
Abstract
Abstract
Background:
Surgical site infections (SSI) are the third most common hospital-acquired infections and account for 14% to 16% of all such infections. In elective colorectal operations, the international SSI rate ranges from 4.7%–25%. In a previous retrospective study in this department, the SSI rate was unacceptably high (25%), and the promising different international evaluations of triclosan-coated suture materials encouraged us to create a multicenter randomized trial to improve our results. The main goal of this study was to compare triclosan-coated and uncoated absorbable suture (PDS Plus® with PDS II®) in elective colorectal operations.
Methods:
This was an internet-based study involving seven surgical centers. All the elective colorectal operations were performed by experienced surgeons. For abdominal fascia closure, running looped PDS was applied; triclosan-coated or uncoated PDS was chosen by computer randomization. Pre-operative and peri-operative variables such as gender, body mass index, neoadjuvant therapy, type II diabetes mellitus, amount of wound dressing material used, nursing days, and microbiological results were recorded. After the operation, the patient's data and risk factors were collected in a password-protected online database.
Results:
From 485 patients randomized, SSI was documented in 47 patients (12.5%), 23 (12.2%) in the group having triclosan-coated sutures (n=188) and 24 (12.2%) in the uncoated suture group (n=197), a non-significant difference. Of all SSIs, 13 (27.7%) were diagnosed only after discharge, being recognized in the outpatient setting, with four patients in the triclosan suture group (8.5%) and nine in the uncoated suture group (19.2%) being affected with no significant differences in the demographic data. Microbiological examinations, in addition to the same colon flora in both groups, revealed two gram-positive infections in the uncoated suture group. The hospital stay and costs of dressings were significantly higher in patients having SSIs.
Conclusion:
Compared with the previous retrospective studies of this department, the implementation of looped PDS decreased the incidence of SSI by one-half, whether the suture was triclosan-coated or not. It seems that patient factors are less important than operative factors in the occurrence of SSI, and there were no differences between elective colon and rectal operations in the development of incisional infections. No beneficial effect of triclosan against gram-positive bacteria, which has been reported in the literature, could be confirmed in our study. We could not show an effect against gram-negative enteric microorganisms. Higher additional costs and longer hospital stay with SSI were confirmed.
Surgical site infections prolong hospitalization. Expensive and more dressing materials are used, longer antibiotic treatment must be administered, and, later, the rate of incisional hernias is increased. These infections can invade the abdominal cavity, necessitating re-operation. Death may follow infectious complications.
Several international studies show the value of certain surgical sutures and wound closure techniques in decreasing the SSI rate [4]. This topic is important also in sterile-contaminated surgical interventions. It is generally accepted that absorbable, monofilament sutures can lower the SSI rate, with running sutures being superior to the interrupted technique. Subcutaneous sutures have not shown benefit in the prevention of infection [12].
A new improvement from Ethicon (Somerville, NJ) is monofilament absorbable suture coated with the antiseptic agent triclosan. The coating is claimed to provide protection against colonization of the tissues around the suture [13,14]. This effect lasts for about 30 days. It has been demonstrated through in vitro studies that triclosan forms an inhibition zone around the suture and is effective against the most frequent pathogens causing SSIs (e.g., Staphylococcus aureus, S. epidermidis) [13]. Several clinical studies have demonstrated its efficacy and advantageous cost: benefit. For example, a study by a group of thoracic surgeons in Vienna showed that SSI after sternotomy increases the hospitalization cost to US$11,200 per patient, whereas surgical site healing disorders did not occur in any of the cases in which triclosan-coated sutures (Vicryl [polyglactin 910] Plus®, Ethicon) were used, resulting in only US$9 in additional cost per patient [15]. On the other hand, a group of Dutch plastic surgeons cautioned against the use of triclosan-coated sutures, as they found a significantly higher dehiscence rate in breast incisions closed in this way [16]. However, a large number of publications favor the use of triclosan, as it reduces significantly the probability of SSI development [17–21], but not invariably [22].
According to in vivo studies, both the absorption and tensile strength of polyglactin 910 with triclosan are identical to those of polyglactin 910® [23], which has been in practical use for years. Several studies prove its efficacy in reducing SSIs. Triclosan is not an antibiotic; it is an antiseptic material. It has no toxic, teratogenic, or irritating effects at the standard concentration [24]. However, its antiseptic effect in relation to SSI has been studied primarily for gram-positive pathogens; the experience against coliform (gram-negative) bacteria, which form the basis of the colonic flora, is sparse. Nevertheless, when testing the effects of triclosan on various E. coli strains in orthopedic infections, a 90% reduction in SSI was achieved [25,26].
Gram-positive bacteria are the most common cause of infections of the surgical intervention port in most operations, but in procedures involving colon opening, colonization of the site by typical gram-negative bowel organisms (Enterococcus, Escherichia coli, Enterobacter, Proteus, Klebsiella) is significantly more common [27].
During the first part of 2009, at the Department of Surgery of The University of Pécs, the SSI rate for elective colon and rectal operations was evaluated retrospectively. This rate turned out to be 25%, which is slightly worse than in the international literature [28]. We sought methods of reducing the likelihood of infection.
For planning this study, a pilot study was performed to compare coated and uncoated sutures. Among abdominal fascia closure fifty patients, 25 received triclosan-coated polyglactin 910 suture and the others uncoated suture. After analyzing the data, a significant difference was found in favor of the triclosan-coated suture (SSI rate 5% vs. 20%). On the basis of these results, a sample size calculation was done to increase the power of the study to 90% to detect a decrease or the historic 20% SSI rate to <10%. On this basis, 468 colorectal surgery patients were planned for.
Closing the abdominal fascia with monofilament absorbable running suture was the routine in our department and in other high-volume departments in Hungary. The most popular suture was PDS II® (polydioxanone). When the trial started, PDS Plus® (triclosan-coated polydioxanone) had become available in our market, without it being tested before in a randomized study. Therefore, the aim of the study evolved to a comparison of polydiaxanone suture with and without triclosan in seven high-volume Hungarian surgical institutions over a one-year period.
Patients and Methods
The primary goals were to determine whether triclosan-coated polydiaxanone is able to reduce the number of SSIs after colorectal surgery. Is triclosan-coated surgical suture material able to inhibit the growth of colon microorganisms as well as has been claimed for skin organisms? Can this abdominal closure technique be recommended to practitioners of colorectal surgery? The secondary goals were to determine whether an SSI increases the length of the hospital stay, whether there are any additional costs, and the chances of late SSI after discharge of the patient from the hospital.
A multi-center-randomized, internet-based study was designed involving seven surgical centers (three university clinics and four high-volume hospitals) selected to cover the country geographically (Fig. 1). Coordination was provided by the Surgical Department of The University of Pécs. All of the enrolled patients underwent elective colon or rectal surgery between December 2009 and November 2010. Each operation was performed by an experienced surgeon; i.e., one who performs at least ten colon or rectal operations annually. In accordance with the laws and regulations applicable to the study locations, each center was responsible for obtaining approval of the protocol and its amendments and the informed consent form, study recruitment procedures, and any other relevant documentation regarding the study from the appropriate ethics committee prior to commencement of the study. This was an investigator-initiated study. The study was officially recorded as Abdominal Wall Closure with Triclosan-Coated Suture (TCS09-10) with ID Number NCT01123616 at ClinicalTrials.gov.

Seven high-volume sites of study.
The examination was prospective, and the randomization was made by computer software (stored in a password-protected website [29]) and could not be influenced manually. A participating center could not view the data from the other centers. Four study meetings were held to cross-check and evaluate the data.
The inclusion criteria were age between 18 and 80 years with benign or malignant colon or rectal disease undergoing an elective open surgical procedure involving an enterotomy. Patients with systemic disease influencing local surgical site healing (e.g., type I diabetes mellitus, Child-Pugh class B–C liver cirrhosis, and chronic kidney disease necessitating dialysis) or those having immunosuppressive treatment or inflammatory bowel disease were excluded. Also, acute operations with unprepared bowel and patients who refused to sign the consent form were excluded. Some patients with intra-operative findings such as locally incurable tumor or sepsis (abscess, necrotic tumor), or with post-operative findings such as further surgical intervention through the site and patients who withdrew the consent later, also were excluded. Undesirable complications such as sterile surgical site dehiscence and suture breakage during the post-operative period also led to exclusion from the trial.
At the randomization phase, the following data were recorded in an internet database: The patient's initials; the health insurance number; the patient's age, weight, height, clinical diagnosis, history of disease that may influence surgical site healing (e.g., type I diabetes mellitus, jaundice, long-term corticosteroid intake, body mass index [BMI], liver failure [Child-Pugh class B–C], end-stage renal disease [hemodialysis, peritoneal dialysis]); previous abdominal operations and type of incision; and neoadjuvant therapy, including the name of the protocol and the number of treatments. The evaluation concluded by confirming that the surgical intervention was elective and not acute. Prophylactic antibiotic (a second-generation cephalosporin and metronidazole 30 min before incision) and disposable drapes were used in every case.
For closure of the abdominal fascia, running looped PDS was used. Use of triclosan-coated or uncoated PDS was determined by computer randomization. Separate peritoneal closure and subcutaneous sutures were optional, depending on the surgeon's preference, but if applied, 2-0 suture was used. Interrupted 2-0 poliglecaprone 25 (Monocryl Plus®, Ethicon) was employed for the skin closure. After the operation, the following data were entered in the website database: Duration and date of the operation, type of intervention (colotomy, cecal resection, right hemicolectomy, left hemicolectomy, segmental resection, sigmoid resection, abdominal rectal resection, hemicolectomy, transversectomy, cecal resection, colotomy, abdomino-perineal [A-P] resection, subtotal or total colectomy), the presence of an ileostomy or colostomy, and the technique of abdominal closure (abdominal wall: continuous suture or continuous with intermittent interrupted stitches, type of peritoneal sutures, and subcutaneous sutures). Any sign of carcinomatosis or ascites and the surgical resectability were documented as well.
After the operation, the incision sites were examined during the hospital stay, and the following data were recorded: Pain scale, signs of SSI, type and quantity of wound discharge (serous, pustulous, feculent), status and penetration of SSI (superficial incisional, deep incisional, abdominal dehiscence), microbiological results (type of bacteria and antibiotics given), number and type of dressings, local lavage, interventions (abdominal lavage, drainage, reoperation), infectious complications of the abdomen (suture insufficiency, abscess, peritonitis), and the number of nursing days. Thirty days after discharge, followup was made by telephone, and information such as clinical intervention, outpatient registration attributable to late SSI, or readmission was collected in the database. Adjuvant chemotherapy was not allowed to be started within the 30-day follow-up period.
Statistical analysis was performed using the Student t-test for continuous variables and a test for independence (chi-square test) for categorical variables. All means were expressed±standard deviation. A p value <0.05 was considered significant.
Results
A total of 468 patients were suitable for randomization, but 83 (18.1%) were excluded later because of the finding of inoperable tumor (45 cases; 54.2%), sepsis in the postoperative period (19 cases; 22.9%), breach of protocol (eight cases; 9.6%), patient request (two cases; 2.4%), and unsuccessful bowel preparation (nine cases; 10.8%). Finally, valid results from 385 patients were analyzed and compared. There were 164 women (42.6%) and 221 men. Surgical site infection was detected in 47 patients (12.5%), including 42 (11.2%) superficial incisional and 5 (1.3%) deep incisional cases. In 188 patients, the triclosan-coated suture (45 right hemicolectomies, 12 left hemicolectomies, seven transversectomies, one cecal resection, three colotomies, 28 A-P resections of the rectum, 28 sigmoid resections, 61 abdominal resections of the rectum, two subtotal colectomies, one total colectomy) were applied. In 197 cases, uncoated sutures (44 right hemicolectomies, 11 left hemicolectomies, five transversectomies, three colotomies, 27 A-P resections of the rectum, 34 sigmoid resections, 68 abdominal resections of the rectum, five subtotal colectomies) were used.
After statistical analysis, in right hemicolectomies, the triclosan-coated suture was significantly inferior to the uncoated one (p=0.006), whereas in resections of the rectum (A-P and abdominal), the coated suture provided significantly (p=0.033) better results. In other types of operations, no significant differences were found (Table 2).
Gram-negative organisms (Pseudomonas aeruginosa, Enterococcos faecium, E. coli, Enterococcus spp.) were isolated from both groups, but gram-positive bacteria (two cases of S. epidermidis) were found only in the uncoated suture group. A total of 23 patients (12.2%) from the triclosan-coated suture group and 24 (12.2%) from the uncoated suture group suffered from SSI, without a statistically significant difference (p=0.982) (Fig. 2). Among all cases of SSI, 13 (27.7%) were diagnosed only after discharge with the distribution of four patients (17.4%) in the triclosan suture group and nine patients (37.5%) in the uncoated suture group. This difference was significant (p=0.041) (Fig. 3).
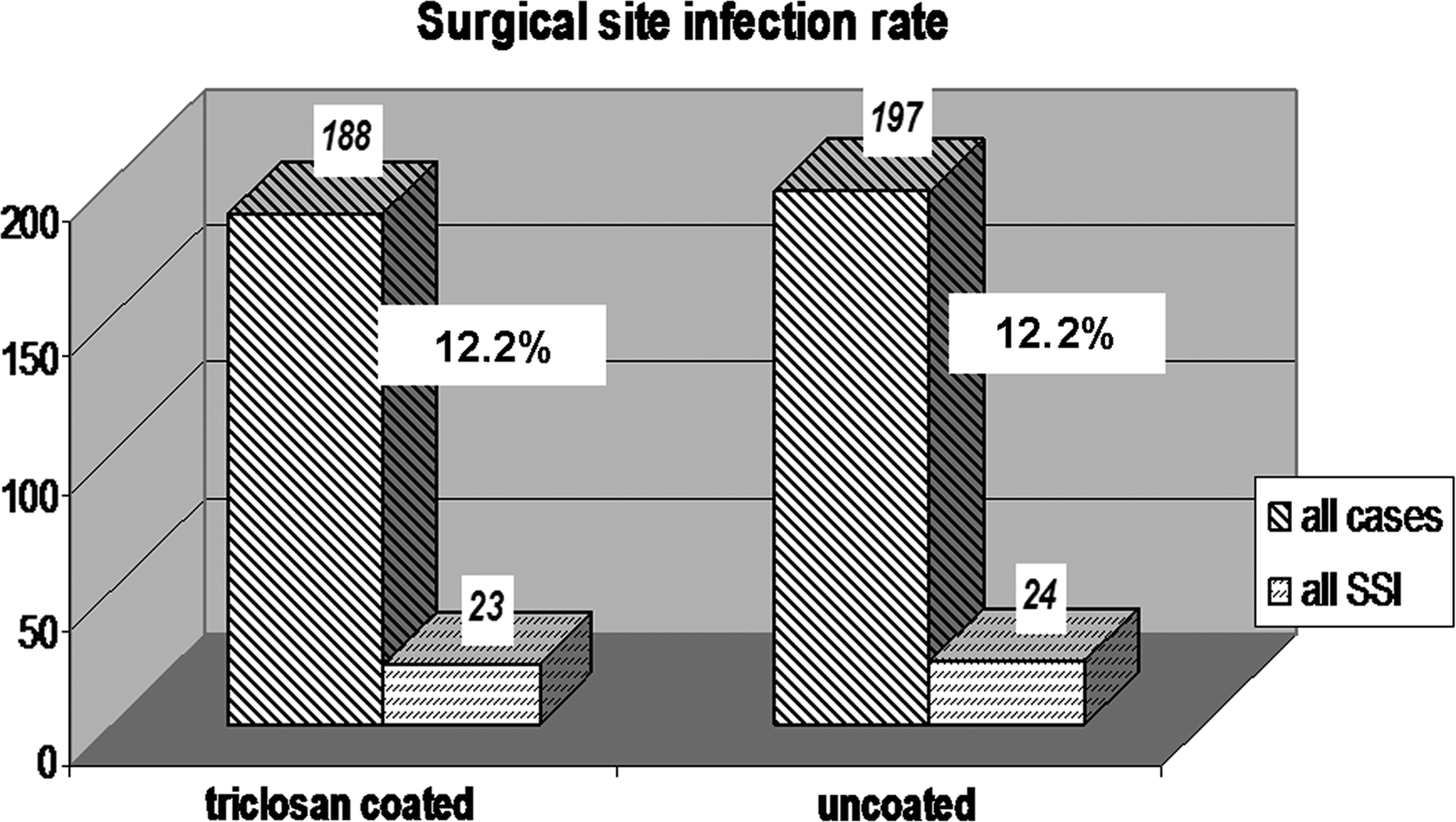
Surgical site infection rate by suture type.
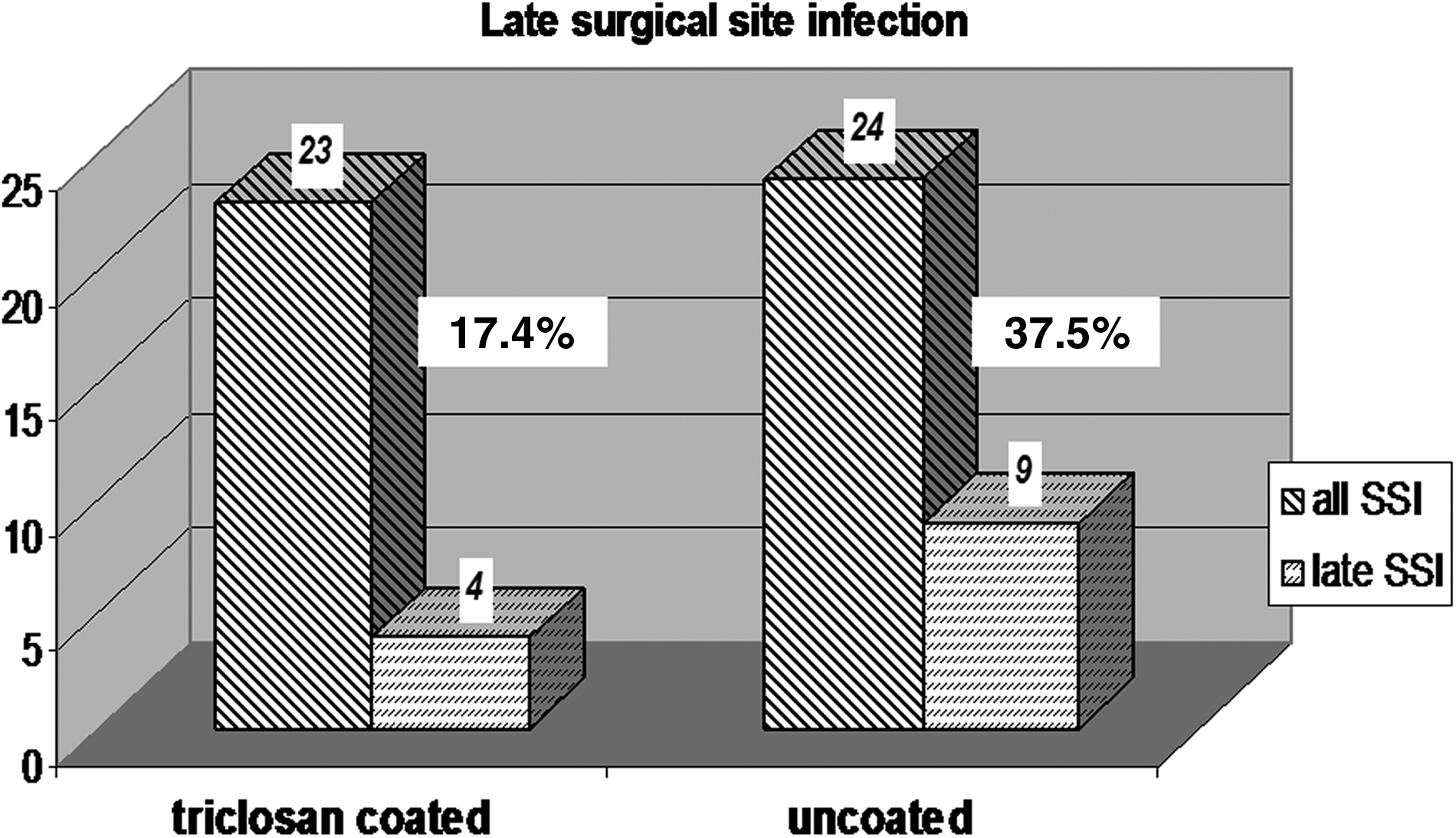
Late surgical site infections by suture type.
Type II diabetes mellitus was found in 31 patients, 16 in the coated (one SSI; 6.3%) and 15 in the uncoated (two SSI; 13.3%) suture group. A series of 43 patients from the triclosan-coated suture group (four [9.3%] with SSI) and 34 from the uncoated suture group (two SSI; 5.9%) had pre-operative chemotherapy or chemo-radiotherapy. In eight cases, fluorouracil–folic acid–oxaliplatin (no SSI) and in a single case, fluorouracil–folic acid–irinotecan (no SSI) therapy was given. Fluorouracil monotherapy was used in 69 cases, and all six SSIs in patients receiving pre-operative chemotherapy were in this group. Two more patients in the coated suture and three more in the uncoated suture group had radiotherapy only. The rest of our patients did not receive neoadjuvant treatment.
We divided the examined population into three groups by BMI. In the undernourished group (BMI<20 kg/m2), the SSI rate was 42.8% (3/7) in the coated suture and 27.3% (3/11) in the uncoated suture group. In the well-fed, normal, and slightly overweight group (BMI 20–30 kg/m2), the SSI rate was 10.9% (16/147) in the coated suture and 11.5% (16/139) in the uncoated suture group. In obese patients (BMI>30 kg/m2), the SSI rate was 11.8% (4/34) in the coated and 10.6% (5/47) in the uncoated suture group.
The cost of SSI and normal wound healing was compared. With normal wound healing, the average number of nursing days was nine, whereas for SSI patients, it was 15 (p=0.043). During the hospital stay, the different types of dressings were recorded, and based on that, a calculation was performed to equilibrate the differences between the various dressings. A unified unit for dressing was determined that would reflect the cost. In this calculation, the least expensive dressing type equaled one unit, and the other types were calibrated according to their cost differential. According to this calculation, 5.2 dressing units were used in cases of normal wound healing in contrast to 32.7 units for SSI (p<0.001). Local lavage was used in almost every case for treating site infections. Because peritoneal and subcutaneous closures were optional and were used in fewer than one-third of the patients, no conclusions could be drawn about their impact on SSI.
Discussion
Surgical site infection is a severe burden on healthcare systems all over the world, increasing surgical morbidity and leading to a greater risk of death and higher healthcare cost. Furthermore, although this point was not examined directly in this study, SSI inevitably influences patient satisfaction and comfort.
Several major factors play roles in the development of SSI [30]. One is the general condition of the patient, including age, fitness (American Society of Anesthesiologists score), and co-morbidities such as obesity, immunosuppression, diabetes mellitus, malnutrition, vascular disease [31–33], anemia [2], and the presence of pathogenic bacteria. A second is local factors such as the lack of pre-operative skin disinfection, lack of antibiotic prophylaxis [34,35], hypoxia and hypothermia [2], contaminated surgical instruments, or the degree of local tissue necrosis induced by retractor use during surgery [36]. Another factor is infectious: Nosocomial infections acquired secondary to prolonged hospital stays, intra-operative bacterial colonization and toxin secretion, or bacterial capsule formation in the wound. Another non-trivial factor is technical: Routines of surgeons, length of operations [35], technique of abdominal wall closure, and the suture material used. This study aimed to examine part of the last two of these factors.
Surgical site infection develops more often after colorectal than after other clean-contaminated operations [2]. Our retrospective study showed that in Hungary, the rate of SSI after colorectal surgery was nearly 30%. In our department, this value was 25%. The technique of abdominal wall closure is not uniform in our country. Some surgical departments used non-absorbable suture material, some use interrupted sutures, and interspersed interrupted sutures were applied in some centers. Therefore, a new multi-center randomized trial was planned to create a national uniform abdominal closure technique for colorectal surgery. To comply with the latest findings, absorbable running monofilament suture was chosen for closing the abdominal fascia and atraumatic stitches for the skin. Closure of the peritoneum and subcutaneous layer was not obligatory. A few months before the start of our study, a new antiseptic solution (triclosan)-covered surgical suture became available in the Hungarian market. This was the first antiseptic-coated, absorbable suture on the Hungarian market that had sufficient tensile strength for abdominal wall closure. Positive evaluations by different international studies encouraged the induction of this multicenter prospective clinical trial [15,22]. The first studies analyzed the in vitro effects of triclosan [13,23]; later, some studies with animal models [18,19,34,36] and then clinical trials [17,32,39] appeared that confirmed the efficacy of triclosan-coated suture.
In the present study, triclosan-coated and -uncoated polydiaxanone sutures were compared in 385 patients undergoing colorectal surgery. The two groups (triclosan-coated and -uncoated polydioxanone sutures) showed homogeneity in demographic features (see Table 1). There were no significant differences in SSI in the two groups. The rate of SSI was nearly equal in percentage (∼10%). On the other hand, compared with the former retrospective study by this department, the SSI rate was reduced by 50%. This was the main result of this randomized trial, but there was not as high a difference between the two groups as in the pilot study. This could mean that the antibacterial effect of triclosan-coated polyglactin 910 suture provided much better results than the coated polydiaxanone in preventing SSI, as was shown also by the University of Saarland [15]. This might be because the polyglactin 910 is braided, whereas polydiaxanone is a monofilament.
NS=not significant; SSI=surgical site infection.
NS=not significant; SSI=surgical site infection.
The SSI rate also was compared after colon and after rectal surgery without any significant difference, in contrast to reports showing double the rate of SSI with uncoated suture after rectal operations [27,32]. On the other hand, our data showed two-fold greater SSI rates in the triclosan-coated suture group after right hemicolectomy. Data also indicated a significant difference in rectal operations, with triclosan-coated suture being superior. The reason a significant difference was found only in two types of operations could not be determined. The explanation could have been the location of the incisions (subcostal, midline), which were not standardized, so further studies are needed to verify these results.
The microbiological examinations, as the literature, indicates, showed that the triclosan-coated suture inhibits the growth of gram-positive bacteria. In vitro studies demonstrate that triclosan produces a larger inhibition zone among gram-positive bacteria than in cases of gram-negative bacilli and specifically Klebsiella strains, which appear in great numbers in colon cultures [34]. We have only two cases supporting this finding, and we cannot draw the same conclusion as did previous studies. Earlier research suggested that triclosan-coated sutures have greater advantages in clean operations, such as orthopedic, plastic, and cardiac surgery, as has been proved [15]. According to our study, triclosan has no real effect against the gram-negative bacteria from the colon.
The literature documents some factors that create a high risk of SSI, including frequent glove changes, surgical aggressiveness, diabetes mellitus, high BMI, and neoadjuvant chemotherapy or radiotherapy [1,3,4,6,30]. Type II diabetes mellitus was found in 31 patients, 16 in the coated suture (one SSI; 6.3%) and 15 in the uncoated suture (two SSI; 13.3%) group. These data suggest a difference in SSI rates; however, because of the small number of patients, we cannot draw this conclusion. A total of 43 patients from the triclosan-coated suture group (four SSI; 9.3%) and 34 from the uncoated suture group (two SSI; 5.9%) had pre-operative chemotherapy or chemo-radiotherapy. Radiotherapy was applied only in rectal cancers and did not affect abdominal wall healing. Just as in the case of diabetes mellitus, more cases will be needed to draw any conclusion regarding this point.
Some papers report higher SSI rates in overweight and obese patients [1,2,4]. These papers also report a higher risk of site infection in the under-fed population (BMI<20 kg/m2). We could not confirm in this study that obesity (BMI>30 kg/m2) had an adverse effect compared with the normal weight and slightly overweight group (BMI 20–30 kg/m2). On the other hand, SSI was twice as common in the undernourished (both coated and uncoated suture) groups as in the group with a normal BMI (11.2% in normal BMI and 33.3% in BMI<20 kg/m2; p<0.05).
An interesting observation is that there are many late SSIs after colorectal operations: SSI presenting after hospital discharge accounts for roughly 50% of such infections [29]. In this study, late SSI was less common overall (17.4% vs. 37.5%) but significantly more common in the uncoated suture group than in the triclosan-coated suture group (Fig. 3). This may confirm the inhibiting effect of triclosan for bacterial colonization of the immediate surroundings of the suture material.
Several investigators doubt the necessity of bowel preparation before colorectal operations [35]. The data show that in some cases, bowel preparation makes the site infection rate higher because the liquid bowel contents cause a higher infective risk than solid feces. That is why several authors recommend the omission of pre-operative bowel preparation [35]. In Hungary, more than 50% of colorectal surgery patients have obstipation and present rarely in the early stages of bowel obstruction because of the lack of screening. This is why bowel preparation was advocated and used. In nine cases, the reason for exclusion was the ineffective bowel preparation, resulting in a large volume of feces above the colon stricture.
The time of hospitalization was significantly longer in cases of SSI. The mean hospital stay with normal wound healing was nine days, whereas in cases of SSI, it was 15 days. These extra days produced a much higher cost for the Hungarian national healthcare system. Moreover, about six times more dressing units were used when SSI developed and wound discharge was present (p<0.001).
According to the literature, the duration of the operation influences the development of SSIs [2,26,30,33]. Concerning SSI, the most important part of the surgical procedure is when the colon is open and able to contaminate the surrounding tissues. Another factor that can influence the SSI rate is the experience of the surgeon. Only surgeons who perform more than ten colorectal operations annually were involved in this study.
In this clinical trial, compared with the former retrospective study, the rate of SSI was reduced by one-half. This can be attributed to the surgical suture material, the exact time of antibiotic prophylaxis, frequent patient monitoring, use of disposable drapes, careful surgical techniques, and, (last but not least) the fact that in all cases, the abdominal fascia was closed by an experienced surgeon, not by residents in training.
Summarizing the data, it can be stated that abdominal wall closure with looped polydiaxenone, independently of whether it is coated or uncoated, decreases the SSI rate. Triclosan protects against gram-positive bacteria [34], which probably originate from the skin, but this cannot be confirmed by our study results because of the small number of cases. It seems that triclosan may not be effective against gram-negative colonic bacteria, because it was not associated with a lower SSI risk than was seen in the control group. Treatment of SSI significantly increases cost. With the prevention of SSI, the cost can be reduced significantly and patient satisfaction probably is greater, but truly effective methods of SSI prevention and multifactorial patient satisfaction reports still are needed.
Footnotes
Acknowledgments
We are beholden to the surgeons of the seven involved centers: the University of Debrecen (head, Doctor L. Damjanovich; local coordinator, Doctor R. Kotán); University of Szeged (Doctor G. Lázár; local coordinators Doctors E. Mán and G. Baradnai); Aladár Petz County Hospital, Győr (head, Doctor A. Oláh; local coordinator, Doctor Z. Benedek-Tóth); András Jósa County Hospital, Nyiregyháza (head, Doctor S. Bogdán; local coordinator, Doctor P. Zemanek); Mór Kaposi County Hospital, Kaposvar (head, Doctor T. Oláh; local coordinator, Doctor K. Somodi); County Hospital, Kecskemet (head, Doctor M. Svébis; local coordinator, Doctor J. Molnár); University of Pécs (head and study principal investigator, Doctor Ö.P. Horváth; local coordinator, Doctor O. Huszár; study coordinator, Doctor J. Baracs).
Author Disclosure Statement
No conflicting financial interests exist.