.9)
0.34
Total GCS
6.1 (4.5)
6.3 (4.2)
0.25
Days to Tracheostomy
9.8 (7.4)
9.0 (6.9)
0.30
Discharge alive
89.1%
92.2%
0.26
Pneumonia
24.3%
22.2%
0.59
Pneumonia: 23.6% (128/542).
Results: Data from 542 TBI patients admitted during 2002–2006 were evaluated. 69% of these patients were admitted to a level I trauma center. Patients who were treated at the Level I were similar to those who were treated at the Level II trauma center in terms of age (mean [SD]: 39.3 [17.1] vs. 40.5 [17.1] years, P = 0.39), race distribution (P = 0.11), Injury Severity Score (ISS) (32.9[12.3] vs. 32.4[12.9], P = 0.34) and initial Glasgow Coma Scale (6.1[4.5] vs. 6.3[4.2], P = 0.25). However, Level I centers had treated more female patients (30.7% vs. 22.2%, P = 0.04). When outcomes were compared, there were no significant differences were between the Level I and the Level II trauma centers in terms of mortality (10.9% vs. 7.8%, P = 0.26) and incidence of pneumonia (24.3% vs. 22.2%, P = 0.59) respectively. From a mulitple logistic regression model, patients who were treated at Level I center had a similar chance of developing pneumonia (odds ratio = 1.21, 95% confidence interval: [0.41, 3.56], P = 0.73), however, male gender and delayed tracheostomy (>7 days) significantly increased that chance.
Conclusion: Our study found that Level I and II trauma center had similar outcomes in terms of incidence of pneumonia and mortality.
AbouassalyChadi TMDKauffmanRondiMD, MPHMacnewHeatherMDOKeefeElizabethPhDWoodworthAlisonPhDMayAddisonMD
Venderbilt University Medical Center
PROCALCITONIN IS A USEFUL MARKER TO DIFFERENTIATE BETWEEN INFECTION AND INFLAMMATION IN TRAUMA PATIENTS UNDERGOING ORTHOPEDIC PROCEDURES
Background: Procalcitonin (PCT) has been used as marker of infection, a guide to antibiotic therapy and a measure of response to antibiotic treatment. Since PCT is elevated by the inflammatory response, levels are also elevated following significant surgical or traumatic stress, making its use as a surrogate for infection problematic in these populations. We hypothesized that interval surgical stress following trauma would result in elevations PCT, confounding its use as a marker of infection.
Our aim is to characterize PCT levels in multiple injured trauma patients undergoing orthopedic procedures and assess its value in predicting infection.
Methods: A random selection of patients admitted to the trauma intensive care unit underwent orthopedic procedures including intramedullary (IM) nailing of long bones and open reduction/internal fixation (ORIF) of various fractures. In addition to daily WBC and CRP, daily PCT levels were obtained over a seven day period. PCT was measured on the Brahms Kryptor. Daily maximal temperature (Tmax), and heart rate (HRmax) were also collected. These markers of inflammation were retrospectively correlated with the diagnosis of infection, and the performance of surgical procedures.
Non-normally distributed variables were reported by calculating the median and IQR for each patient and then for the population (infected vs. non-infected) and analysis was conducted using Wilcoxon-rank sum test. Normally distributed variables were reported by mean and standard deviation and differences in the populations analyzed with two sample t-test.
Results: Eighteen patients underwent orthopedic procedures during the seven day course. Seven patients developed infections during the study period: 5 pneumonias, 1 pelvic infection, and 1 gastrostomy tube leak.
Out of all the variables compared in this trauma population, only median PCT was statistically significantly different between these two populations (p = 0.0098). Markers usually accepted as denoting signs of infection or inflammation: Tmax (p = 0.2198), WBC (p = 0.6180), CRP (p = 0.1573), and HRmax (p = 0.6011) did not show a statistically significant difference between the two populations.
Conclusion: In this small population of Trauma patients undergoing orthopedic procedures, preliminary results suggest that PCT may be useful in distinguishing between infected and non-infected patients, while frequently used markers for infection and inflammation such as WBC, CRP, and Tmax were not. A larger, prospective study is needed to confirm these findings.
BonattiHugo JRMDBarrosoLuis FMDSawyerRobert GMDBraymanKennethMDKottonCamielle NMDSifriCosti DMD
University of Virginia
CRYPTOSPORIDIOSIS INCREASES TACROLIMUS LEVELS IN SOLID ORGAN RECIPIENTS: EXPERIENCE WITH SEVEN ADULT CASES FROM TWO CENTERS AND REVIEW OF THE LITERATURE
Background: Diarrhea is a common condition after solid organ transplantation (SOT). Cryptosporidiosis is a rare disease after SOT.
Patient and methods: A retrospective chart review of all cases of cryptosporidiosis in SOT recipients from two centers was performed. Cryptosporidiosis was defined by presence of diarrhea and detection of the pathogen using either microscopy or enzyme immunoassay.
Results: Five renal-, one lung- and one pancreas recipient, median age 51 (range 36–57) years, were diagnosed with cryptosporidiosis median 22.1 (range 3.4–53.1) months post-SOT. Symptoms had existed for median 14 (range 10–42) days before diagnosis (microscopy: 3, EIA: 4) was made. Therapy consisted of azithromycin and/or nitazoxanide. Median TAC levels increased from 6 ng/mL to 22 ng/mL; median serum creatinine increased temporarily from 1.2 mg/dL to 2.4 mg/dL. All patients recovered from enteritis. Thirty-one articles on cryptosporidiosis after SOT were found. Publications from India, South America and the Middle East–all reporting on renal recipients - suggest a high prevalence of the disease in renal recipients in these endemic regions. The majority of the 22 reports from Europe and the US including 39 patients are sporadic cases commonly involving patients with intensified immunosuppression. Renal, pancreas, liver, small bowel and cardiac recipients were affected and 56% of patients were children.
Conclusion: Cryptosporidiosis should be recognized an important cause of diarrhea after SOT. A rise in TAC levels is commonly observed.
HariharaYasushiPhDKonishiToshiroPhD
Kanto Medical center NTT EC
SUBDIVISION OF SURGICAL PROCEDURE GAST AND BILI IN SSI SURVEILLANCE
Background: Recently SSI surveillance according to JHAIS (Japanese Healthcare-associated Infection Surveillance) system is widely performed in Japanese hospitals to reduce SSI rates. However, surgical procedure GAST and BILI in JHAIS system and NHSN system included all gastric surgery from total gastrectomy with lymph node dissection to gastrostomy, and all hepato-pancreato-biliary surgery from pancreaticoduodenectomy, extended hepatectomy to T-tube drainage, respectively. Surgeons specialized in gastric surgery or hepato-pancreato-biliary surgery cannot consider it useful to refer to the SSI rates of all gastric surgery or all hepato-pancreato-biliary surgery. In this paper we proposed the subdivision of surgical procedures GAST and BILI, in order to provide appropriate data for surgeons trying to reduce SSI rates.
Methods: Among 4004 cases of abdominal surgery, 841 cases of gastric surgery (GIST) and 287 cases of hepato-pancreato-biliary surgery (BILI) performed in Kanto Medical Center NTT EC between January 2000 and July 2006 were included in this study.
SSI rates of gastric surgery and hepato-pancreato-biliary surgery were investigated to consider appropriate subdivision of SSI procedure categories.
Results: SSI rates were 93/841 (11.1%)for all gastric surgery, 40/540 (7.4%)for distal gastrectomy and 43/221 (19.5%)for tatal gastrectomy. SSI rate of total gastrectomy was significantly higher than that of distal gastrectomy (p < 0.0001).
SSI rates were 65/287 (22.6%)for all hepato-pancreato-biliary surgery, 14/139 (10.1%) for hepatic surgery, 8/50 (16.0%)for biliary surgery, and 43/98 (43.9%)for pancreatic surgery. SSI rate of pancreatic surgery was significantly higher than those of hepatic and biliary surgery (p < 0.0005).
Discussion: From the practical point of view, subdivision of GAST and BILI into more than three categories is inappropriate. Distal gastrectomy is a common standard procedure of gastric surgery and its SSI rate is significantly lower than those of total gastrectomy or proximal gastrectomy. Total gastrectomy consists of several procedures with or without splenectomy or distal pancreatectomy. However, subdivision of total gastrectomy is considered too complicated for SSI surveillance.
Hepatectomy without bilio-enteric anastomosis is a common standard procedure of hepato-pancreato-biliary surgery and its SSI rate is significantly lower than those of bile duct surgery or pancreatic surgery. Pacreaticoduodenectomy is a standard procedure of hepato-pancreato-biliary surgery and regarding pacreaticoduodenectomy as an independent procedure category of SSI can deliver useful information to surgeons specialized in hepato-pancreato-biliary surgery.
Conclusion: We propose to subdivide GAST and BILI into total gastrectomy, distal gastrectomy, and other gastric surgery; and pacreaticoduodenectomy, hepatectomy without bilio-enteric anastomosis, and other hepato-pancreato-biliary surgery, respectively, for the purpose of properly comparing SSI data among different institutions. It is hoped surgeons can get useful information on SSI rates to make plans to reduce SSI rates.
KamanakaKenjiBAMeadowsMichael CMDChamberlainRonald SMD, MPA
University of Medicine and Dentistry of New Jersey
ACINETOBACTER BAUMANNI: A COLLATERAL DAMAGE PATHOGEN. A REVIEW OF RISK FACTORS AND CURRENT TREATMENT RECOMMENDATIONS
Introduction: Unnecessary or overtreatment treatment of common infections and a lack of interest in the development of new antimicrobials are in part responsible for the increasing number of multi-drug resistant microorganisms. One such pervasive pathogen, Acinetobacter baumanni, was once treated commonly with carbapenems. Since 1991, A. baumanni has rapidly evolved resistance to these drugs and other pharmaceuticals at an alarming rate.
Methods: A comprehensive English and non-English search of all articles pertinent to Acinetobacter baumanni infections was conducted using PubMed, a search engine provided by the U.S. National Library of Medicine and the National Institutes of Health. Keywords searched included: ‘multi-drug resistance’, ‘acinetobacter’, ‘nosocomial’, ‘pneumonia, ‘peritonitis', ‘treatment’ and ‘skin infection’.
Results: Risk factors for various infections caused by A. baumannii including nosocomial pneumonia, peritonitis, and bacteremia were identified. These risks include deficiencies in the implementation of infection control guidelines, prolonged hospital or intensive care unit stay, prolonged or repeated intubation, head injury, acute respiratory distress syndrome, aspiration, previous antibiotic therapy with imipenem, and exposure to fluoroquinolones. A variety of algorithms have been developed for the treatment and eradication of Acinetobacter baumanni infection. These algorithms are not universally applicable, but institutionally dependent on antibiotic sensitivity.
Conclusion:Acinetobacter infections, along with the other organisms associated with the collateral damage of excessive antibiotic usage, are an emerging problem. Such infections should be heeded as harbingers of the developing problems stemming from inadequate enforcement of infection control guidelines, injudicious use of antimicrobials, and the lack of development of new antibiotics. Possible solutions for these problems include the implementation of antibiotic stewardship programs, development of public policy that will foster an environment productive of greater rewards for the development of novel antibiotics and strict enforcement of universal precautions for infection control.
JonesMaris SMDHillCharles R St.MDTsudaShawnMDBarberAnnabel EMD
University of Nevada School of Medicine
SURGICAL SITE INFECTION IN LAPAROSCOPIC INGUINAL HERNIORRHAPY
Objective: To evaluate the incidence of surgical site infection in laparoscopic inguinal herniorrhapy.
Background: An abundance of data supports the practice of antibiotic prophylaxis in open inguinal hernia repair for a reduction in surgical site infections. There is a paucity of data, however, investigating rates of surgical site infection in laparoscopic inguinal hernia repair in conjunction with antibiotic prophylaxis. In the current economic climate, and the prevalence of multi-drug resistant organisms, it is of extreme importance to assess whether or not antibiotic prophylaxis is beneficial in laparoscopic inguinal herniorrhapy. The primary outcome under investigation is surgical site infection in laparoscopic inguinal herniorrhapy with mesh with prophylactic antibiotics in an academic medical center.
Methods: A single institution, retrospective chart review was performed on adult patients who underwent elective inguinal herniorrhapy from 2008–2009. Surgical site infections were recorded in each group utilizing the definition from the Centers for Disease Control. Surgical site infections were included in the data set if they occurred within 90 days of surgery. Both groups received antibiotic prophylaxis according to Surgical Care Improvement Project guidelines. Fisher exact statistical test was utilized to analyze these results; results were concluded to be statistically significant if p < 0.05.
Results: A total of 104 patients were evaluated. The surgical site infection rate for the laparoscopic inguinal hernia repair group was 2.3% (1/42) compared to a 6.5%(4/61) infection rate in the open herniorrhapy group. This difference did not reach statistical significance (p = 0.318).
Conclusion: The rate of surgical site infections after laparoscopic inguinal herniorrhaphy is lower than that for open inguinal herniorrhaphy. This finding suggests that routine antibiotic prophylaxis may not be necessary for laparoscopic inguinal herniorraphy. Future studies with a larger sample size may be required to achieve significance when comparing surgical site infection in laparoscopic inguinal repairs with and without routine antibiotic prophylaxis.
CampbellLynne WBSN, MSN, ARNP-BCZackJeannePhD, RN, CICHansenNancyRN, BSN, CICOdnohaLindaRN, BSNStuckertKevinMHA, BS, RRTHathornTracyRD, LD/N, CNSDTuttleSusanPharmDKoleMarilynMDScottJeffrey MDO
Lee Memorial Health System
A MULTIDISCIPLINARY TEAM APPROACH TO REDUCING CLBSI IN THE ICU
Introduction: Gulf Coast Medical Center is a 349-bed hospital with a 36-bed ICU with complex medical, surgical and transplant patients. Our population is primarily Medicare patients. In trying to improve our outcomes, we established a zero tolerance policy for Central Line Blood Stream Infections (CLBSI) and set about to decrease our monthly CLBSI rate to zero. Prevention of nosocomial bloodstream infections is a priority in the intensive care unit. These infections prolong the patient's hospitalization by a mean average of 7 days with an attributable cost increase between $3,500 and $30,000 per incidence. It is estimated that 90% of catheter related bloodstream infections are related to central venous catheters. (CVC) The Central Line Bundle, which is a group of best practices, was developed and has been proven to decrease the central line bloodstream infection rate.
Background: In 2008 there were 21 CLBSI in our ICU. Between January and April 2009 there were 10 CLBSI in our ICU. This upward trend was alarming so we began evaluating our practice to improve our outcomes.
Methods: As part of the Lee Memorial Health System, we participated in the IHI initiative to decrease CLBSI. We were already using the central line bundles with each patient, so we looked at other ways to more efficiently decrease our risk of infection. We changed our focus during rounds to include a multidisciplinary approach. The entire team was encouraged to become engaged and take an active role. The necessity for CVC was addressed on a daily basis. The nursing staff was encouraged to be more proactive in discontinuing the CVC. Insertion dates, last dressing change, and site appearance were all reviewed. Our mid-level providers assessed the sites daily during their examination of the patients. Changing the CVC was at the discretion of the attending physician. Criteria included if the CVC was greater than 10 days old or the patient had an increase in white blood cell count, or if the site was questionable. The subclavian area was the site of choice. If not optimal then the internal jugular vein was used. The CVCs were discontinued if there were no vasopressors, nutrition, etc., infusing and a peripheral IV or PICC line could be placed. In order to solidify our processes, we had an outside consultant evaluate our methods and practices. Her focus was on educating nursing staff using proven tools as well as bedside training to aid in decreasing risk of contamination and improve line care post placement.
Results: After implementation of the above changes in our practices, we have had a zero monthly CLBSI rate for the past 7 months.
Conclusion: By adding a multidisciplinary team approach, increasing nursing education, heightening awareness, and following CDC guidelines for care of CVC, we were able to meet our goal of zero CLBSI. We continue to use bedside nursing education and encourage team engagement. This empowers all members of the staff to actively participate and take ownership in the prevention of CLBSI in our ICU.
SURGICAL INFECTION AND RISK FACTORS IN A GENERAL SURGERY SERVICE: A PROSPECTIVE STUDY
Pablo Vazquez Aragon, Medicine, Pedro Cascales Sanchez, Medicine, Maria Teresa Villar Canovas, Medicine, Antonio Serafin Valero Liñán, Medicine, Juan Luis Rueda Martinez, Medicine, Antonio Prat Calero, Medicine, Maria Abad Martinez, Medicine, General and University Hospital Albacete Spain
Introduction: Along the history, hospitals have coexisted with the nosocomial infection , defined as "that infection that was not present neither was incubating at the moment of patient admission at a hospital. In our medium, between 6% and 14% of the patients that enter in general hospitals develop a nosocomial infection. In order of frequency, the urinary tract infection represents 42% of all infections, following by the surgical infection, previously denominated as "surgical wound infection" with 24%, nosocomial pneumonia with 15- 20% and bacteremia with 5%.
Background: The aim of the study was quantifying the frequency of surgical infection in a service of general surgery from a tertiary-care hospital of the Spanish National Health System and know the risk factors for its acquisition.
Methods: From 1/1/1995 to 31/12/1998 a prospective, longitudinal, descriptive and analytical study of a cohort of 2794 patients who underwent a surgical procedure with a post-surgery stay longer than 48 hours was carried out. The used infection criteria were the defined by the Centers for Disease Control and Prevention (CDC).
Results: During their stay at hospital, 314 patients (11,23%) of the cohort presented any type of hospital infection. The more frequently nosocomial infection was surgical infection with a global accumulated incidence of 7.7%, ranging from 3.4% for clean surgery to 23.7% for dirty surgery. It is followed In order of frequency by the urinary tract infection and bacteriemia with 1.5%, and nosocomial pneumonia with 0,5%. The incidence of surgical infection for NNIS index was 0 = 2.2%, 1 = 6.8%, 2 = 15.6% and 3 = 28.2%.
Conclusion: The stay prior to surgery, the number of days with urinary probe, with central catheter, with mechanical ventilation as well as the use of antimicrobial prophylaxis were found factors to modify on the way to prevent nosocomial infection.
HaithLinwood RJr.MDAckermanBruce HPharmDHornbeekHeidiMDPattonMary LMDGuildayRobert EMD
Crozer-Chester Medical Center
SCEDIOSPORIUM BRAIN ABSCESSES IN A PATIENT WITH A PATENT FOREMEN OVALE CAUSED BY SINUSITIS AND FUNGAL PNEUMONIA FOLLOWING A WORK-RELATED BOILER EXPLOSION
Introduction: Fungal infections are reported in approximately 11 to 17% of thermal injury patients. The most common infections involve Candida species and Aspergillus species infection, thus routine treatment of fungal infections often includes either fluconazole or an ehcinocandin when Aspergillus spp. is suspected.
Case: A 50 year old male suffered a steam boiler explosion in an enclosed space. The patient was intubated and transferred to our burn treatment center with an estimated total body surface area flame injury of 64% with inhlation injury and confirmed C-3 to C-6 spinal column stenosis. The patient was hemodynamically stable with ventilatory support. Following consensus fluid resuscitation, the patient eventually developed a positive sputum culture with Escherichia coli and nasal cultures with Staphylococcus aureus. The patient was taken to surgery for excision and grafting on post-burn day (PBD) 3 and following surgery a chest x-ray revealed a right upper lobe consolidation and new Acinetobacter baumannii isolate. On PBD 15, bronchoscopy with bronchooalvelolar lavage revealed A. baumannii, Klebsiella pneumoniae, Aspergillus fumagatus and Verticulum species. On PBD 23, a sudden neurological change was noted with areflexia and flaccid paralysis and magnetic resonance imaging of the brain revealed 13 ring enhancing lesions consistent with multiple brain abscesses. On PBD 33, an echocardiogram demonstrated a patent foramen ovale. The patient was taken to the operating room for brain biopsy and abscess drainage. Cultures isolated S. aureus and Scediosporium apiospermum warranting a change to voriconazole. Three weeks after initiation of voriconazole, a CT scan of the brain revealed no further lesions and resolution of edema in the ring enhancing lesions. On repeat CT scan 8 days later regression was noted in the lesions.
Conclusion: Initial fungal therapy was selected presuming that the A. fumagatus in the lung was the causative organism in the brain abscesses. The worsening clinical course while being treated with caspofungin warranted brain abscess drainage and culture, which revealed a fungal organism inherently resistant to caspofungin.
CantosMae FBSc, MDKapusAndrasMD, PhDAilenbergMenachemPhDRotsteinOri DMD, MSc
St. Michaels Hospital
LIPOPOLYSACCHARIDE ALTERS THE GENETIC EXPRESSION OF KEY ENZYMES IN CERAMIDE METABOLISM
Rationale: Lipopolysaccharide (LPS) is a prototypical inducer of innate immunity with its receptor (TLR4) involved in inflammation signaling pathways. Activated TLR4 is found in the plasma membrane in lipid rafts containing ceramide. Ceramide has many important functions within the cell. It makes up part of specialized formation (lipid rafts) which act as signaling platforms. Ceramide also functions as a cell signaling molecule itself and is involved in many cellular functions from apoptosis to inflammatory responses. Ceramide can be generated via a multitude of mechanisms – mainly from the breakdown of sphingomyelin located in the plasma membrane by sphingomyelinases and de novo synthesis. It has been shown that LPS increases ceramide. Our objective is to understand the mechanisms by which LPS affects ceramide production through either an increase in production and/or a decrease in degradation by regulation of enzyme expression.
Hypothesis: Gene expression of key enzymes in ceramide metabolism is altered after LPS exposure. To demonstrate this we will treat macrophages with LPS and will expect to see an increase the gene expression of acid sphingomyelinase (ASM ) and/or neutral sphingomyelinase (NSM).
Methods: We have treated cells with various dose and time exposures to LPS and measured the amount of enzymatic mRNA using quantitative real-time Polymerase Chain Reaction (qPCR). In addition, we have used inhibitors to elucidate which pathways LPS utilizes to bring about the effects seen.
Results: We have shown a decrease in mRNA level of both ASM and NSM at 4 and 8 hours of LPS exposure by qPCR.
Conclusion: While ceramide concentrations are known to be elevated acutely after exposure to LPS, the effect of inflammatory mediators on key enzymes of ceramide metabolism have not been elucidated. The aim of our studies was to explain if LPS affect the level of key enzymes at the genetic level. We have concluded that gene expression, although an indirect method to measure enzymatic activity, is altered after exposure to LPS. We have focused on one key enzyme, ASM, which seems to act in a negative feedback mechanism.
YamagishiYukaMDMikamoHiroshigeMD, PhD
Aichi Medical University
A CASE OF CAT BITE INFECTION AS POLYMICROBIAL INFECTION CAUSED BY PASTEURELLA MULTOCIDA AND PREVOTELLA SPECIES
Introduction: We have encountered a case of cat bite infection as polymicrobial infection caused by Pasteurella multocida and Prevotella species.
Case: A 67-year-old man who had not received diabetic treatment. Although the fifth finger of his left hand was bitten by a homeless cat, he had not received medical care. Since the bite infection had worsened, he consulted private clinic and had received wound treatment with disinfectant every day. In spite of wound treatment, the bite infection had worsened and had also noticed that the movability of his finger had not been well even 30 days later after injury. The clinic doctor performed surgical drainage, while his wound had not recovered. Therefore, he consulted Aichi Medical University Hospital and was admitted to the department of orthopedics 32 days after injury. His left fifth finger was odiferous and reflex tendon was melted. X ray, CT, and MRI showed osteomyelitis. He was diagnosed as osteomyelitis and tendon necrosis. Cleansing and drainage ware thereafter performed daily, and an antimicrobial agent was systemically administered. We started teicoplanin, 18.0 g/day of piperacillin-tazobactam, and 2.4 g/day of clindamycin. Because P. multocida was detected on culture, we changed from CLDM to MINO to cover enough the range of antimicrobial spectrum of Rickettsia species. 45th days of accident, he had his 5th finger amputed. At 47th day after bites, MINO was stopped because of drug allergy induced by MINO. Subsequently, his condition gradually improved and he left the hospital on the 60th days after injury. Prevotella species was identified based on cultivation study. We diagnosed his infection as a polymicrobial infection caused by P. multocida and Prevotella species.
Conclusion: Mixed aerobic and anaerobic infection is often present in the cat bite infection. The antibiotics should be cover beta-lactamase-producing aerobic and anaerobic species until pathogens are isolated.
ByrnesMatthew CMDAdegboyegaTitiBARiggleAndrewBABeilmanGregMDChipmanJeffreyMD
Univerisity of Minnesota
NASAL SWAB SPECIMENS THAT ARE ROUTINELY COLLECTED TO SCREEN FOR MRSA IN INTENSIVE CARE UNITS CAN BE USED TO PREDICT THE PRESENCE OF MRSA IN CLINICAL CULTURES
Introduction: Many hospitals screen patients for MRSA upon admission to the ICU. To date, the utility of this information has been epidemiologic in nature only. We hypothesized that this screening information could be used clinically to assist with empiric antibiotic decisions.
Methods: Medical records of patients admitted to a university affiliated community hospital as well as a tertiary care university hospital were reviewed. Patients admitted to the ICU were screened for MRSA colonization with a nasal swab that was analyzed with either chromogenic medium or polymerase chain reaction (PCR). The results of the nasal swab were compared with clinical culture results. We defined concordance as clinical culture results that matched the nasal swab screen and discordance as clinical culture results that did not match the nasal swab screen. The number of days separating the nasal swab from the clinical culture was also noted.
Site
PCR
Chromogenic Media
P value
Overall
88%
66%
0.006
Sputum
93%
68%
0.005
Wound
70%
62%
0.67
Blood
100%
83%
0.38
Urine
100%
100%
1
Results: There were 141 patients included in the study. The mean age of patients was 59.7 years. The mean hospital length of stay was 19.3 days, with an ICU length of stay of 11.75 days. There were 167 clinical cultures performed in the study patients. The majority (70%) of cultures were performed on sputum specimens in an effort to diagnose pneumonia. The remaining cultures were performed on blood (10.1%), wound (21.5%), and urine (3.4%). The overall concordance between nasal swab results and clinical culture results was 69.5%. This concordance rate, however, was significantly higher for nasal swab screening performed within six days of clinical cultures compared with nasal swab screening performed seven days or more before clinical cultures were obtained. (79% vs. 46%; p < 0.0001). Concordance rate also varied significantly depending on the surveillance method used to detect MRSA. The concordance rate for patients screened with PCR within six days of developing an infection was significantly higher than patients screened with chromogenic media (88% vs. 65.5%; p = 0.006). Concordance rates of PCR vs. chromogenic medium are listed in the table.
Conclusion: MRSA screening with PCR through nasal swab specimens carries a high concordance rate with clinical cultures. Clinicians may be able to use these results to tailor more appropriate empiric antimicrobial regimens. The results with chromogenic media screening are markedly lower, which suggests that clinicians should view these results with caution.
ByrnesMatthewMDRiggleAndrewBABeilmanGregMDChipmanJeffreyMD
University of Minnesota
ABDOMINAL WALL WOUNDS SURROUNDING HIGH OUTPUT ENTEROCUTANEOUS FISTULAS CAN BE SUCCESSFULLY SKIN GRAFTED
Introduction: Enterocutaneous fistulas are often associated with large abdominal wall wounds as a result of necrosis and debridement. Successful skin grafting of these wounds is difficult to achieve, as the wound bed is constantly bathed by enteric contents. A method to successfully skin graft these wounds would provide a significant advancement to their treatment, in that wound closure could be markedly accelerated.
Methods: Medical records of patients undergoing skin grafting of a wound around an enterocutaneous fistula were reviewed. The amount of fistula output at the time of skin grafting was recorded. The method of skin grafting as well as the method of protecting the graft from enteric exposure was noted. Skin grafts were evaluated for "graft take." This analysis was done at 1–2 weeks after the initial operation as well as at follow up appointments.
Results: Seven patients were identified that met inclusion criteria. After 1–2 weeks, the graft take was 90% in 3 patients, 80% in two patients, and 50% in 2 patients. After 1 month, there was complete epithelialization in 85% of patients, while one patient had mostly epithelialized. This allowed placement of an ostomy device in all patients. The fistula output was greater than 400 mL per day in 70% of the patients. Multiple techniques were used to divert enteric flow away from the skin graft. Six of the patients were treated with a modification to the standard wound vac. A defect was cut in the sponge overlying the fistula. Ostomy paste was placed along the sponge interior, such that enteric contents could not be suctioned into the sponge. This held the graft in place, while diverting the enteric contents. In one of these patients, a Foley catheter was placed in the fistula to divert the enteric flow. One patient was treated with continuous irrigation and suction of the wound, which kept the graft clean and allowed full healing.
Conclusion: The presence of a high output enterocutaneous fistula does not preclude successful skin grafting of abdominal wounds. Successful grafting can accelerate the process of wound healing as well as improve skin and wound hygiene by allowing the placement of an ostomy device.
HaithLinwood RMDPodolskyErica RMDGuildayRobert EMDPattonMaryLouMDNeeliSurekhaMDOkechukwuNathanMD
Crozer Chester Medical Center
CALCIFIC UREMIC ARTERIOLOPATHY: A COMBINED AGGRESSIVE CONJOINT NEPHROLOGY/BURN SURGERY MANAGEMENT
Introduction: Calcific uremic arterilopathy (CUA), commonly called calciphylaxis, is a systemic calcification of arterial medial and soft tissues causing various quantities of soft tissue destruction and potential infection.
Background: The incidence of CUA has been increasing in recent years due to an increased awareness among physicians (Wang, KL et al. Kidney Int. 70 [2006]: 1196) as well as aggressive treatment of hypocalcemia with vitamin D in chronic kidney disease patients. It has been estimated that 1% of end-stage renal disease patients develop CUA each year increasing in prevalence to 4% in dialysis patients yet more common post renal transplant failure. Mortality, most commonly a result of wound infection may approach 80% (Scully, RE et al. NEJM 2001;345;1119).
Methods: We present a case of CUA in a 32 year old female patient post renal transplant failure subsequently diagnosed with hyperparathyroidism and was treated initially with cinacalcet. Despite that, her parathyroid hormone level remained high (3110 pg/ml) and she underwent parathyroidectomy. Over the subsequent 4 weeks she developed dark, painful ulcerating lesions of her breast and abdomen. She was treated on the med-surgery floor by nephrology service with daily silver sulfadiazine dressings. Development of new torso lesions prompted the addition of sodium thiosulfate to her regimen. Because of deterioration of her wound status and severe wound pain she was transferred to the Burn Service. Her treatment consisted of multiple dedridements with temporary closure utilizing a silver nylon dressing in conjunction with a negative pressure device. The wounds were ultimately closed with a two stage Integra@ grafting system or primary closure where possible. Pain was controlled as typical in our burn center with analgesics titrated to the degree of pain that the patient was experiencing.
Results: The grafted wounds healed well as did the wounds closed primarily. The patient remained infection free and was discharged home.
Conclusion: This experience has prompted us to formulate a treatment paradigm for patients with CUA. We believe that because wound infection is the primary cause of death, appropriate and aggressive surgical wound management as well as adequate pain control is absolutely necessary. However, we realize that aggressive renal replacement and management is also indispensible to halt progression of the presenting lesions as well as preventing development of new areas of calcification and necrosis.
KleinJeffrey AMD, MPHCameronAtoussaRN, NPCokerJoAnnRN, NPLangmanLoralieMDSnozekChristineMD
University of California, Riverside
TUMESCENT ANTIBIOTIC DELIVERY FOR SSI PROPHYLAXIS
Introduction: Tumescent antibiotic delivery (TAD) is the subcutaneous (subq) infiltration of large volumes (typically >1 L) of dilute antibiotic in a solution of tumescent local anesthesia (TLA). TLA is a dilute solution of lidocaine (0.5 to 1 gm/L), epinephrine (0.5 to 1 mg/L) and sodium bicarbonate (10 meq/L) in normal saline. Compared to IV antibiotic delivery (IVAD), we hypothesized that TAD will 1) increase the area under the concentration (conc.)-time curve (AUC) & peak (Cmax) antibiotic conc. in subq tissue at a surgical incision site, thus killing more incision site bacteria and 2) decrease AUC & Cmax in serum, reducing the risks of bacterial antibiotic resistance and C. difficile colitis.
Background: TLA produces intense vasoconstriction, delayed lidocaine/antibiotic absorption and surgical anesthesia for >8 hours. Maximum safe tumescent lidocaine dosage is 35 mg/kg. Lidocaine is bactericidal.
Methods: With IRB-approval, 4 subjects received cefazolin IVAD and TAD on repeated occasions. One pt received metronidazole (Met) & Cef. TAD was achieved using blunt-tipped Monty infiltration cannulas and peristaltic tumescent infiltration pump. Areas treated were abdomen (patient #1 & #4), female breasts (pt #2) & hips-outer thighs (pt#3); pt #4 received Cef & Met. After TAD or IVAD, blood was sampled at 1 to 2 hour intervals for >12 hours. After TAD, samples of subcutaneous fat/tumescent fluid were aspirated every 1 to 2 hrs over >8 hrs by hand-held syringe-liposuction. Samples were centrifuged. Serum & subq interstitial tissue fluid were assayed for Cef and Met by HPLC.
Results: Patient #1 (reported here) was studied 3 times (TAD 1000mg Cef/1111ml, TAD 500mg Cef/1061ml, & IVAD 1000mg Cef) at least 1 week apart. See graph. The 10 hr cefazolin AUC & Cmax for TAD & IVAD were:
Tissue Cef (TAD 1000 mg) AUC = 4782 Cmax = 823
Tissue Cef (TAD 500 mg) AUC = 2280 Cmax = 456
Serum Cef (TAD 1000 mg): AUC = 167 Cmax = 20
Serum Cef (TAD 500 mg): AUC = 82 Cmax = 11
Serum Cef (IVAD 1000 mg) AUC = 315 Cmax = 146
AUC Ratio TAD 1000 mg:IV 1000mg = 4782/315 = 15.2
AUC Ratio TAD 500 mg:IV 1000mg = 2280/315 = 7.2
The 3 other patients (to be presented) had similar results.
Conclusion: In subq tissue fluid AUC for TAD 1000 mg Cef & TAD 500 mg Cef yield 15.2 & 7.2 times AUC for IVAD 1000 mg Cef, respectively (we assume subq tissue Cef conc. after IVAD < concomitant serum Cef conc.). In serum, AUC & Cmax are less for TAD than IVAD, but with TAD the duration of Cef in serum is prolonged. Based on pharmacokinetic absorption characteristics, antibiotic surgical site infection prophylaxis by TAD may be better & safer compared to the current standard of care using IVAD.
PoslusznyJoseph AJrMDHicksChindoPhDShankarRaviPhDGamelliRichard LMD
Loyola University Medical Center, Case Western Reserve University School of Medicine
INCREASED INFECTIONS ARE ASSOCIATED WITH NON-OPERATIVE TRANSFUSIONS IN BURN PATIENTS
Introduction: Blood transfusion is associated with increased rates of infection in trauma and burn patients. For burn patients, transfusion rates have decreased with the implementation of strategies to reduce operative blood loss and lower transfusion thresholds. > 60% of all transfusions in burn patients occur outside the operating room. The relationship between non-operative transfusion and infection has not been extensively explored. We hypothesized that transfusions administered outside the operating room (non-OR) are a function of the severity of the critical illness rather than the size of the burn and that total transfusions and the % of non-OR transfusions are associated with increased risk of pneumonia, bloodstream infection, and sepsis.
Methods: Infection, clinical and transfusion data were obtained from 60 adult burn patients with >20% TBSA burn. Infection data included development of pneumonia, bloodstream infection and sepsis. Clinical data included age, APACHE II score, % TBSA burn, inhalation injury, number of ventilator days (NVD) and number of operative events (NORE). Transfusion data included total transfusions and % non-OR transfusions. Linear correlation, univariate analysis and adjusted stepwise logistic regression were used to determine relationships between infection, transfusion and clinical variables.
Results: Infection rates included: pneumonia 35/60 (58%), bloodstream infection 17/60 (28%) and sepsis 7/60 (12%). The average age was 45 ± 2 years, APACHE II score was 22 ± 1 and % TBSA burn was 40 ± 2%. 48% (29/60) of the patients had an inhalation injury, the average NVD was 35 ± 5 days and NORE was 3.0 ± 0.4 events. 996 units of pRBCs were transfused to 60 patients (17 ± 3 units/patient). 62% of all transfusions were outside the OR (non-OR). APACHE II score, % TBSA burn, inhalation injury, NVD and NORE all correlated with total transfusions. However, the % of non-OR transfusions only significantly correlated with APACHE II score (p = 0.02) and showed a strong trend with NVD (p = 0.06). There was no correlation between % non-OR transfusions and other clinical variables. Total transfusions and % non-OR transfusions were significantly increased in patients with pneumonia, bloodstream infections and sepsis (Table).
When compared with clinical variables, total transfusions still correlated with bloodstream infections and sepsis, and % non-OR transfusions correlated with pneumonia, bloodstream infection and sepsis.
Total Transfusions
% non-OR Transfusions
Pneumonia
No
8 ± 2
42 ± 6%
Yes
23 ± 4
61 ± 3%
Bloodstream Infection
No
10 ± 1
49 ± 4%
Yes
33 ± 8
65 ± 4%
Sepsis
No
13 ± 2
51 ± 4%
Yes
48 ± 17
72 ± 4%
Mean ± SE; p < 0.05, no v. yes for all; two-sample paired student's t-test
Conclusion: Transfusions outside of the OR are a function of the initial injury severity (APACHE II score) and the duration of the critical illness (number of ventilator days). These transfusions, in particular, have a significant impact on the development of pneumonia, bloodstream infections and sepsis. Developing methods to decrease non-operative transfusions and more aggressively targeting the mechanisms that lead to anemia in these patients are essential to reducing transfusion-related increases in infection.
PoroykoValeriyPhDAlverdyJohnMDLiuDonaldMDMorowitzMichaelMD
The University of Chicago
SINGLE CELL METAGENOMIC ANALYSIS OF GUT BACTERIA FROM HUMAN INFANTS WITH NECROTIZING ENTEROCOLITIS
Background: High-throughput single cell sequencing of individual bacterial cells has revolutionized our ability to study microbial communities in the environment and within the human body. However, single cell metagenomic analysis of intestinal bacteria has not yet been performed due to technical hurdles. The goal of this study was to perform metagenomic sequencing analysis of bacterial cells isolated from intestinal tissue resected from babies with neonatal necrotizing enterocolitis (NEC).
Methods: With institutional approval, we collected and cryopreserved small intestinal segments from 3 human infants undergoing bowel resection for complicated NEC. We developed a novel protocol to collect single microbial cells after removal of human epithelial cells and lymphocytes. A single intestinal segment (1 cm2) from each infant was gently shaken in wash buffer containing 50 mM sodium phosphate and 0.1% Tween 80, and spun at 200g for 15 min. Host tissue was discarded and the supernatant was spun at 30,000g to allow for precipitation and collection of free prokaryotic cells. Cells were stained with 10x SYBR green nuclear stain and sorted with a MoFlo cytometer equipped with a robotic arm for sorting into plates. Bacterial cells were disrupted by boiling and then whole genome DNA amplification was performed using REPLI-g UltraFast Mini Kit (Qiagen). To characterize the number of bacterial species present in each sample, the gene encoding the 16S ribosomal subunit was PCR amplified in an aliquot of each DNA sample and temporal temperature gradient electrophoresis (TTGE) was performed.
Results: We analyzed intestinal segments from 3 infants with NEC. Using FACS cell sorting, we quantified and collected 1200 bacterial cells (12 aliquots of 100 cells each) from each resected segment. We confirmed by PCR that our collections of isolated bacterial cells contained the 16S ribosomal RNA gene, whereas eukaryotic cells did not. Thus, these collections of microbial cells were successfully depleted of human epithelial cells and lymphocytes, making it possible to sequence the genomes of these species without eukaryotic DNA contamination. 16S PCR amplicons were further analyzed by TTGE, demonstrating that each intestinal specimen contained only 2 or 3 bacterial species and that these species differed in each specimen. This is consistent with published studies demonstrating limited species richness and high interindividual variability in the gut bacterial communities of premature babies. Taxonomic identification of the species in our samples is pending. Whole genome metagenomic sequencing of the DNA from these species will be completed in January 2010.
Conclusion: We have successfully isolated individual bacterial cells from the small intestinal mucosa of human infants with NEC. This positions us to complete the first published single cell metagenomic analysis of bacteria associated with the human gastrointestinal tract. The results of this study will yield valuable genomic information regarding mucosa-associated microbes in NEC, and it will also have broad implications for the study of gut bacteria in a wide range of clinical settings.