
Abstract
Abstract
Background:
Tetanus is now a rare disease in the Western world, but not so in developing countries. Cephalic tetanus, unlike some other local forms of the disease, is likely to be fatal.
Methods:
We describe the clinical presentation of a case of fatal cephalic tetanus complicating an unattended open non-severe head injury with a review of the literature on the disease.
Results:
Few cases of cephalic tetanus complicating head injury are found in the world literature, and many were diagnosed late. Cephalic tetanus from open or compound depressed skull fracture is even more rare. Our patient was a young male with an uncertain tetanus immunization history who sustained mild head injury (scalp laceration) and an unattended open depressed skull fracture in a motorcycle crash. He developed cephalic tetanus seven days later, presented late to our service, and died while being prepared for surgical debridement of his cranial wounds. At the immediate post-trauma medical contact, in an across-the-street “clinic,” he had received suboptimal care for his head wound and inadequate tetanus prophylaxis.
Conclusion:
Cephalic tetanus is a rare form of the disease. Although it is preventable easily by well-established medical and surgical treatment paradigms, it continues to catch many clinicians disastrously unaware.
Comparatively few cases of cephalic tetanus have been reported as the result of head trauma and even fewer from compound or open depressed skull fractures [10–12]. We were involved recently in the clinical care of a patient with fatal tetanus complicating an unattended open depressed skull fracture from an otherwise minor head injury. The clinical report of this case is presented herein. We also explored the English literature dating back beyond the 20th century for documented cases of cephalic tetanus complicating head injury. A brief review of these cases is the other subject of this report.
Case Report
A 24-year-old male, a commercial bus driver, first presented to the physicians in our university teaching hospital with a history of drooling of saliva, trismus, and body spasms of one day's duration. He had been the victim of a pedestrian motorcycle crash within the metropolis eight days earlier. He sustained a left frontal laceration from being knocked down but was apparently otherwise unhurt; there was no history of loss of consciousness, seizures, vomiting, headache, or focal neurologic deficit. He received first aid care, including suturing of the scalp laceration, in an unnamed nearby “private hospital,” and was said to have “declined” the antimicrobial agent prescribed in that facility. Apparently, no anti-tetanus treatment or prophylaxis was administered.
Seven days after the trauma, he presented to another clinic with trismus. There, in addition to some other general medical care, he was given intramuscular tetanus toxoid but not antitetanus serum. He was then referred to our hospital. His previous tetanus immunization history could not be ascertained.
He presented eight days after trauma to our hospital's accident and emergency room with the tetanus symptomatology mentioned above. He was conscious but in distress and agitated; the vital signs were normal. There was a sutured left frontal scalp laceration, which apparently was healing well. A clinical diagnosis of tetanus was made, and treatment was outlined, which included clinical laboratory investigations, intravenous infusions of diazepam (40 mg) and magnesium sulfate (10 mg/h), and intravenous metronidazole and ceftazidime. He also had repeated intramuscular administration of 0.5 mL of tetanus toxoid and administration of equine anti-tetanus serum (ATS) 10,000 units intramuscularly.
On day nine after trauma (the second day after admission in our hospital), a screening skull radiograph showed a depressed skull fracture, and a neurosurgical consult was sought. Examination revealed a critically ill, drowsy (probably as the result of sedation), intubated patient with a Glasgow Coma Scale score of 8 points, that is, eye opening on command (3); intubated and hence no verbal response (1), and strong flexor withdrawal in response to pain (4). There was neck stiffness, left cranial nerve VII palsy, left hemiparesis, and frequent generalized muscle spasms. He also had evidence of sympathetic autonomic derangement: Blood pressure 114/70 to 197/111 mm Hg; pulse rate 120–140 beats/min, and ventilation 20–38 breaths/min. The body temperature ranged from 36°C to 38°C.
The skull radiographs (Fig. 1) showed a left frontal comminuted depressed skull fracture in association with the sutured scalp laceration. The patient could not afford the requested cranial CT scan, urgent debridement the fracture was planned as a crucial part of the care of his cephalic tetanus. However, he suffered sudden cardiorespiratory arrest on his way to the operating room, and attempts at resuscitation failed.
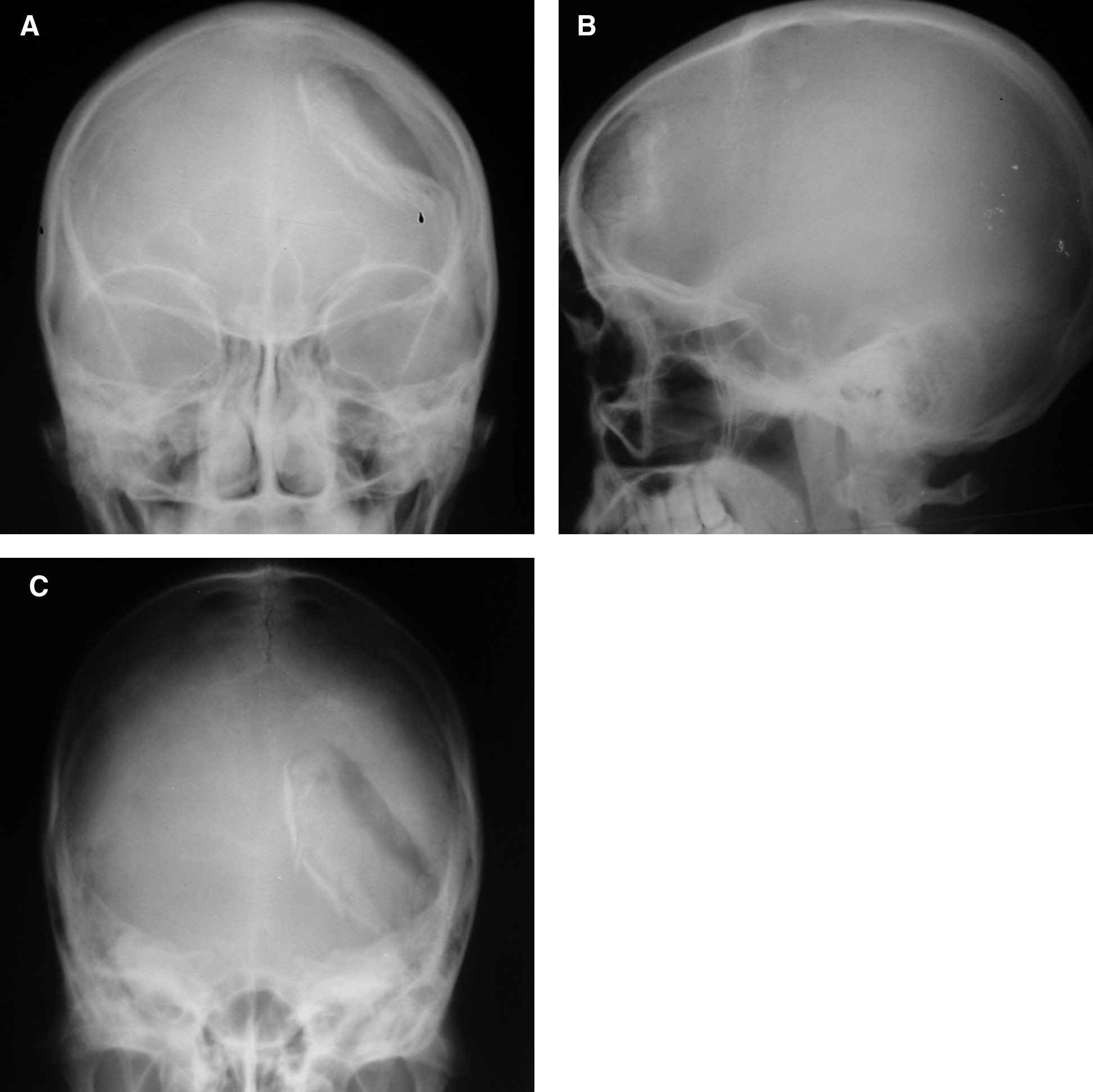
Skull radiographs in (
Discussion
This case illustration is another example of the disastrous result that can follow inexpertly treated “minor” trauma: Fatal cephalic tetanus arising from an unattended open depressed skull fracture sustained at an otherwise-minor head injury one week earlier in a young man in the 21st century. Tetanus is rare in many Western countries because of effective population-wide preventive immunization programs. Hence, out of the current global yearly incidence of about one million cases, an average of only 4, 12–15, 30–50, and 50–70 cases are seen in Canada, the UK, Japan, and United States, respectively, whereas tetanus still is a major health problem in many developing countries because of the challenges in delivering preventive medicine [4,13–16].
Tetanus actually is not an infection, but rather a toxemia, with a characteristic nervous system predilection [13]. Of course, the source of the tissue toxins in man is C. tetani, an obligate anaerobic gram-positive, spore-forming bacillus found ubiquitously in the soil and in the excrement of some farm animals and of human beings. The spores gain entry to human tissues through traumatic or inflammatory/infected wounds. There, if they encounter an anaerobic environment (more common in contaminated open trauma), they germinate into the vegetative form of the organism, the toxin-producing bacilli [2,13,17]. Thus, the clinical form of a particular case; that is, either general or local tetanus, is determined, among many factors, by the patient's age and, importantly, by the site of entry [16].
Tetanospasmin is the toxin responsible for the clinical manifestations of tetanus. It works through central interruption of the inhibitory gamma-amino butyric acid (GABA)-ergic and glycinergic neurons and of inhibitory interneurons at the level of the spinal cord. The practical approach to reducing the burden of this deadly disease therefore is prevention. This involves administration of statutory numbers of active immunizations before adolescence and continuous scheduled boosters periodically, at either 5 or 10 years, to maintain immunity [13]. However, in spite of previous active immunization, occasionally overwhelming infection with excessive toxin production may be attributable to inadequate surgical treatment of the offending wound, especially wounds in the craniofacial regions or that are contaminated heavily [7,18]. Clinical tetanus is more likely to be observed in persons whose last booster tetanus immunization dates back more than five years and moreso if there is an uncertain or no immunization history [13]. Such was the case here in a patient with an untreated open depressed skull fracture.
Every surgical incision site with the potential for contamination, especially if the subject has questionable immunization status, as in the case described here, should receive the full complement of preemptive care aimed at preventing tetanus. This care is a three-pronged approach involving immunization with the toxoid to boost the body's active immunity, and concurrent administration of high doses of human tetanus antiserum (or the equine serum in limited-resource areas). The latter is necessary because active immunization with toxoid alone does not combat any already-elaborated toxins. The third prong, possibly the one most likely to be overlooked, is proper care of the offending wound [18]. This site, especially if it is in the head and neck region, should be sought out and debrided aggressively to lay bare fully, and thus oxygenate, the potential anaerobic sanctuary of the toxin-producing microorganism. Sadly, these points were missed in the case illustrated here. First, this patient should have received antiserum as well as toxoid, and not toxoid alone, at the first suspicion of tetanus [14,19]. But of even more clinical and neurosurgical importance was the inexpert care of the head wound, causing untimely late diagnosis and inadequate treatment of the open depressed skull fracture, the most likely cistern of his tetanus toxemia.
Cephalic tetanus
Cephalic tetanus is a form of local tetanus that many times transitions to the generalized form. Its cardinal symptomatology before it becomes generalized is trismus/drooling and deficits of one or more cranial nerves (most usually CNVII) in the presence of a head or neck wound [13,20,21]. There are conflicting views regarding when this unique form of tetanus was first described: Either sometime between 1869 and 1872 by Rose [19,22]; earlier, in 1830, by Sir Charles Bell [19]; or even earlier still in the 1550s B.C.E. by Egyptian writers as documented in the Edwin Smith papyrus [12]. Nevertheless, from medical antiquity to the current era, cephalic tetanus remains the rarest of all forms of the disease. A wartime military report from Europe early in the last century found only two examples of the cephalic form among more than 2,500 cases of clinical tetanus, whereas a more contemporary civilian series reported only about a 2% prevalence of head tetanus in more than 1,000 cases [23,24].
Cephalic tetanus following head injury
Although the original definition of cephalic tetanus is that of local tetanus that originates from an injury to the head or neck [19], few cases described in the literature followed head injury. Not only do most cases involve only the facial region below the eyebrows but the bulk of the offending injuries are situated in the territory of CNV (trigeminal nerve) [22], and moreso in the periorbital region [9], and are caused on many an occasion by what is essentially minor trauma caused by objects such as wood splinters, keys, whips, a rooster peck, or hockey stick, and only occasionally by firearms [2,3,8,9,11,19,22,25–27].
In addition, the few cases attributable to head injury usually were secondary to small scalp lacerations of the frontal temporal regions as a result of minor trauma [2,9,11,12,14, 18,20,21,28,29]. Cases secondary to open depressed skull fracture are almost unknown. We are aware of only one unequivocal such case in the English-language literature reportedly dating back to 1550 B.C.E., and it was said to have been documented as tetanus from cranial trauma in the Edwin Smith papyrus from ancient Egypt [12].
Herein lies the importance of this clinical scenario. Cephalic tetanus is so demonstrably rare, and that from open depressed skull fracture virtually unknown, that in the early clinical phase, its diagnostic apprehension is apt to be missed by managing clinicians, and it may be confused with more benign conditions such as Bell palsy, temporomandibular joint dysfunction, and even malaria or hysteria [4,13–15,24].
This is a main reason the clinical diagnosis of cephalic tetanus usually is delayed until disease progression to the more unmistakable general presentation of tetanus, including trismus, spasms, rigidity, and autonomic derangements, as seen in our case. This also is why, in many series, the mortality rate for this form of tetanus is much higher than that of other forms, being as high as 53%–80% in early reports [11,29]. And although the mortality figures in the contemporary times have dropped to 16% or so, missed diagnosis or delayed treatment still is very common, occasionally with disastrous results [8,10,19,24].
Conclusions
Cephalic tetanus secondary to head injury is rare, and that from open depressed skull fracture, as we illustrate here, is almost unknown. Although the disease, potentially fatal as in our case, should be highly salvageable in the medical practice of the current era, clinical awareness is low, and many potentially salvageable patients continue to be lost to the toxemia.
Footnotes
Author Disclosure Statement
The authors have no competing financial interests to declare.