
Abstract
Abstract
Background:
Nocardia farcinica is a gram-positive, partially acid-fast, methenamine silver-positive aerobic actinomycete. Nocardia spp. are opportunistic pathogens, and N. farcinica is the least common species of clinical importance.
Methods:
Review of the recent literature and description of a immunocompetent patient with no known risk factors who contracted fatal N. farcinica sepsis.
Results:
Positive pre-mortem and post-mortem cultures from the lung and synovium correlated with acute bronchopneumonia and synovitis at autopsy. Colonies of filamentous bacteria, which were not apparent in conventional hematoxylin and eosin-stained sections, were observed with gram and methenamine silver stains, but acid-fast stains were negative. A literature review revealed that disseminated N. farcinica often is associated with an underlying malignant tumor or autoimmune disease (88% of patients). Chemotherapy or corticosteroid treatments are additional risk factors.
Conclusions:
Trimethoprim–sulfamethoxazole typically is the first-line therapy for N. farcinica; treatment with amikacin and imipenem-cilastatin is used less often (7% of patients). Despite aggressive therapy, we observed that the death rate (39%) associated with N. farcinica in recent publications was eight percentage points higher than reported in a review from 2000.
Case Report
A 78-year old male presented with a one-day history of right knee pain and swelling. The patient had received a steroid injection in the same knee one week before admission. Three years prior to admission, the patient had an unexplained illness consisting of one month of fever (100.3°F), a 19-pound weight loss, and an elevated white blood cell count (15,300/mm3). At that time, he also had an infected cyst in the posterior scalp, which was treated with cephalexin but was not cultured. The full extent of clinical evaluation at that time is unknown.
On admission, laboratory evaluation revealed hemoglobin 13.4 g/dL, hematocrit 40.1%, white blood cell count 23,300/mm3, and platelets 435,000/mm3. Pertinent chemistry findings were blood urea nitrogen 74 mg/dL, creatinine 2.6 mg/dL, and glucose 151 mg/dL. Cultures from six knee synovial fluid aspirations and peripheral blood grew N. farcinica susceptible to ciprofloxacin (minimum inhibitory concentration [MIC] 1 mcg/mL), linezolid (2 mcg/mL), amikacin (2 mcg/mL), and sulfamethoxazole (4 mcg/mL). A computed tomography (CT) scan revealed numerous subcentimeter non-calcific pulmonary nodules (Fig. 1). The patient was treated with intravenous trimethoprim–sulfamethoxazole (TMP-SMX). The patient's renal function improved with hydration. Eleven days after admission, the patient developed tachypnea and respiratory distress acutely and died.
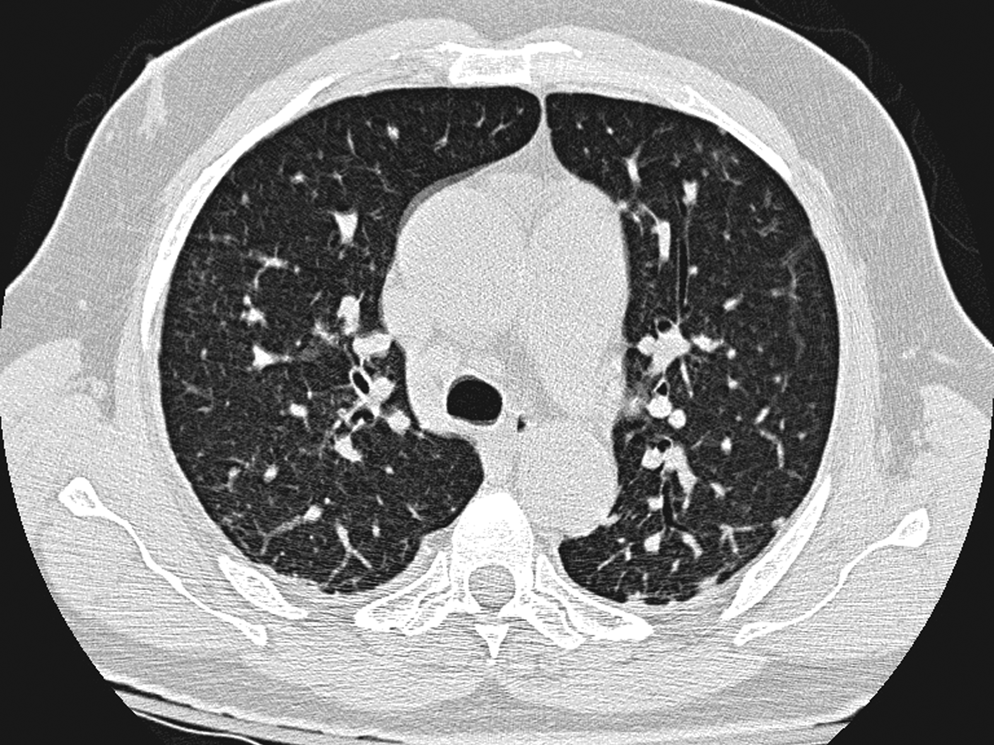
Chest CT scan demonstrates multiple subcentimeter nodules in both lungs.
Autopsy findings included bilateral serosanguinous pleural effusions (200–300 mL) and copious turbid, greenish fluid in the right knee. Histologically, there was acute suppurative and chronic synovitis (Fig. 2A). In both lungs, extensive organizing, nodular, intra-alveolar pneumonia (Fig. 2B, C) with abscesses and associated miliary granulomas (Fig. 2D) were observed. Cultures of both lungs and the synovial fluid were positive for N. farcinica. Gram-positive, methenamine silver-positive, beaded, branching, filamentous bacteria were identified in both locations. Although acid-fast stains were negative, N. farcinica was identified by polymerase chain reaction amplification and sequencing of the bacterial rRNA.
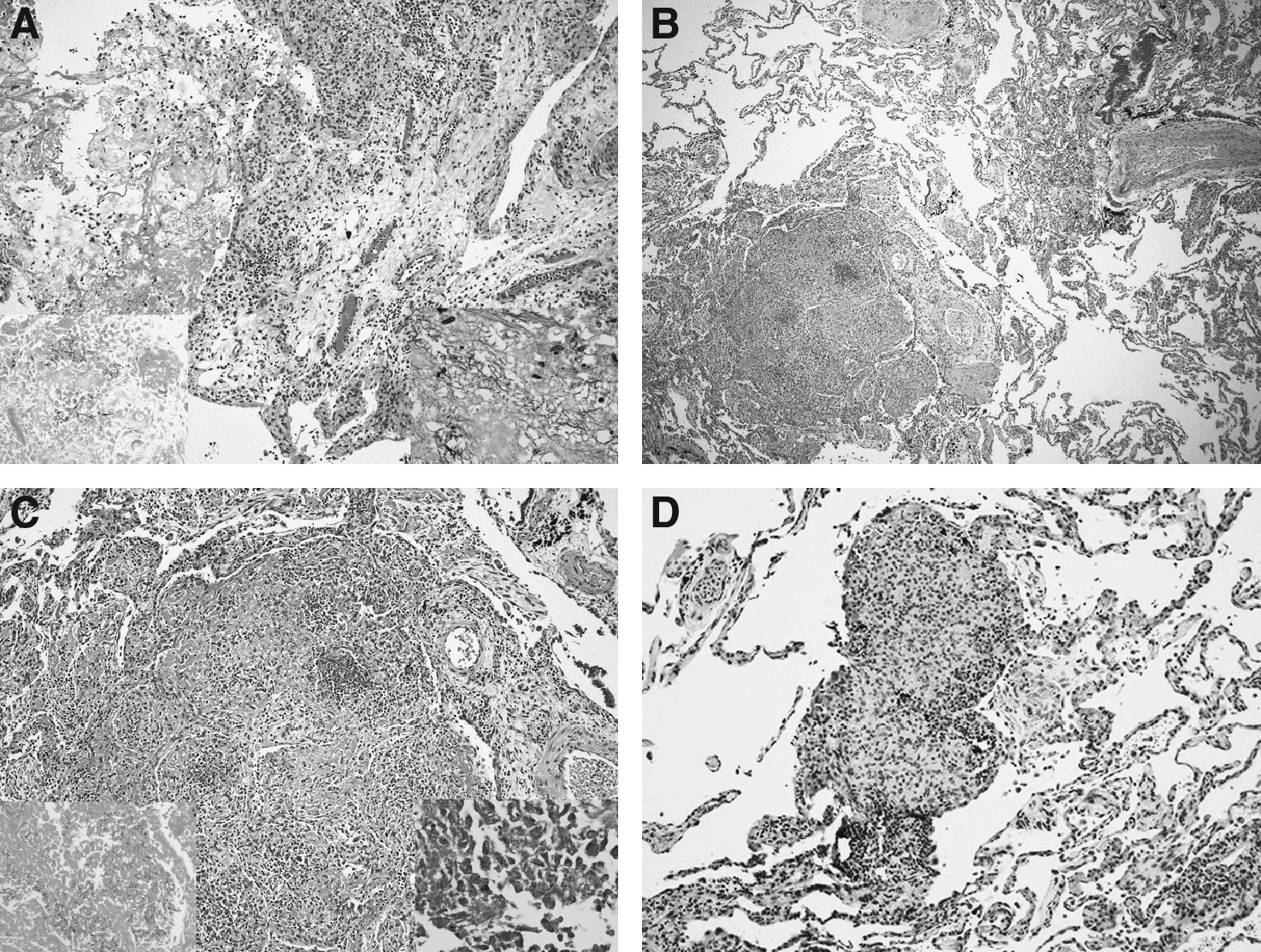
Histologic views. (
Discussion
A relatively infrequent cause of nocardiosis, N. farcinica is a clinically aggressive infection, particularly in immunocompromised patients. For unknown reasons, small numbers of immunocompetent patients also are affected. In the last review of N. farcinica sepsis by Torres et al. in 2000, a retrospective analysis of 53 patients identified eight cases (15%) in which no predisposing factors for infection were discernible [13]. Of the eight patients, one presented with a brain abscess [14] and two had lung or kidney involvement or both [15,16]. Similarly, Beaman et al. reported that 15% of patients infected with Nocardia had no identifiable underlying condition [4]. In most cases, the pathogenesis of Nocardia infection is presumed to be via an airborne route from soil inhabited by latent forms. Following colonization of the respiratory tract, T lymphocyte-mediated cellular immunity is activated after phagocytosis of the organism
Our search of the literature for cases of N. farcinica published since the last review [14] demonstrates the continued rare occurrence of N. farcinica infection in immunocompetent patients [17]. Of the 67 cases reported since 2000, 59 (88%) patients suffered from a predisposing illness or had risk factors associated with diminished immunocompetence (Table 1). Of the eight immunocompetent patients in this cohort, six presented with brain abscesses and two with disseminated disease. Previous reports indicate that Nocardia spp. were responsible for 2%–20% of cerebral abscesses in immunocompromised patients [18,19], with a mortality rate of 30%–80% [14,20].
Plus cyclophosphamide.
Co-infection with cytomegalovirus and Pneumocystis jirovecii.
Co-infection with Pseudomonas aeruginosa.
Plus tacrolimus.
Plus cyclosporine.
Co-infection of lungs with P. aeruginosa, and Escherichia coli.
Plus azathioprine.
Patients were treated with chemotherapy and immunotherapy for cancer.
Microphenolate+tacrolimus immunosuppression.
ABPA=allergic bronchopulmonary aspergillosis; AMK=amikacin; AMP/SULB=ampicillin/sulbactam; AMX/CLAV=amoxicillin/clavulanic acid; BAL=bronchoalveolar lavage; BOOP=bronchiolitis obliterans organizing pneumonia; CF=cystic fibrosis; CFP=cefozopran; CFZ=ceftazidime; CLL=chronic lymphocytic leukemia; CPX=ciprofloxacin; COPD=chronic obstructive pulmonary disease; CTR=ceftriaxone; CTX=cefotaxime; CTZ=ceftazidine; CXN=cloxacillin; DXN=dicloxacillin; DM=diabetes mellitus; ESRD=end-stage renal disease; GEN=gentamicin; HCV=hepatitis C virus; HIV=human immunodeficiency virus; IMI=imipenem-cilastatin; IND=indomethacin; IPF=idiopathic pulmonary fibrosis; ITC=itraconazole; ITP=idiopathic thrombocytopenic purpura; IV=intravenous; LIN=linezolid; LVX=levofloxacin; MAC=Mycobacterium avium complex; MER=meropenem; MET=metronidazole; MIN=minocycline; MOX=moxifloxacin; NHL=non-Hodgkin lymphoma; NR=not reported; PO=orally; SLE=systemic lupus erythematosus; SUF=sulfadiazine; TEI=teicoplanin; TMP-SMX=trimethoprim–sulfamethoxazone; VAN=vancomycin.
In agreement with previously published reports [13], the ratio of male:female infection was 3:1. Although typically responsible for infections in adults, N. farcinica also infected a 12-year-old adolescent following renal transplant [21], an 8-year-old boy with cystic fibrosis [22], and an otherwise-healthy 2-month-old boy [23]. Our review of the literature demonstrated that 10.4% of patients receiving TMP-SMX prophylaxis became infected. Nocardia infection also is reported in 60% of lung transplant recipients [19,24]. Furthermore, most of the patients (61.2%) infected with N. farcinica were receiving systemic steroids or chemotherapy. Corticosteroid treatment inhibits the cytokine response and phagocytic killing of microbes by macrophages [25].
Table 2 summarizes the co-morbidity factors most commonly associated with infection for the cases in Table 1. Hui et al. [26] reported that 63% of pulmonary nocardiosis patients had underlying respiratory disorders. In particular, COPD was identified as a risk factor in 23% of patients with pulmonary nocardiosis [27]. Nocardia infection is reported in as many as 3% of transplant recipients [7] with an associated mortality rate ranging from 0% to 75% in lung transplant recipients [19,28]. Alcoholism (3.0%), hematologic malignancy (4.5%), HIV infection (7.5%), idiopathic thrombocytopenic purpura (ITP) (3.0%), systemic lupus erythematosus (SLE)(4.5%), neoplastic disease (7.5%), diabetes mellitus (9.0%), and vasculitis (4.5%) were co-morbid conditions identified in at least two patients.
Some patients presented with more than one factor.
One case each of invasive aspergillosis, Mycobacterium avium complex, drug abuse, pneumoconiosis, Evans syndrome, bullous pemphigoid, interstitial pneumonia, ulcerative colitis, bronchiolitis obliterans organizing pneumonia, idiopathic pulmonary fibrosis, polymyalgia rheumatica, cystic fibrosis, allergic bronchopulmonary aspergillosis, cirrhosis, sarcoidosis, trauma, and chronic bronchitis.
Disseminated nocardiosis is associated with a mortality rate ranging from 7% to 85% in immunocompromised hosts [29]. Disseminated disease and bacteremia occurred in 37% of the cases reported since 2000 (Table 3). Assuming that patients with central nervous system lesions also had a lung infection that was unrecognized [13], 39 patients (58%) had disseminated disease. Soft tissue infection involving muscles or connective tissue, including subcutaneous abscesses, was present in 17.9% of the cases. Torres et al. [13] reported a mortality rate of 31% in cases diagnosed before 2000; the mortality rate in the cases reported since then was 39%.
“Disseminated” includes bacteremia or more than one organ involved.
The diagnosis rests on the demonstration of organisms in tissue, cultures, or both. Histologically, organisms are difficult to recognize by hematoxylin and eosin stains. Also, as demonstrated here, acid-fast staining is variable and unreliable [1, 13]. Gram and methenamine silver (GMS) stains usually are positive, although gram staining may be weak. Cultures of Nocardia can take more than five days to grow [30]. Biochemical tests may be used for identification of a subset of Nocardia spp., but 16S rRNA gene sequencing or restriction analysis of amplified DNA (16S rRNA or hsp65 genes) allows rapid identification [31, 32]. This is significant, as it is important to distinguish N. farcinica from N. asteroides—the former is more resistant to antimicrobial agents and has a higher risk of dissemination [33]. The treatment for N. farcinica is complicated by its resistance to most β-lactam anti-microbials, tobramycin, and tetracyclines [12, 34]. The treatment of choice is TMP-SMX [35]. However, side effects such as skin reactions may necessitate alternative therapy [6,24,36]. In addition, as many as 50% of isolates demonstrate TMP-SMX resistance, emphasizing the need for antibiotic susceptibility testing of clinical isolates [13,37,38].
N. farcinica is susceptible to TMP-SMX, minocycline, linezolid, moxifloxacin, and amikacin and demonstrates variable susceptible to imipenem-cilastatin and ciprofloxacin [20, 39–43]. It is recommended that immunocompetent patients be treated for at least six months [44]. If the central nervous system is involved, 12 months of therapy is recommended [44]. Therapy for N. farcinica has become more aggressive, with increasing administration of multiple antimicrobials. In this review, 74.6% of patients (n=50) received TMP-SMX as part of their treatment. Carbapenems (n=25; 37.3%), amikacin (n=16; 23.9%), and ceftriaxone (n=12; 17.9%) also were used commonly (see Table 1). A previous review found TMP-SMX was administered in 54% of patients infected with N. farcinica, whereas amikacin with imipenem-cilastatin and amoxicillin/clavulanic acid were used in only 7% [13]. Nevertheless, the death rate was 31% with TMP-SMX and 38.8% with carbapenems and amikacin [13].
The patient described here was unusual in that he was immunocompetent. Although the primary origin of his infection is not documented, it is tempting to speculate that the prior febrile episode and infected cyst of three years earlier was his initial encounter with the organism. Subsequent reactivation with dissemination may have been prompted by unknown factors and perhaps facilitated by the local steroid injection. The distribution of his infection was pulmonary and musculoskeletal (limited to the right knee) with no radiologic or post-mortem evidence of central nervous system involvement. Despite therapy, the patient died from Nocardia sepsis, attesting to the virulence N. farcinica.
Footnotes
Acknowledgments
JMB is a trainee of the National Institutes of Health Medical Scientist Training Program (Grant GM07281) at the University of Chicago.
Author Disclosure Statement
No conflicting financial interests exist.