
Abstract
Abstract
Background:
Hyperglycemia is common in surgical patients and is associated with adverse outcomes. Conflicting data exist regarding the best method and the value of glycemic control in various patient populations. The contributions to hyperglycemia and the components of its control are complex and overlapping and likely contribute to the documented variation in outcomes. We provide an overview of the physiologic contributors to hyperglycemia and its control, review the differences in the major randomized trial results, and summarize the data regarding glycemic control in surgical patients.
Methods:
Major reviews of the pathophysiology of hyperglycemia in surgical patients, large randomized trials in critically ill and peri-operative populations, and meta-analyses were reviewed. Summations are provided for the critically ill population and for the peri-operative group.
Results:
A substantial physiologic rationale exists for the control of hyperglycemia in surgical patients during critical illness and in the peri-operative period. Randomized, controlled studies are limited predominately to critically ill populations. The data support controlling hyperglycemia to a serum glucose concentration <200 mg/dL, but the absolute target range remains controversial and studied inadequately. The data indicate the benefit of tight glycemic control using insulin to achieve a target of 80–110 mg/dL (intensive insulin therapy [IIT]) vs. a liberal target of 180–200 mg/dL in critically ill surgical patients, although hypoglycemia is more common with IIT. Inadequate studies are available in the peri-operative period to draw conclusions about non-critically ill surgical patients, but the weight of the data suggests control to <200 mg/dL likely is beneficial.
Conclusions:
Surgical patients benefit from maintaining serum glucose concentrations <200 mg/dL. Intensive insulin therapy (80–110 mg/dL), which appears beneficial in critically ill surgical patients but requires frequent measurement of glucose to avoid hypoglycemia. Further studies are needed to determine the appropriate target range and the influence of nutritional provision and other factors on outcome.
Incidence of Hyperglycemia in Surgical and Acutely Ill Patients
The majority of patients undergoing major surgical, traumatic, thermal, or sepsis-related stress develop what is termed “stress hyperglycemia” [2–5]. Hyperglycemia has been defined in several large trials as having a cut point of either 180 mg/dL (10 mmol/L) [6,7] or >200 mg/dL (11.1 mmol/L) [1,8–10] but is defined as >140 mg/dL (7.8 mmol/L) by the American Association of Clinical Endocrinologists and the American Diabetes Association [11]. Critically ill patients in particular have a high incidence of hyperglycemia. In one prospective observational study, 90% of critically ill medical and surgical patients either developed hyperglycemia or required insulin to control the serum glucose concentration during the course of their intensive care unit (ICU) stay [12]. The degree of hyperglycemia is proportional to the magnitude of the stress response (e.g., the extent of the surgery, injury severity) and is strongly associated with poor outcomes in patients both with and without diabetes mellitus; however, this relation is stronger in non-diabetic patients [2]. In one study of 1,886 unselected hospitalized patients, the risk of death was 2.7 times greater for diabetic patients and 18.3 times greater for non-diabetic patients who had hyperglycemia vs. those who did not when adjusted for age, body mass index, gender, hypertension, coronary artery disease, infection, renal failure, and ICU admission [13].
Similar associations between hyperglycemia and outcomes have been demonstrated in both diabetic cardiac surgery and critically ill patients. A single blood glucose value >200 mg/dL after cardiac surgery was associated with a doubling of the post-operative infection rate [14]. Furnary et al. demonstrated an increase in both cardiac-related and non-cardiac-related deaths in patients with diabetes mellitus undergoing coronary artery bypass grafting as glucose concentrations increased above 150 mg/dL, from approximately 1% to >14% in patients whose blood glucose value was >250 mg/dL [15]. In a study of nearly 5,000 ICU patients, Egi et al. demonstrated that hyperglycemia was strongly and independently associated with death in non-diabetic patients, with odds ratios (ORs) for death increasing from 1.74 for patients with glucose in the 140–180 mg/dL range to 3.85 for patients with glucose concentrations >200 mg/dL [16]. However, no significant association with death could be demonstrated in patients with diabetes mellitus.
Other surgical populations have provided similar results. In trauma patients, elevated glucose concentrations are associated with death [17–19]. In one study of acutely injured patients, a single episode of hyperglycemia >150 mg/dL was linked to a two-fold increase in the mortality rate when adjusted for age, Glasgow Coma Scale score, ventilator days, and admission serum lactate concentration [20]. Glucose elevation both pre-operatively and post-operatively in elective surgery has been associated with infectious and non-infectious morbidity. Glucose elevations are a strong risk factor for post-operative complications in gastric bypass patients [21] and vascular patients [22]. In a retrospective study of non-critically ill orthopedic patients, Richards et al. demonstrated a greater than three-fold increase (OR 3.3) in the risk of surgical site infection (SSI) for patients with two or more glucose values >200 mg/dL or a hyperglycemic Index of ≥1.76 during their hospitalization [23]. In critically ill or injured surgical patients, acute changes in insulin requirements to maintain normoglycemia or acute glucose elevation while on a glycemic control protocol are highly predictive of subsequent infection [21,24–27]. Thus, hyperglycemia is both common and strongly associated with morbidity and death in a variety of surgical populations.
Etiology of Hyperglycemia after Stress
Numerous factors may contribute to a patient's development of hyperglycemia during illness, including established diabetes mellitus (either type 1 or type 2), therapeutic interventions such as nutritional support, exogenous steroids, vasopressors, and the patient's response to the illness itself [2]. Several aspects of the human stress response contribute to hyperglycemia, including activation of the hypothalamic/pituitary/adrenal axis, catecholamine release, and the inflammatory cytokines that result in lipolysis, glycogenolysis and gluconeogenesis by the liver insulin resistance (IR) and decreased glucose uptake and clearance by skeletal muscle [3–5,28,29]. Figure 1 outlines stress-related hyperglycemia and insulin resistance (IR) that occur as a result of surgery, infection, or injury. During the early phases of the stress response, epinephrine, glucagon, and cortisol appear to act synergistically to contribute to hyperglycemia [30], and glucose production by the liver appears to contribute to hyperglycemia through pathways involving increased hepatic gluconeogenesis via hepatic glycogenolysis, lipolysis, and cycling of alanine and glutamine from skeletal muscle proteolysis [29,31]. However, although these changes all contribute to hyperglycemia acutely, changes in glucose homeostasis persist long after corticosteroids, catecholamines, and cytokines have returned to normal concentrations [3,12].
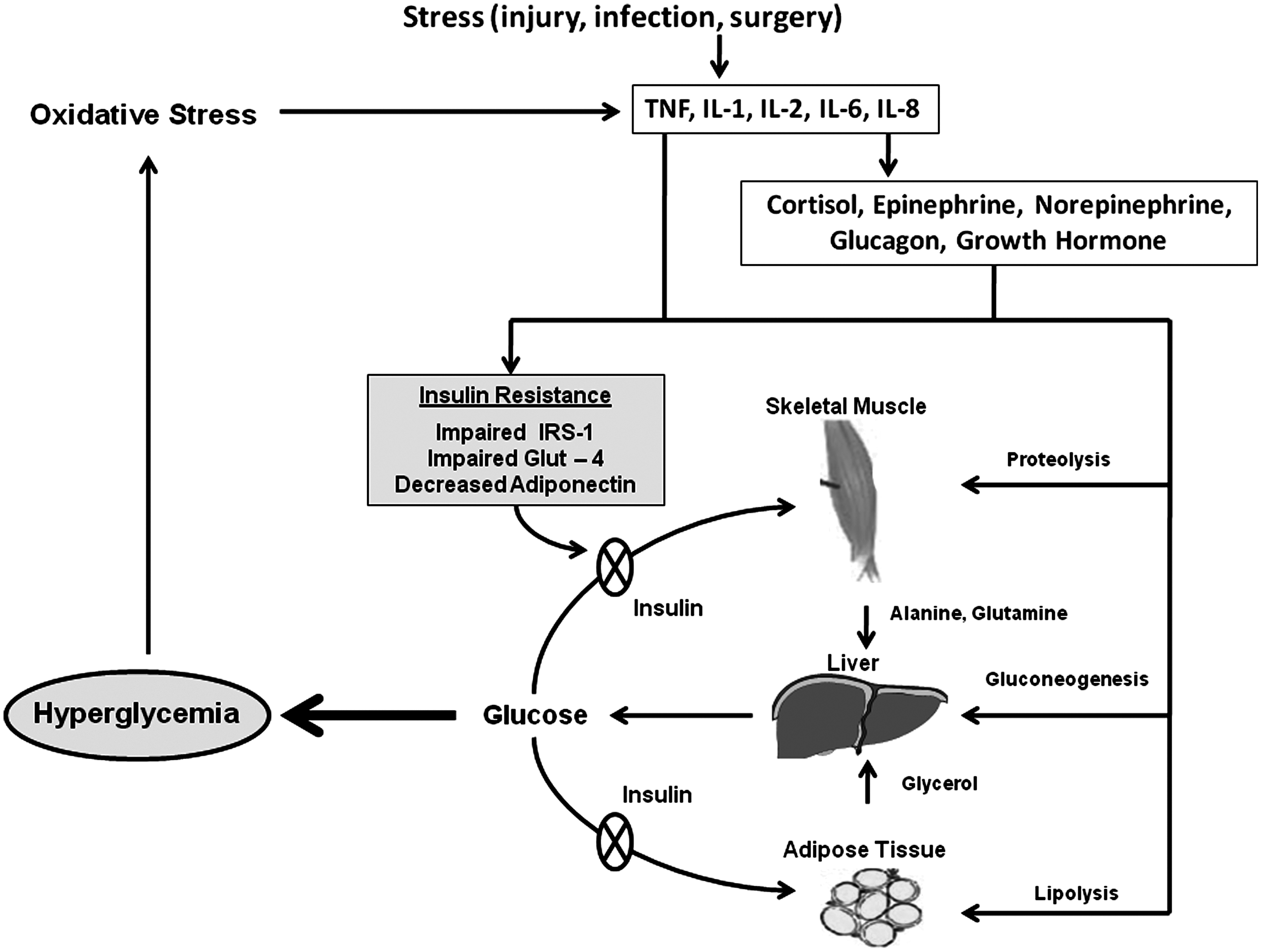
Model of stress-induced insulin resistance and hyperglycemia. GLUT=glucose transporter; IL=interleukin; IRS=insulin receptor substrate; TNF=tumor necrosis factor.
The development of this prolonged period of stress hyperglycemia is related predominately to IR that develops during and persists after stress, promoted at least in part by the elevation of hormones and pro-inflammatory cytokines soon after stress [29]. Insulin resistance is defined as a decrease in the biologic response to insulin relative to normal, thus resulting in hyperglycemia [3,28]. The degree of IR differs among healthy individuals. Within a single individual, IR demonstrates diurnal variation and is increased substantially by fasting [3]. The increase in IR associated with illness and stress is caused in part by altered uptake and clearance of glucose by skeletal muscle secondary to post-receptor insulin signaling alterations induced by phosphorylation of insulin receptor substrate (IRS)-1 [32,33] and downregulation of the glucose transporter (GLUT)-4 receptor [3,4,28]. After uncomplicated elective surgery, IR increases in a dose-dependent manner corresponding to the magnitude of the surgical stress. For example, after elective open cholecystectomy, IR shows a 50% increase that persists for two to three weeks [4,34]. This period of IR mirrors the catabolic state and net nitrogen loss that persists for weeks after major burns, trauma, and sepsis [35]. Critical illness produces dramatic changes in IR. In a study of 925 critically ill surgical patients, the degree of IR (assessed as the insulin dose required to maintain euglycemia) expressed by individual patients differed by an average of 11-fold across their ICU stay and by 42-fold across the entire study population [36]. Additionally, the degree of IR correlates with death in critically ill surgical and trauma patients, independent of glycemic control [18,36–38].
Alteration of Insulin Resistance
Several lines of research suggest that the degree of IR that follows stress may be alterable by numerous variables. For instance, fasting not only increases IR but also enhances the IR induced by surgical stress [3,4]. On the other hand, the provision of glucose, rather than fasting, with maintenance of a normal serum glucose concentration with insulin appears to abrogate this response and may be associated with better outcomes after elective surgery [3,4,39]. Data also suggest that the control of elevated serum glucose with insulin in critically ill patients reduces increases in IR during the period of illness [40–42].
Glutamine administered parenterally appears to reduce stress-induced IR in critically ill and injured humans [43,44], as well as in animal models [45,46]. The protein adiponectin, which decreases significantly during critical illness, alters IR directly through its activation of several intracellular signaling pathways that increase glucose utilization, glucose uptake by muscle, and hepatic gluconeogenesis [47–49]. Adiponectin decreases phosphorylation of the IRS-1 subunit, which is involved in post-receptor insulin signalling and is linked to IR after stress [50]. The ability to alter IR may be clinically important, as changes in IR may be associated with alterations in the mortality rate, independent of glycemic control [18,36–38].
Basic Science Rationale for Glycemic Control
The theoretical benefits of glycemic control during critical illness and the peri-operative period include both the adverse effects of hyperglycemia and the positive effects on insulin in these settings. The negative effects of hyperglycemia may be grouped into those related to cellular and organ injury and those related to immunocompetence and infection.
Cellular and organ injury
Hyperglycemia contributes directly to oxidative stress at the cellular level and promotes activation of both classic and acute-phase intracellular signaling pathways [2]. Hyperglycemia is associated with endothelial dysfunction, proinflammatory cytokine production, platelet activation, mitochondrial dysfunction, immune dysregulation, procoagulant activity, catabolism, lipo-toxicity, extracellular matrix deposition, and sympathetic nervous system activation. Both the magnitude and the duration of hyperglycemia appear to affect these physiologic changes. Accumulation of these changes thus may contribute significantly to the end-organ dysfunction observed after surgical stress and critical illness.
Immunocompetence and infection
Acute elevations in glucose are strongly pro-inflammatory and alter neutrophil and antigen-presenting functions significantly [11,51–55]. There is considerable in vitro and in vivo evidence that acute hyperglycemia impairs immune function by several mechanisms, including alteration of neutrophil activity, degranulation, and phagocytosis; expression of cellular adhesion molecules; promotion of neutrophilic adherence and sequestration in peripheral tissues; generation of reactive oxidant species; stimulation of cytokine production; and alteration in vascular tone [54–66]. These changes lead to inability of the host to control pathogens and a higher peri-operative infection rate. As noted above, both the magnitude and the duration of glucose elevation appear to contribute to these physiologic changes. Reversal of hyperglycemia with insulin partially or completely prevents or reverses these hyperglycemic effects.
Insulin effects
The positive effects of insulin during stress include both metabolic and immunologic/inflammatory modulation [28,67]. The key metabolic effects are changes in carbohydrate, lipid, and protein metabolism. Insulin causes increased uptake of glucose into skeletal muscle and adipose tissue, greater glucose storage as glycogen, decreased glycogenolysis, and reduced gluconeogenesis by the liver. Insulin also affects lipid metabolism via increased conversion of glucose to free fatty acids and triglycerides in the liver and adipocytes, reduced lipolysis, and reduced ketone production by the liver. Finally, insulin alters protein metabolism by increasing the uptake of amino acids by skeletal muscle and liver and by reducing protein breakdown. The key immunologic/inflammatory effects of insulin during stress include reduced production of pro-inflammatory cytokines such as interleukin [IL]-1, IL-6, macrophage migration inhibitor factor [MIF], tumor necrosis factor [TNF], high mobility-group protein box [HMGB]-1, monocyte chemoattractant protein [MCP]-1; enhanced anti-inflammatory cytokine production (including IL-2, IL-4, IL-10); decreased complement activation (C3 and C4); inhibition of apoptosis of monocytes and macrophages; better neutrophil chemotaxis and oxidative function; and modulation of expression of adhesion molecules soon after critical injury or illness [28,67]. Thus, insulin may limit directly the post-stress inflammatory state that exists in acute illness and injury.
Clinical Rationale for Glycemic Control
Several clinical studies performed in the 1990s suggested that controlling glucose might improve outcomes of surgery and illness [15,68,69]. Retrospective studies demonstrated that glycemic control in patients with diabetes mellitus was associated with a reduction of SSI after cardiac surgery [15,68]. In a randomized study of diabetic patients, intensive insulin treatment improved the long-term survival of those suffering acute myocardial infarction, with a 28% relative risk reduction at five years of followup [69]. Two additional studies published simultaneously examined the effect of tight glucose control on cardiovascular morbidity and mortality rates in patients with type II diabetes mellitus and achieved contradictory results, one demonstrating benefit and the other harm [70,71].
Interest in glycemic control for critically ill patients exploded in 2001, when Van den Berghe et al. published the results of a landmark, single-center, randomized controlled trial examining continuous intravenous insulin therapy to control glucose [1]. The authors targeted glucose concentrations between 80 and 110 mg/dL vs. 180–200 mg/dL in critically ill surgical patients and demonstrated a 32% adjusted reduction of the in-hospital mortality rate with tighter control. However, these impressive results have been criticized for study flaws, including its single-center nature, the high mortality rate (5%) in the control group, the large volumes of intravenous glucose provided (causing hyperglycemia), the lack of blinding, and the fact that the study was stopped early because of determination of inferiority in the control group. Studies stopped early for benefit frequently over-estimate the effect of treatment. These results have sparked vigorous debate regarding the benefit and risks of tight glycemic control in various populations, although the practice has been accepted widely. Studies of glycemic control have been performed in both the peri-operative and ICU settings, although the majority have been studies of both surgical and non-surgical ICU populations [1,6–10,21,72–74], with a smaller number of studies focused specifically on the peri-operative setting, nearly all of which are in the setting of cardiac surgery [75–84]. These two separate (but at times overlapping) clinical indications are discussed separately below.
Glycemic control in critical illness
Since the original Van den Berghe et al. study in 2001 [1] (referred to frequently as Leuven 1), several large randomized trials, many smaller trials, and meta-analyses have been published. The larger trials include the Leuven 2 study, published in 2006 [10]; the Glucontrol trial from 2008 [7]; a study by Arabi et al., published in 2008 [8]; the VISEP trial from 2009 [9]; and the NICE-SUGAR trial, also published in 2009 [6]. These trials differ substantially in several ways, making direct comparisons of the results difficult (Table 1). In particular, the trials differ in the glucose targets in the control arms (four used a control target of 180–200 mg/dL, two a target of 140–180 mg/dL), rates of hypoglycemia, timing and type of nutritional provision, ICU population (surgical, medical, or mixed), percent of patients who were non-surgical, entry criteria (and thus severity of illness), and the number of centers included. The Leuven 1 study included 1,548 mechanically ventilated surgical patients, 62% of whom had undergone a cardiac surgical procedure. Insulin therapy and glucose provision were both initiated on admission, and the target range in the conventional arm was 180–200 mg/dL. Intensive insulin therapy (80–110 mg/dL) resulted in a 42.5% relative reduction in the ICU mortality rate (4.6% vs. 8.0%) and a 32% adjusted reduction in the in-hospital mortality rate (7.2% vs. 10.9%). Most of the mortality benefit (16.8% vs. 26.3% intensive insulin therapy (IIT) vs conventional) occurred in those patients who remained in the ICU for five days or longer (two thirds of whom were non-cardiac surgery patients). The rate of hypoglycemia was low in both arms: 5% in the IIT arm vs. <1% in the control arm.
Achieved glucose reported as mean morning concentration, except in Glucontrol study, which are overall mean concentrations.
Patients in VISEP study all had severe sepsis. Although no odds ratio was reported, did state no difference in the mortality rate.
hypoglycemia=<40 mg/dl.
APACHE=Acute Physiology and Chronic Health Evaluation; BMI=body mass index; CI=confidence interval; HES=hydroxyethyl starch; ICU=intensive care unit; IIT=intensive insulin therapy; LOS=length of stay; LR=lactated Ringers solution; MODS=multiple organ dysfunction syndrome; Mort=mortality; RRT=renal replacement therapy; SOFA=Sequential Organ Failure Assessment score.
The second published trial by Van den Berghe et al. (Leuven 2) [10] included 1,200 medical ICU patients who were estimated to require an ICU stay of at least three days and not tolerate an oral diet. The IIT and conventional targets were the same as those in Leuven 1, but glucose and nutritional provision were different. No provision of glucose was required, and nutritional supplementation awaited the tolerance of enteral feeding. Sixty-four percent of the study patients remained in the ICU for three days or longer. No significant difference in the mortality rate was observed in the total population (37.3% vs. 40%; p=0.33), but there was a significant difference in those patients who remained in the ICU for three days or longer, with a lower mortality rate (43.0% vs. 52.5%; p=0.009) for patients receiving IIT. Additionally, patients in the IIT arm were less likely to suffer renal failure and had fewer ventilator, ICU, and hospital days. Patients experienced a much higher rate of hypoglycemia than in the original study (18.7% vs. 5.1%), potentially related to less consistent nutritional support. These results may be interpreted as either negative for the entire population or positive for the population that was originally targeted. Two additional studies performed in mixed ICU populations (each with roughly 500 patients) examining IIT (80–110 mg/dL) vs. control arms targeting glucose concentrations of 180–200 mg/dL demonstrated non-significant relative reductions in the mortality rate (5% and 21%) [8,9].
Finally, two additional studies have examined IIT vs. control arm targets of 140–180 mg/dL, tighter than in the Leuven 1 and 2 studies. Both studies included mixed ICU populations and demonstrated a slight relative increase in the mortality rate in the IIT arm of the study relative to the control arm that was statistically significant in the larger of the studies [6,7]. These results suggest that 140–180 mg/dL is a more appropriate target than 80–110 mg/dL. However, a more recent randomized trial suggests that a lower target range of 80–110 mg/dL may be preferable in some populations to the higher target range of 140–180 mg/dL [73]. In this study, Jeschke et al. studied 239 severely burned (>30% total body surface area [TBSA]) children randomized 3:1 to conventional therapy vs. IIT [73]. The conventional target range was 140–180 mg/dL vs. 80–110 mg/dL in the IIT arm. Although the IIT arm had a significantly greater percentage of patients with high TBSA third-degree burns (52% vs. 44%; p<0.05), patients in the IIT arm had fewer infectious complications (8.2% vs. 22.6%; p<0.05), a dampened inflammatory and acute-phase response (p<0.05), better organ function (p<0.05), and higher total and lean body mass (p<0.05). The mortality statistics favored the IIT arm (4% vs. 11%; p=0.14). Power analysis for a 50% relative reduction in the mortality rate in a 3:1 randomization demonstrates that 570 patients would be required for the study to achieve significance. Thus, more remains to be determined regarding the variation with patient populations and target range of glycemic control.
Critically ill surgical populations, in contrast to findings of studies of medically critically ill patients, appear to benefit from tight glycemic control. A meta-analysis published in 2009 supports the mortality benefit of IIT in critically ill patients when studies are confined to those performed in surgical populations (Fig. 2) [72]. This analysis did not include the Jeschke et al. study performed in the pediatric burn population, which demonstrated a trend toward a lower mortality rate with tighter control [73]. The observation that critically ill and injured surgical patients have a greater benefit from IIT might be explained by the increase in IR induced by surgical and traumatic stress relative to that in medical patients, although no direct comparisons of IR in critically ill medical vs. surgical patients have been performed.
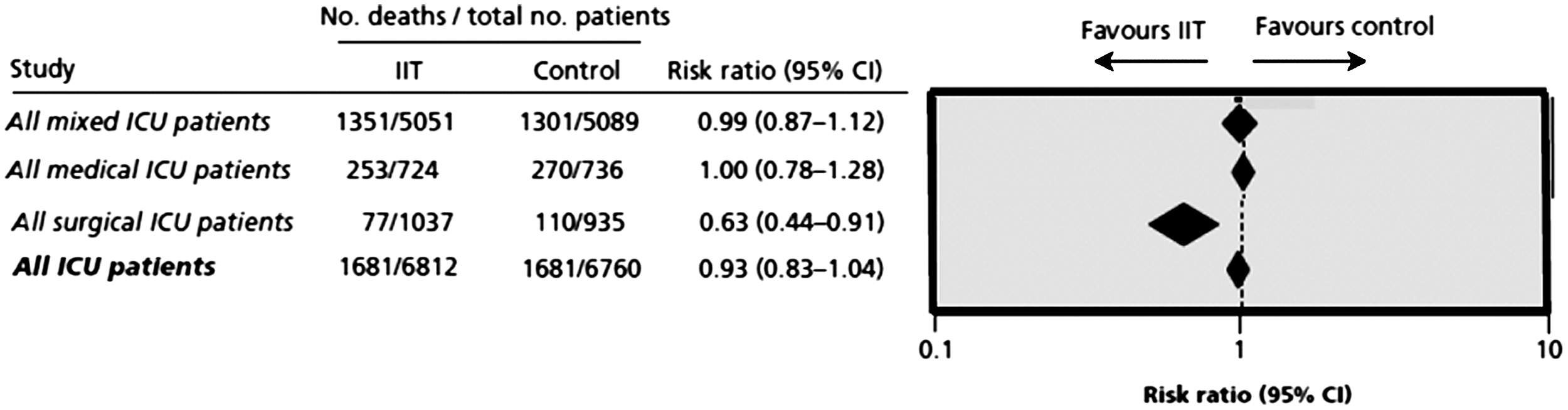
Risk ratios of death in clinical trials, comparing intensive insulin therapy (IIT) with conventional glycemic control, stratified by type of intensive care unit. Adapted from Griesdale DE, de Souza RJ, van Dam RM, et al. Intensive insulin therapy and mortality among critically ill patients: A meta-analysis including NICE-SUGAR study data. Can Med Assoc J 2009;180:821–827.
Factors contributing to variation in study results in critical illness
As noted above, the major randomized studies differ from each other in several ways that may alter their results (Table 1). These differences include:
• Patient populations—surgical vs. medical or mixed; • Target glucose range in the control arm; • Timing, type, and amount of nutritional support; • Median insulin dose in both the control and investigational arms; • Rate (and possibly severity) of hypoglycemia; • Time to initiation of insulin therapy; • Glycemic variability; • Protocol design and success of maintaining individual patient's serum glucose within the target range.
Patient population
As discussed, the results obtained in surgical patients appear to support IIT, whereas those in medical (or mixed) populations do not [72]. If this preliminary observation proves to be true, the physiologic explanation for this variation remains unclear but could be related to differences in IR in the two populations. Both surgical and traumatic stress clearly increase IR to a significant degree, contributing to hyperglycemia. However, inadequate data exist to allow direct comparison of IR in surgical vs. medical populations. Additionally, entry criteria differed in each study, so that the severity of illness, use of mechanical ventilation, and inotropic support may have differed, contributing to the differing treatment responses. As an example, nearly twice as many patients received inotropic support in the Leuven 1 study (75%) than in the Glucontrol study (39%). These differences in entry criteria make direct comparisons of studies difficult.
Target glucose range in the control arm
As noted above in the discussion of study results (Table 1), two large randomized studies included a control arm with a target glucose range of 140–180 mg/dL [6,7]. Both of these studies demonstrated a numerically higher mortality rate in the IIT arm. This has been interpreted variably as indicating that IIT either is not efficacious or is deleterious or that the mid-target range is superior to a range of 80–110 mg/dL. When interpreted in isolation, these data support a target range >80–110 mg/dL, but they neither negate nor provide information regarding the benefit of controlling glucose to <200 mg/dL. In addition, other differences confound the interpretation of the data. These studies differ from the Leuven 1 trial in several other ways that may contribute to the differences in observed outcome (Table 1). The differences in mean glucose concentration defined for each of the groups were less than in other studies, and the mean insulin doses were less than in the Leuven 1 study. No information is provided regarding glucose delivery within the first 24 h, but both protocols provided much less total nutritional support than the Leuven 1 study. In one study of 239 severely burned children, patients treated with a target of 80–110 mg/dL appeared to have better outcomes, with a lower incidence of sepsis, better organ function, greater lean and total body mass, more rapid resolution of inflammatory mediators, and a trend toward a lower mortality rate (4% vs. 11%), despite a larger percentage of third-degree large TBSA burns [73]. Thus, further studies are required to determine the optimal range for the various populations.
Nutritional support
The provision of glucose within the first 24 h, the total caloric intake, and the total protein and non-protein calories all appear to have differed significantly among the studies included in Table 1. The Leuven 1 study provided non-protein (18.5–19.1 non-protein kcal/kg/day) and protein (0.14–0.15 g/kg/day of nitrogen) calories, both of which are greater quantities than were given in subsequent major studies for which information is available. The provision of nutrition is in line with recommended nutritional support guidelines. By contrast, the NICE-SUGAR study provided significantly less than the recommended nutritional support. Additionally, in Leuven 1, patients were provided a calculated amount of glucose within the first 24 h of ICU admission (200–300 g/24 h, equivalent to 680–1,020 Kcal/24 h) with full nutritional support beginning on the second day. The early supply of this amount of glucose appears to be unique among the studies. Whether the variation in nutritional support contributed to the variation in outcomes is unclear.
A sub-analysis of 339 patients from the Leuven 1 study, all of whom remained in the ICU for at least one week, demonstrated that although the insulin dose for patients in the IIT arm was several-fold higher than in the conventional arm, serum insulin concentrations were only transiently higher with IIT despite much lower blood glucose concentrations, indicating greater insulin sensitivity [41]. Whether the early provision of glucose contributed to these findings is unknown. Extrapolation of data obtained from patients undergoing elective surgery suggests that early provision of glucose could play a role [3,4,28,34,85]. Although pre-operative fasting results in greater IR after surgery, provision of glucose during the fasting period decreases the change in IR, and normalization of the serum glucose concentration with insulin eliminates the increase in IR induced by surgery [3,85]. Contrary to this line of reasoning, some have argued that the provision of early glucose and parenteral nutrition in the Leuven 1 study may have represented overfeeding and contributed to a higher mortality rate in the control group. These hypotheses have not been tested directly, and inadequate data are available to draw reliable conclusions.
Rates of hypoglycemia
The risk of hypoglycemia induced by IIT has been a topic of considerable debate, and hypoglycemia has been assumed to contribute to worsened outcomes in patients who experience it. In all randomized studies, IIT targeting 80–110 mg/dL is associated with higher rates of hypoglycemia; however, the rates of hypoglycemia with IIT differ greatly among published studies, ranging from roughly 5% to 30% of patients experiencing one or more episodes of severe hypoglycemia (serum glucose <40 mg/dL). However, the association of hypoglycemia with death has not been consistent [86–90]. Whereas some studies [87,88] have demonstrated that hypoglycemia is associated independently with death, other studies [86,89,90] have not. The variation in the association of hypoglycemia with death may be related to the variation in time intervals between serum glucose assays in the various protocols. Many studies prescribe increasing the intervals between assays (as long as 4–6 h) when glucose control has “stabilized.” However, hypoglycemic events occur throughout the ICU stay, and increasing assay intervals raises the risk of hypoglycemia and contributes to more severe episodes and longer periods of hypoglycemia [91–93]. In an analysis of more than 1,100 critically ill or injured surgical patients, serum glucose analysis intervals of >3 h were associated with a three-fold greater rate of hypoglycemic glucose values than intervals <3 h.93 In another study of 1,392 critically ill surgical patients managed with a computer-assisted algorithm with glucose assays performed every 2 h by protocol, 11.1% of patients experienced one or more glucose values <50 mg/dL [92]. Patients with assays obtained at the upper 75th percentile of time interval (2 h 20 min from the previous assay) were 1.45 times more likely to experience a hypoglycemic event than patients assayed at the lower 25th percentile (1 h 40 min from the previous assay). Finally, a study of nearly continuous glucose assays (every 5 min) demonstrated a significant reduction in hypoglycemic events compared with assays performed at every-2-h intervals (1.6% vs. 11.5%) without an improvement in overall glycemic control [94]. Thus, glucose assay intervals extending beyond 2 h appear to increase the risk of serious hypoglycemic events and may increase the morbidity associated with them.
The incidence of hypoglycemia also is altered by nutritional provision. Vriensendorp et al. examined the predisposing factors for hypoglycemia in 2,500 critically ill patients, identifying changes in nutritional support as a significant risk factor. Lowering or discontinuing nutritional support (enteral, parenteral, or oral) and lowering the rate of 5% glucose infusion without adjusting insulin infusion both were associated with hypoglycemia (OR 6.6; 95% confidence interval [CI] 1.9–23.0 and OR, 6.0; 95% CI 0.72–49.0, respectively) [95]. More recently, the provision of glucose with protein (balanced nutrition) has been shown to be more protective than glucose provision alone. Patients who were not receiving both glucose and protein (with or without lipid) had a greater than a three-fold increase in the risk of hypoglycemia at the next glucose check (OR 3.6; p<0.001) than those who were receiving both, and the provision of glucose alone did not confer protection [91].
Time to insulin therapy
Recent data suggest that a delay in the initiation of insulin therapy for patients with hyperglycemia alters outcomes. In a recent study of more than 3,000 ICU patients treated with intravenous insulin, the time delay within the first 24 h between the glucose analysis and insulin infusion was associated independently with death and increased across the 24-h time period [96]. If this is true, the underlying physiology of this observation has not been elucidated but would be consistent with the hypothesis that elevations in glucose create a cellular insult that is additive over short time periods and the finding that acute elevations soon after critical illness and injury are associated independently with death despite tight glycemic control [97–99]. Whether the variation in the time of initiation of glycemic control contributes to the variation in findings in the large randomized trials cannot be determined because of inadequate data.
Glycemic variability
Following the publication of the Leuven 1 study, interest in factors that might alter outcome in the setting of glucose control increased. One measure that was associated independently with outcome in critically ill medical and surgical patients, patients with sepsis, patients with >20% TBSA burns, and critically injured patients [16,100–107] is glucose variability. Variability in blood glucose concentrations is more closely associated with death than either isolated or mean blood glucose values [16,100–103,105,107–113]. This association with death appears to be true whether patients are being treated with tight glycemic control [100,102,103,107,113] or not [16,100,101,105,106], and the finding has been demonstrated with differing measures of variability, including the standard deviation of glucose variables (with and without standardizing to the mean blood glucose value) [16,105,106], triangular index and percentile values of the individual range [102], difference between highest and lowest daily glucose concentrations [100], and absolute glucose change/time [101,103]. Factors contributing to glucose variability in the hospital setting are poorly characterized or understood but presumably are related to both intrinsic and extrinsic patient factors. Extrinsic factors likely include glycemic control algorithms, time intervals between glucose assays, mode of insulin delivery, and type and variability of nutritional support. Although glycemic variability could be postulated to be greater with longer time intervals between assays and with alterations in nutritional support, glycemic variability and its association with death appears to persist despite computerized insulin protocols, every-2-h analysis, and consistent nutritional support [92,102,103]. Intrinsic factors also appear to alter individual glycemic variability but are not well characterized or described. Factors demonstrated previously to be associated independently with variability include patient age, diabetes mellitus and daily insulin dose [100], and variability changes within individual patients during their ICU stays [92]. Glycemic variability and the ability to keep patients within the range safely may have altered the results of the various randomized trials, as the protocols differed significantly in their ability to keep patients within range [114]. This metric is poorly measured and assessed by mean or median glucose values. Further investigation is required to delineate the intrinsic and extrinsic factors influencing blood glucose variability over time both in and between individual patients. Additionally, interventions to decrease blood glucose variability likely are necessary to improve patient outcomes.
Protocol design and success of achieving individual patient's serum glucose values within target range
Analysis of the outcomes of patients in the different trials has incorporated mean or median glucose values for each individual cohort. Wide glycemic excursions within individual patients may be incorporated into these values, as well as wide variation of patient values within the entire study cohort. Analysis of mean and median values does not allow analysis of such fluctuations and thus cannot determine the success of a given protocol in controlling patients within a given range appropriately. Inter-patient and intra-patient variability within studies may significantly alter the success of glycemic control but has not been evaluated adequately with the data reported from clinical trials [114].
Reviews, Meta-Analysis, and Guidelines
Several systemic reviews and meta-analyses have been published, with disparate findings and results [72,78,115–117]. Although most demonstrate a significant reduction in infectious complications with tight glucose control, the effects on the mortality rate are inconsistent. These disparate findings result from differences in the study population, the handling of mixed ICU populations, and the inclusion of studies with potential design flaws. Despite the number of studies attempting to address this topic in critical illness, each of these studies is fraught with limitations and potential bias. The Leuven 2 trial was a single-center study, in which post-randomization stratification was used as an inclusion criterion. The Glucocontrol study was stopped early because of unintended protocol violations and thus was underpowered. Additionally, the study was not blinded, nutritional provision was not standardized, and differing experience and clinical practice at the various centers introduces a source of potential bias. Likewise, the VISEP study was stopped early because of safety concerns and was not blinded. The NICE-SUGAR trial has been criticized for its treatment approach, analysis, and randomization [118–121]. Again, this study was not blinded, the subjective criterion of expected length of ICU stay was part of the inclusion criteria, no standard nutritional protocol was utilized, and the care provided (except for management of blood glucose) was at the discretion of the critical care practitioner and may have differed by center. Finally, the study by Arabi et al. [8] was a single-center, un-blinded analysis.
In evaluating meta-analyses of the surgical subset, controversy is introduced by the issue of whether to include the >2,000 surgical patients from the NICE-SUGAR trial in the mixed ICU group. Centers participating in the NICE-SUGAR trial largely had mixed, not dedicated surgical, ICUs. In this trial, sub-group analysis of the surgical population showed an odds of death (OR 1.31; CI 1.07, 1.61), that did not reach statistical significance. However, these results should be interpreted cautiously, because the trial included patients admitted to mixed ICUs at 42 centers, in which all critical care (except management of blood glucose) was at the discretion of the practitioner. It is likely that there was variability from one center to the next in the protocols for other aspects of patient care, including nutritional support, use of antibiotics, ventilator support, or management of vasopressors. Furthermore, surgical and medical ICU patients differ the pathophysiology of their disease, and a benefit of a treatment in one sub-population may be masked when care is standardized across populations. Sub-group analyses of the surgical population treated in a mixed ICU may not reflect best practice for the surgical patient relative to the medical ICU patient.
The complexities of this topic, the data produced by various trials, and the conflicting results have produced disparate consensus guidelines and recommendations by national organizations [11,122]. The authors concur with the recommendations of the American Association of Clinical Endocrinologists and the American Diabetes Association that persistent acute elevations of serum glucose above the normal range are deleterious, and control of serum glucose below <150 mg/dL protects against hypoglycemia.
Perioperative Glycemic Control: Rationale and Results
Although a substantial amount of data is available on the critically ill patient population, markedly fewer data exist specifically regarding glycemic control for the prevention of peri-operative morbidity and death. Peri-operative and peri-traumatic hyperglycemia is associated with infectious complications, longer stays, and death, even when adjusted for confounding variables [14,23,24,123]. In a study of 1,000 consecutive cardiac surgery patients, a single post-operative glucose value >200 mg/dL was independently associated with sternal SSI and increased proportionally with the degree to which the concentration was above 200 mg/dL (ORs of SSIs: 2.54 for glucose 200–249, 2.97 for 250–299, and 3.32 for ≥300 mg/dL) [14]. Similar associations have been demonstrated between glucose concentrations and infectious complications in elective general and vascular cases [123], after traumatic injury [24], and in orthopedic cases [23]. In patients with diabetes mellitus, acute post-operative glucose elevations appear to have a more pronounced association with infection than pre-operative glycemic control. In a study that examined the effect of long-term vs. acute glycemic control on post-operative infection rates in 55,408 diabetic patients undergoing non-cardiac surgery, higher infection rates were associated with a mean 0–24-h post-operative glucose concentration of 150–250 mg/dL (adjusted incidence rate ratio 1.22) and >250 mg/dL (adjusted incidence rate ratio of 1.43) relative to patients with glucose values in the normal range [124]. Pre-operative HbA1C and serum glucose concentrations were not associated with infectious complications. In comparison, the adjusted incidence rates for other variables were cigarette smoking, 1.15; emergency surgery, 1.58; non-clean case, 1.32; and American Society of Anesthesiologists class 4 or 5, 1.32.
Cardiac surgery
Most interventional data are from cardiac surgery patients, particularly patients with diabetes mellitus, and support controlling peri-operative serum glucose to concentrations at least <200 mg/dL with insulin infusion [15,68,77,78,81,82]. In a non-randomized before-and-after study of nearly 2,500 diabetic patients undergoing open heart procedures, Furnary et al. demonstrated significantly lower serum glucose concentrations and significant reductions in sternal SSIs using continuous insulin infusion targeting glucose between 150 and 200 mg/dL vs. a sliding-scale subcutaneous regimen to keep glucose <200 mg/dL [15]. A randomized study of 93 diabetic cardiovascular patients demonstrated better and more rapid glycemic control with continuous insulin vs. a subcutaneous regimen targeting the same range of 150–200 mg/dL [82]. Sternal infections were numerically but non-significantly fewer in the continuous infusion arm. Lazar et al. randomized 141 diabetic patients undergoing cardiac surgery to insulin infusion combined with a 5% glucose and potassium solution (GIK) targeting a serum glucose concentration of 120–200 mg/dL vs. subcutaneous insulin to keep serum glucose <250 mg/dL [81]. Patients in the study arm had a significantly lower incidence of post-operative atrial fibrillation (16.6% vs. 42%; p=0.0017), shorter post-operative length of stay (6.5±0.1 vs. 9.2±0.3 days; p=0.003), fewer peri-operative infections (0 vs. 13%; p=0.01), a survival advantage during the initial two years after surgery (p=0.04), and fewer episodes of recurrent ischemia (5% vs. 19%; p=0.01). A meta-analysis of peri-operative glycemic control by Gandhi et al. suggests a mortality benefit for glycemic control [78]. However, this analysis includes a heterogenous group of studies with various designs, variable interventions, and differing treatment periods published between 1977 and 2007. All studies used in the analysis of mortality rates included only cardiac surgery patients except for the Leuven 1 study. Most studies examined the use of GIK without glucose targets. The Lazar et al. study was not included in this analysis.
Non-cardiac surgery
Some limited data from randomized trials suggest that peri-operative glycemic control may be beneficial in non-cardiac patients, although the studies do not allow adequate assessment of the overall benefit. Grey et al. demonstrated a decreased rate of nosocomial infections in 61 patients admitted to a surgical ICU and assigned randomly to glycemic control with intravenous insulin targeting a serum glucose concentration of 80–120 mg/dL vs. standard therapy targeting glucose at 180–220 mg/dL [79]. A study of 78 patients undergoing aneurysm clipping after subarachnoid hemorrhage demonstrated fewer post-operative infections in patients who received intravenous insulin targeting serum glucose between 80 and 120 mg/dL vs. maintaining it <220 mg/dL [75]. However, no difference in neurologic outcome or mortality rate was demonstrated in this small study. Additionally, a randomized study of 236 patients undergoing vascular surgery procedures demonstrated a reduction in a composite endpoint of death, myocardial infarction, and congestive heart failure in patients randomized to intravenous insulin infusion targeting blood glucose of 100–150 mg/dL initiated at the start of surgery and continuing for 48 h post-operatively vs. subcutaneous insulin for serum glucose >150 mg/dL [84]. Finally, one recent randomized controlled trial strongly suggests that tighter glycemic control in the non-critically ill post-operative period in general surgical patients reduces infectious complications. Two hundred eleven patients with type II diabetes mellitus were randomized to two post-operative control regimens: A sliding scale four times daily with regular insulin vs. basal-bolus therapy with insulin glargine once daily and insulin glulisine before meals. The basal-bolus regimen resulted in better glycemic control, with lower mean fasting glucose concentrations (155 mg/dL vs. 165 mg/dL) and lower mean daily glucose (157 mg/dL vs. 176 mg/dL) and significantly reduced composite complications (SSI, pneumonia, bacteremia, respiratory failure, and renal failure: 8.6% vs. 24.3%; p=0.003) and SSI (2.9% vs. 10.3%; p=0.050) [125].
Conclusions
Despite an extensive body of literature on the use of IIT in the critically ill population, controversy persists regarding the appropriate target glucose range, the role of nutritional support, the relative importance of decreasing blood glucose variability in improving outcomes, and the relation between hypoglycemia and death. In the critically ill surgical patient, the body of literature supports glycemic control when the glucose concentration exceeds 200 mg/dL. For those surgical patients who are critically ill, the data still favor the use of IIT to control hyperglycemia, but the optimal degree of control has not been established. However, the use of intravenous insulin in the SICU population appears to reduce infectious complications, with a trend toward a lower mortality rate. On the other hand, the risk of hypoglycemia clearly is increased with tighter glycemic control, potentially producing morbidity or death.
We recommend controlling blood glucose with a target range of 100–140 mg/dL in both critically ill and post-operative surgical patients. In the critically ill setting, this should be accomplished using intravenous insulin, and in the post-operative, non-critically ill patient, using subcutaneous insulin. Frequent blood glucose monitoring should accompany both types of therapy. In the critically ill, minimizing the risk of hypoglycemia through frequent monitoring (at least every 2 h), providing early nutritional support (ideally to include carbohydrate and protein), and minimizing blood glucose variability should remain important components of IIT protocols.
In the setting of perioperative glycemic control, fewer data exist. Again, the literature suggests that maintaining serum glucose concentrations <180–200 mg/dL is beneficial, and we suggest that a target of 100–140 mg/dL provides a reasonable range by which to minimize infectious complications while avoiding severe hypoglycemia. Very few data exist on intra-operative control in non-cardiac surgery patients, and no recommendations can be made specifically for this procedure. Many questions remain unanswered, including the contribution of insulin administration vs. glycemic control, the contribution of nutritional support to IR and glycemic control, the intrinsic and extrinsic factors that contribute to blood glucose variability, and the most appropriate goal blood glucose range by patient population and risk.
Author Disclosure Statement
No conflicting financial interests exist.