
Abstract
Abstract
Background:
Endocarditis is a potentially lethal complication of implantation of a cardioverter–defibrillator (ICD).
Methods:
We report the case of a 62-year-old male with candidemia and vegetation from a large implantable ICD lead that could not be extracted percutaneously. The ICD system was completely and successfully removed through pocket re-exploration and sternotomy with cardiopulmonary bypass.
Results:
Although the patient was considered at high risk from thrombocytopenia, systemic infection, and symptomatic heart failure with a very low ejection fraction, the surgical procedure used to remove his ICD provided a good clinical outcome.
Conclusion:
An early and aggressive combination of surgical and medical therapy is effective for the removal of an ICD causing endocarditis, and reimplantation of the device is safe when guided by principles for preventing infection.
A 62-year-old male with coronary artery disease, congestive heart failure, hepatitis C infection, and diabetes mellitus presented with increasing dyspnea on exertion and pressure in his chest. Eleven months before presentation the patient had had a ICD implanted for the primary prevention of sudden cardiac death. He was admitted with fever and an infiltrate in his upper right lung. Blood cultures were positive for C. albicans. In accordance with the recommendations for managing such disease, an antifungal regimen of intravenous fluconazole (200 mg/q12h) was begun. A transesophageal echocardiogram was done secondary to fungemia revealed a 4 cm, oscillating, echogenic mass anchored to the right atrial portion of his ICD lead and almost obstructing the orifice of his tricuspid valve (Figs. 1 and 2). The vegetation was anchored entirely to the ICD lead, without contact with any endocardial surface. Extraction of the ICD lead with the vegetation was recommended, together with removal of the patient's ICD and its other leads. Percutaneous extraction of the lead bearing the vegetation was considered unsafe because of a high risk of distal embolization of the pulmonary artery, with potential major hemodynamic consequences including circulatory collapse.
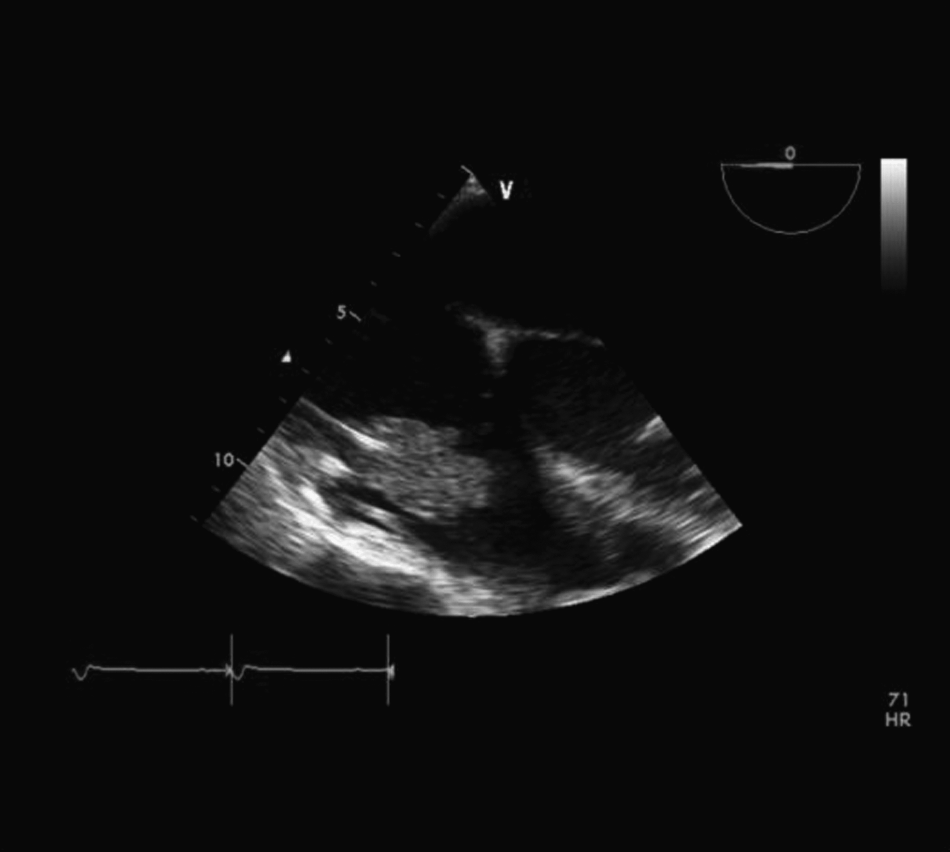
Transesophageal echocardiogram revealing a 4-cm echogenic mass anchored to the right atrial portion of the lead of the implantable cardioverter–defibrillator and almost obstructing the orifice of the tricuspid valve.
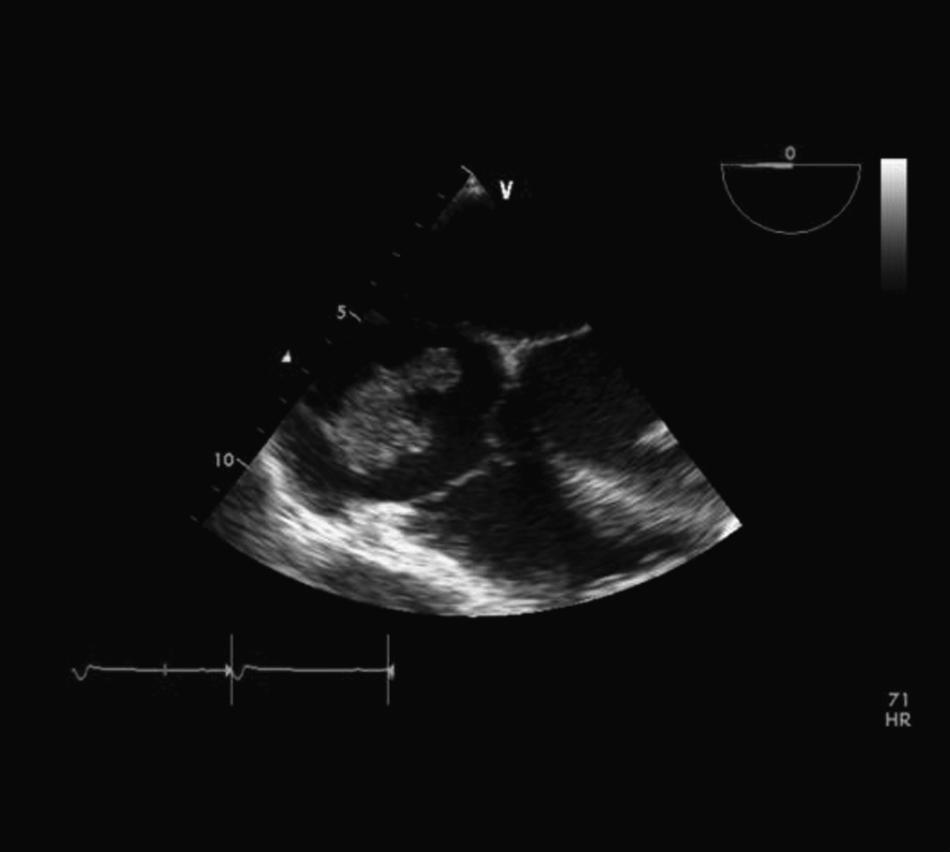
Transesophageal echocardiogram showing a large, free-floating vegetation attached to the right atrial pacing lead of the implantable cardioverter–defibrillator.
A full midline sternotomy was done and cardiopulmonary bypass (CPB) was initiated with perfusion through the ascending aorta and bicaval drainage. Aortic cross-clamping and cardioplegia were not necessary. The right atrium was opened with the heart beating, and revealed a 5-cm vegetation attached to the right atrial ICD lead (Fig. 3). The lead was cut proximal to the vegetation and the distal portion of the lead was removed with the vegetation attached, to ensure minimal disruption of the vegetation and prevent distal embolization. The proximal portions of the ICD leads and the pulse generator of the ICD were removed without complication through a separate incision made into the generator pocket. The right atrium was closed and CPB was discontinued without difficulty. The patient's postoperative course was uneventful and he was discharged from the hospital on postoperative day 3. He was to remain on oral fluconazole therapy (200 mg qd, p.o.) for 6 wks before reimplantation of his ICD.

Gross specimen with a 4.5×4.5×1.6 cm vegetation adherent to the lead of the implantable cardioverter–defibrillator.
Discussion
Implantable pacemakers and ICDs are lifesaving therapeutic devices for patients with cardiac arrhythmias. Clinical indications for the use of devices for controlling cardiac rhythm have increased over the past several years, and this has led to an increased incidence of infection associated with such devices [3]. Although endocarditis stemming from electrode leads occurs in <1% of pacemaker and ICD implants [4], infectious endocarditis remains a major complication of the use of implantable devices for regulating cardiac rhythm because of the inherent difficulties in its management and its potential for having adverse outcomes, with mortality rates ranging from 13% to 30% [2,5].
Risk factors for infections from pacemakers and ICD leads include chronic illnesses. Among these are diabetes mellitus, immunosuppressive therapy, malignant tumors, advanced age, and steroid treatment [6]. Conditions involving an ICD itself, such as manipulation or extrusion of the device and battery exchange, as well as skin contamination at the time of surgery, can also lead to infection [2].
In 80% to 100% of cases, ICD-related infectious endocarditis yields positive blood cultures [2]. The most common pathogens in such endocarditis are staphylococci, and of these, the most commonly encountered species is Staphlococcus aureus [1, 5, 7] Infectious endocarditis associated with Candida is not common, and this fungus remains an opportunistic pathogen in such disease. Such endocarditis is generally right-sided, and Candida is the most common fungal pathogen associated with endocarditis involving prosthetic valves [8]. The ability of Candida species to adhere to various plastics favors their colonization of foreign intravascular and intracardiac materials [9]. Large endocardial vegetations are frequent findings in cases of fungal endocarditis, although vegetations larger than 3 cm are exceedingly rare [7, 9]. Current European guidelines recommend early cardiac surgical intervention in cases of fungal endocarditis, especially if a prosthetic intracardiac device is involved [10].
The leads of ICDs can be extracted both percutaneously and surgically. The simplest method for their extraction is direct, gentle manual traction. However, this is associated with many complications, including tearing of the tricuspid valve, damage to the right heart, and arrhythmias [6]; pulmonary embolism has been reported in 30% of patients after the percutaneous removal of ICD leads [4]. Intravascular approaches to the removal of ICD leads, through the use of wire-loop snares, hook-tipped wires, basket retrievers, and grasping forceps have also been described, but commonly disrupt the lead being removed [6].
The main indications for surgical treatment in endocarditis caused by infected ICD leads are heart failure from valvular regurgitation and uncontrolled infection [8]. Percutaneous extraction of infected leads is the method of choice, and surgery is reserved for contraindications to or failure of percutaneous techniques, as in cases involving large vegetations or tricuspid regurgitation [8]. A vegetation on a lead poses additional difficulties for extraction of the lead. The percutaneous removal of leads is safer with vegetations <1 cm because septic embolization can occur with vegetations larger than this [1,2]. Historically, surgery was the main means for removing leads with such larger vegetations, and a surgical approach involving sternotomy has recently been considered a safe method for their removal [6]. This allows complete visualization of the affected area and minimizes potential injury to the right ventricle and tricuspid valve. It can also prevent the embolization of a vegetation into the pulmonary circulation. However, immediate post-operative complications of sternotomy for this purpose are relatively common. Among the most frequent such complications are severe coagulopathy requiring treatment with clotting factors, re-exploration of the chest for bleeding or tamponade, acute kidney injury requiring hemodialysis, stroke, low-cardiac–output syndrome, and pneumonia [10].
Conservative medical therapy for lead endocarditis often fails [11]. Patients treated medically have been reported to have a mean of 1.6 relapses until they undergo surgical treatment [4]. Complete removal of the ICD with the infecting lead is essential to eradicate infection and prevent recurrent bacteremia or fungemia. Extraction and explantation of the ICD with antibiotic coverage is effective in eradicating infection but carries a mortality rate of 12.5% [11]. The presence of intracardiac vegetations identifies an increased risk for complications and early mortality from systemic infection [1]. Permanently implanted devices for controlling cardiac rhythm can safely be reimplanted provided that blood cultures remain sterile until this is done and thereafter [1].
In the case described here the patient was in poor condition, with postoperative sepsis. Neither prompt percutanous procedures, such as, manual extraction of the vegetation-bearing lead, nor intravascular approaches to its removal were performed because they would have led to dissemination of and embolization by the vegetation on the lead. Antifungal therapy geared to the patient's blood cultures were continued after removal of his ICD.
Infections caused by ICD leads are associated with high rates of morbidity and mortality. Early, aggressive, combined surgical and medical therapy is recommended for their management. The risk of transvenous removal of an ICD lead causing pulmonary embolism should be weighed against the risks of the CPB needed for this procedure. Reimplantation of an ICD that has caused infectious endocarditis is both feasible and safe when guided by principles for the eradication and prevention of infectious disease.
Footnotes
Author Disclosure Statement
No competing financial interests exist.