
Abstract
Abstract
Background:
Selective decontamination of the digestive tract (SDD) has been advocated to prevent ventilator-associated pneumonia (VAP) and possibly other nosocomial infections. However, its incorporation into standard health care practices has been limited.
Methods:
Comprehensive literature search using www.pubmed.gov and derivative cross-references.
Results:
The abundance of basic science and clinical literature largely supports the concept that the incidence of VAP declines after the introduction of SDD, although there are some controversial aspects. Several meta-analyses and recent controlled clinical trials have supported the benefit of SDD. A few years ago, the Institute for Healthcare Improvement introduced the “ventilator bundle,” a set of simple evidence-based measures designed to reduce the incidence of pneumonia. These measures have been implemented rapidly throughout the country. Of the four initial measures (elevation of the head of the bed, daily “sedation vacations” with assessment of readiness for endotracheal extubation, prophylaxis against stress-related gastric mucosal hemorrhage, and deep venous thrombosis prophylaxis), only the first two affect the development of VAP either directly or indirectly.
Conclusions:
The evidence supporting SDD as a prevention measure for VAP is at least as good as that supporting the ventilator bundle, if not better. At many centers, a topical oral antiseptic (e.g., chlorhexidine) has been incorporated as a fifth element of the ventilator bundle.
A few years ago, the Institute for Healthcare Improvement (IHI) introduced the “ventilator bundle,” a set of simple evidence-based measures designed to reduce the incidence of pneumonia [1]. These measures have been put in place rapidly in hospitals throughout the country. Of the four measures advocated initially (elevation of the head of the bed, daily “sedation vacations” with assessment of readiness for endotracheal extubation, prophylaxis against stress-related gastric mucosal hemorrhage, and deep venous thrombosis prophylaxis), only the first two affect the development of VAP either directly or indirectly. The evidence supporting SDD as a preventive measure for VAP is at least as good as that for those measures, if not better. A topical oral antiseptic (e.g., chlorhexidine), which is undeniably a form of SDD, has been incorporated as a fifth element of the ventilator bundle [2].
Background and Mechanisms
The most common cause of death in critically ill patients is multiple organ dysfunction syndrome, typically as a result of infection and sepsis [3,4]. The infections that critically ill patients develop invariably involve organisms that colonized him or her initially, regardless of the anatomic location of the infections. Whereas healthcare workers are concerned, appropriately, about transmitting organisms from one patient to another, it is important to realize that there are vastly more organisms already resident on the patient's epithelial surfaces than could possibly be transmitted during care delivery. However, transmission via healthcare workers is detectable and often is documented by the involvement of organisms resistant to antimicrobial agents, which serves as a marker of transmission. Because of this notoriety, a great deal of attention has been directed at hygiene and precautions against microbial transmission [5]. Yet, the huge reservoir of organisms living on the patient's epithelial surfaces, combined with the challenges of maintaining the personal hygiene of a critically ill patient, makes the risk of infection an ever-present one. It is always sobering to realize during rounds that the individual most likely not to have showered that day is the patient. Moreover, even when an organism has been transmitted to a patient, that organism is a colonist needing an opportunity to invade tissue through epithelial defects if it is to produce an infection. Topical “bathing” with chlorhexidine-impregnated wipes has decreased the risk of some intensive care unit (ICU) infections [6].
The possibility was raised in the early 1980s that colonists in the gastrointestinal tract could cause much of the sepsis encountered in critically ill patients. After a thorough workup and investigation that included autopsy data, Goris et al. were unable to identify an infectious source of systemic inflammation in 50 of 92 patients (54%) with multiple organ failure [7]. Other investigators described patients who appeared to have sepsis clinically, yet did not have positive blood cultures or any other identifiable microbial source [8,9]. These findings, coupled with the huge bacterial load colonizing the gut lumen, make the intestinal tract a potential source for infectious problems resulting from barrier violations [10].
Healthcare workers are encouraged to be compulsive about hand washing and using protective barriers when dealing with hospitalized patients. This practice results primarily from the desire to avoid transmitting organisms resistant to various antibiotics because of the more complicated care that ensues with such infections. Whenever such an infection develops, the process of transmission can be recognized through an epidemiologic survey of similar infections of other patients in the unit. This resistance transmission creates a sense that such transmission causes infection, which is true. However, a resistant organism often is able to capitalize on barrier violations and establish an infection because the empiric or directed antibiotics used fail to provide coverage. Thus, even transmitted organisms become colonists in their new home before they can infect through tissue invasion (and failure of host defenses).
However, it can be argued that many, possibly most, hospital-acquired infections actually involve organisms that already have colonized the patient, not those transmitted to him or her by others. After all, there are vastly more organisms in constant contact with the host than could possibly be transmitted to the patient by healthcare workers.
Most cases of VAP develop from aspiration or micro-aspiration of oropharyngeal contents [11]. The oropharynx is considered the second most heavily colonized mucosal surface of the human body, after the colon. Yet, the human trachea is essentially sterile under normal conditions [12–17]. Unlike whales, which have a separate blowhole for air and a sieve for their diet of plankton [18], humans have a single aperture through which they inhale and exhale air and ingest food. Because of this, a variety of mechanisms create an elaborate baffle mechanism that normally prevents food and bacteria-laden pharyngeal secretions from entering the trachea (Fig. 1).
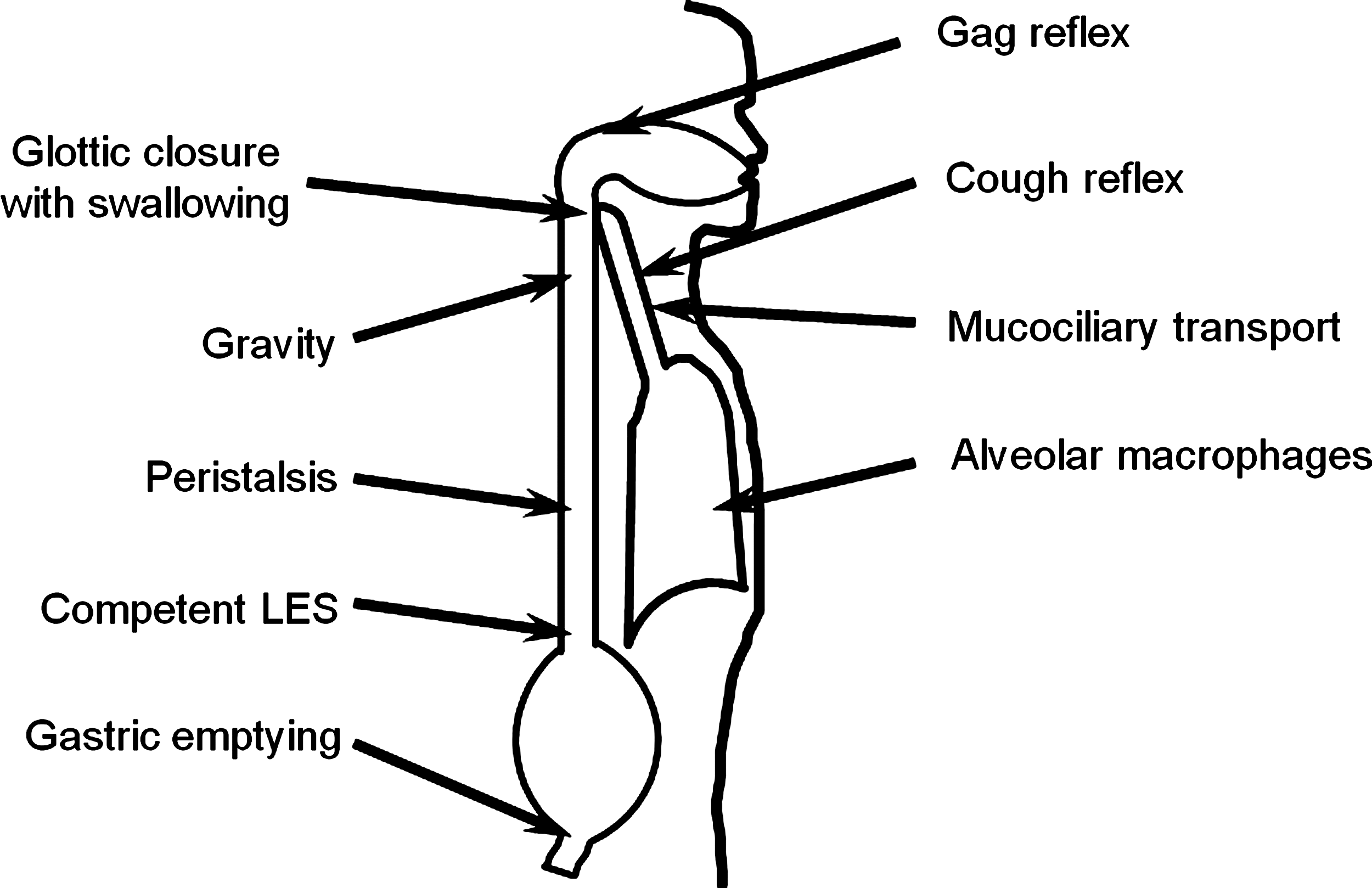
Host resistance mechanisms preventing pneumonia.
With critical illness or injury, pathophysiologic processes can interfere with those baffle mechanisms. Similarly, several therapeutic tactics employed in patient care can promote tracheal micro-aspiration. For example, many (if not most) critically ill patients have immunodeficiencies (known collectively as immunoparalysis) that can cripple the ability of pulmonary macrophages and other immunocytes to clear any inhaled organisms from alveoli [19,20]. Also, many ICU patients have gastrointestinal (GI) dysmotility from a variety of causes, such as opioids, bowel edema, or gut hypoperfusion [21,22]. The net result of sluggish GI motility (if not overt ileus) is the progressive overgrowth of the luminal microbial flora [23], analogous to a “backed up” household septic drainage system.
When critically ill patients are placed supine, which is a universal practice, gravity no longer facilitates the normal drainage of posterior pharyngeal secretions or particulates to the stomach, as happens in the normal upright human being. The common practice of placing nasogastric (NG) tubes may seriously worsen the situation, and increase the quantity of fluid and flora in the posterior pharynx. The presence of an NG tube likely interferes with esophageal peristalsis, in that clumps of material that normally would be “milked” downstream by peristalsis can adhere to the tube and stay resident in the esophagus, providing an excellent nidus for bacterial growth [24].
As mentioned previously, there is dense bacterial colonization of the posterior pharynx. The malfunction of normal drainage mechanisms and pooling of secretions add to this phenomenon substantially in the critically ill or severely injured patient. The cuffed endotracheal tube does not appear to be a substantial barrier to the aspiration of contaminated secretions into the tracheobronchial tree; indeed, secretions may pool between the vocal cords and the cuff, where they cannot be suctioned without a specialized endotracheal tube, and pose a continuous risk of aspiration. Using such a tube appears to decrease the risk of VAP [25]. There is a large body of literature, including the current consensus guidelines from the American Thoracic Society and the Infectious Diseases Society of America, that considers chronic micro-aspiration of oropharyngeal organisms via capillary action around the endotracheal tube cuff to be the primary route of bacterial colonization of the lower respiratory tract in endotracheally intubated patients [11,26–31].
Therefore, critically ill intubated patients have a number of assaults on the anatomic and physiologic processes that normally keep bacteria from entering the trachea or staying in the airways for any meaningful period of time. As a consequence, the incidence of pneumonia in ICU patients ranges from 7% to more than 40% [32,33]. Patients with VAP have a mortality rate that can exceed 50% [11]. In a case-control study, Fagon et al. identified an increase in the mortality rate of 27% attributable to VAP [33], but Heyland et al. were able to attribute death from VAP only to critically ill medical patients, not their surgical counterparts [34].
Development of Selective Digestive Decontamination
Because of overwhelming evidence that VAP develops from aspiration of oropharyngeal organisms, SDD using poorly absorbed antimicrobials has been suggested. Its first use was reported by Stoutenbeek et al. in 1983 [35] and again in 1984 [36]. Those investigators described the benefits of oral and parenteral antimicrobial decontamination in ICU trauma patients who required mechanical ventilation. Their regimen consisted of: (1) A sticky oral paste (Orabase) containing polymyxin E (2%), tobramycin (2%), and amphotericin B (2%); and (2) a suspension administered via a gastric tube containing the same antimicrobials (polymyxin E 100 mg, tobramycin 80 mg, and amphotericin B 500 mg). In addition, intravenous cefotaxime was administered until potential pathogenic microorganisms were eliminated (at a mean of 9 days); frequent surveillance cultures were obtained from multiple body sites to assess for microbial eradication. However, this was not a randomized trial; instead, the intervention group was compared with a historical control group. The control group presented with an oropharyngeal colonization rate of 63% that increased to 86% and 81% in those patients remaining hospitalized after 15 and 21 days, respectively. However, the patients who received SDD had an initial oropharyngeal colonization rate of 41% that decreased to zero at both 15 and 21 days. Importantly, it appeared that the protocol reduced the overall incidence of nosocomial infection from 81% to 16% (p < 0.001), with the incidence of VAP being reduced from 59% to 8% (p < 0.001).
Since that initial report, several other studies have been conducted on the use of SDD as a preventive measure in ICU patients, reaching various conclusions. At the time of this writing, a PubMed query for “selective decontamination digestive” yielded 70 randomized, controlled trials of SDD with topical ± intravenous (IV) antibiotics. A variety of antimicrobial regimens were used, with the most common listed in Table 1.
Because of the complexity of the cases in which SDD would be appropriate, Idemyor stated that “it would be difficult to conduct a multi-center, double-blind, placebo-controlled study that would help determine the effects of selective gut decontamination on the length of ICU stay, overall mortality rate, and the ecology of the colonizing bacteria” [37]. Nevertheless, a recent study by de Smet et al. appears to step up to that challenge [38]. They evaluated the effectiveness of SDD (and selective oral decontamination only; SOD) in a crossover study using cluster randomization in 13 ICUs in the Netherlands. Patient eligibility included expected duration of intubation of more than 48 h or an expected ICU stay of more than 72 h. The different regimens of SDD, SOD, and standard care were applied in random order over six months in each ICU. The SDD regimen consisted of four days of intravenous cefotaxime and topical application of tobramycin, colistin, and amphotericin B in the oropharynx and stomach, whereas the SOD protocol consisted of oropharyngeal application only of the same antibiotics. In addition, monthly point-prevalence studies were performed to analyze for the emergence of antibiotic resistance. A total of 5,939 patients were randomized to one of the three regimens (standard care 1,990 patients; SOD 1,904 patients; SDD 2,045 patients). The crude mortality rate at day 28 (the study's primary endpoint) was 27.5% in the standard care group, 26.9% in the SDD group, and 26.6% in the SOD group. The odds ratio (OR) for death by day 28 (vs. standard care) was 0.86 for the SOD group (95% confidence interval [CI] 0.74, 0.99) and 0.83 (95% CI 0.72, 0.97) for the SDD group. The authors noted a significant reduction in bacteremia attributable to Staphylococcus aureus, glucose-non-fermenting gram-negative bacilli (Pseudomonas aeruginosa, Stenotrophomonas maltophilia, and Acinetobacter spp.), and the Enterobacteriaceae. They also saw a significant reduction in the percentage of patients with at least one episode of bacteremia or fungemia, from 9.3% for the standard treatment group to 6.5% and 4.3% in the SOD and SDD groups, respectively. Importantly, despite the heavy use of prophylactic agents with SDD and SOD, the rate of bacterial resistance was consistently less than 5% and even lower for multi-drug-resistant strains. Whereas the study demonstrated significant differences in the mortality rate in the decontamination and standard care groups, the differences do not appear to be meaningful clinically. However, the authors noted that with a baseline rate of death during the first 28 days of 27.5%, the absolute and relative reductions in mortality at 28 days were 3.5% and 13%, respectively, for the SDD group and 2.9% and 11%, respectively, for the SOD group. They determined that it would be necessary to treat 29 patients with SDD to prevent one death (34 patients for SOD).
Concerns over SDD
Selective decontamination has been used extensively in Europe since its introduction, and most studies are European. However, the practice is not accepted widely in the U.S. because of the large variations in decontamination regimens and the incidence of infections in ICU patients in the various studies, making it difficult to assess the absolute impact of SDD as a result of what may be considered a low signal-to-noise ratio. In addition, concern has been expressed over the potential for the emergence of bacterial resistance. Daschner reported that patients receiving an SDD regimen can develop highly resistant infections [39]. Blair et al. noted a change in the ecology of the environmental and colonizing bacteria, although the emergence of multi-resistant strains was not a problem [40].
Importantly, most trials have ignored the pharmacoeconomic impact of SDD regimens. A key concern in the use of antimicrobials as prophylaxis is whether the expense is warranted. After all, in most cases, the patient does not have an infection at the time of initiation of SDD, so some justification is needed. Unfortunately, the proportion of SDD studies that analyze costs is relatively limited. Markowsky and Christie determined that the weekly costs range from $55 to $11,550 [41]. In a double-blind, placebo-controlled trial that demonstrated no advantage to SDD, Gastinne et al. reported that overall antibiotic charges averaged $1,287 ± $1,368 in the SDD group compared with $588 ± $1,051 in the placebo group (p < 0.001) [42]. In another double-blind, placebo-controlled trial that failed to show benefit, Hammond et al. determined that the average SDD antibiotic cost was approximately $500 and the average cost of treating infections in the SDD group was approximately $400 compared with $250 in the placebo group [43]. In a randomized trial of SDD in liver transplant patients, van Enckevort et al. found no difference in infection rates but an additional cost of $3,100 in the SDD group for the antibiotics and routine cultures [44]. It is interesting that the prospective trials that find little benefit from SDD are also those that investigate the costs of the program.
Systematic Reviews and Meta-Analyses
A number of reviews have consolidated the results of various clinical trials of SDD. At the time of this writing, PubMed returned 11 English-language publications filtered by “selective AND digestive AND decontamination” in the title and restricted to meta-analyses. However, review of the manuscripts showed that several do not describe sound science. A review by van Saene et al. examined 20 trials, consisting of 17 controlled studies and three observational cohort studies [45]; of the controlled studies, 16 demonstrated a significant reduction in secondary endogenous infection, but no odds ratios or confidence intervals were reported. Another report, by Sun et al. [46], is not itself a meta-analysis but rather an analysis of another meta-analysis [47]. Similarly, a study by van Nieuwenhoven et al. [48] assesses the methodologic quality of clinical trials of SDD, but does not actually provide a meta-analysis. Two meta-analyses by Silvestri et al. assessed the impact of SDD only on fungal infections [49] and general bacterial infections [50] but did not specifically evaluate the effect of SDD on overall VAP or mortality rates.
The remaining six studies are included in Tables 2 and 3, along with meta-analyses detected through other searches [51–56]. One of these is a recent meta-analysis and systematic review that came to the conclusion that oral decontamination with chlorhexidine was effective in reducing the incidence of VAP but not mortality, and was more effective than SDD with antimicrobials [57]. This is one of the references used to justify the addition of daily oral hygiene with chlorhexidine as a fifth component of the ventilator bundle [2].
Risk difference (Pc-Pt).
RCT = randomized controlled trial; RTI = respiratory tract infection; Abx = antibiotics.
Risk difference (Pc-Pt).
RCT = randomized controlled trial; Abx = antibiotic.
Boldface = favors reduction in mortality.
Impact of SDD on mortality rate
One of the major criticisms of SDD has been that there is no demonstrated impact on mortality. Earlier estimates indicated that in order to demonstrate a reduction in the mortality rate of 10%–20%, a study would have to include between 2,000 and 3,000 patients [47]. A few small studies have documented a decrease in the overall mortality rate with SDD regimens [58–60], but other, larger studies failed to show a mortality impact. A meta-analysis by Silvestri et al. evaluated 21 randomized, controlled trials of 4,902 patients. The investigators noted that the overall mortality rate was, in fact, reduced significantly (OR 0.71; 95% CI 0.61–0.82; p < 0.001) [61]. There were 481 deaths in the SDD group (19.9%) compared with 634 among control patients (25.5%). Subgroup analysis revealed a significant mortality reduction in those patients who were decontaminated successfully (OR 0.58; 95% CI 0.45–0.77; p < 0.001). Mortality reduction also was demonstrated when parenteral and enteral antimicrobials were administered to every patient in the intensive care unit (OR 0.59; 95% CI 0.42–0.82; p < 0.001). The authors determined that one death could be prevented for every eighteen patients treated with SDD.
Similarly, a Cochrane review evaluated 36 trials involving 6,914 adult ICU patients who received SDD for prevention of respiratory tract infections (RTIs) and death [62]. The study determined that a combination of topical and systemic antibiotics produced a significant reduction in both respiratory tract infections, from 40% in controls to 19% in SDD-treated patients (no. of studies = 16; OR 0.28; 95% CI 0.20–0.38), and the total mortality rate, from 30% in controls to 24% in SDD-treated patients (no. of studies 17; OR 0.75; 95% CI 0.65–0.87). In trials comparing topical antimicrobials alone (or comparing topical plus systemic treatment vs. systemic alone), there was a significant reduction in respiratory tract infections, from 30% in controls to 21% in SDD-treated patients (no. of studies 17; OR 0.44; 95% CI 0.31–0.63), but there was no impact on the overall mortality rate, which was 26% in treated patients vs. 25% in the control patients (no. of studies 19; OR 0.97; 95% CI 0.82–1.16). Those investigators concluded that a combination of topical and systemic prophylactic antibiotics reduces respiratory tract infections and the overall mortality rate in adult ICU patients, and that topical prophylaxis alone reduces the incidence of respiratory infections but not the mortality rate. Also, they noted that the risk of resistance as a negative consequence of antibiotic use was appropriately explored in only one trial, which did not show any such effect.
Selective decontamination with antiseptics
Because of the variability and cost of antimicrobial-based SDD, a growing number of studies have evaluated the use of topical antiseptics for this purpose. Antiseptics act rapidly on multiple organisms through mechanisms that have rarely induced resistance.
DeRiso et al. conducted a randomized, double-blind, placebo-controlled trial of 353 patients undergoing open heart operations (excluding transplantation) to receive a twice-daily oral rinse of 0.12% chlorhexidine or placebo [63]. They noted a 69% reduction in the incidence of total respiratory tract infections in the chlorhexidine-treated group (17/180 vs. 5/173; p < 0.05). Moreover, there was a reduction in the overall nosocomial infection rate by 65% in the chlorhexidine-treated group (24/180 vs. 8/173; p < 0.01), as well as a reduction in the mortality rate (1.16% vs. 5.56%). The use of non-prophylactic IV antibiotics was decreased by 43% (42/180 vs. 23/173; p < 0.05), and there was no change in bacterial resistance patterns. Subsequently, studies with similarly favorable results were reported by Segers et al. [64], Houston et al. [65], Genuit et al. [66], Bopp et al. [67], Koeman et al. [68], Fourrier et al. [69], Tantipong et al. [70], and Cabov et al. [71].
These nine studies favorable to chlorhexidine oral rinses are countered by three randomized, controlled trials that failed to show benefit. One such study, by Bellissimo-Rodrigues et al., did not find benefit with 0.12% chlorhexidine oral rinses compared with placebo [72]. A subsequent prospective, double-blind, placebo-controlled study performed by Fourrier et al. did not show a reduction in pneumonia rates with the use of 0.2% chlorhexidine rinses [73]. Similarly, Panchabhai et al. found no benefit from 0.2% chlorhexidine rinses [74].
Three meta-analyses evaluate the use of chlorhexidine (Tables 2 and 3). Two demonstrated a favorable effect of oral rinses for VAP [57,75], whereas one did not [76]. There has been some discussion of whether stronger concentrations of chlorhexidine (i.e., 2.0%) should be used, as they seemed to be more consistently effective in clinical trials. However, there is concern about adverse patient effects (i.e., mucosal irritation and a bitter taste) with the higher concentration [77].
A study by Seguin et al. explored the use of an antiseptic other than chlorhexidine for SDD [78]. Ninety-eight head-injured, mechanically ventilated patients were randomized to naso- and oro-pharyngeal rinsing every 4 h with either 60 mL of a dilute aqueous povidone-iodine solution (36 patients) or 60 mL of saline (31 patients), followed by aspiration of oro-pharyngeal secretions. The investigators compared these two regimens with aspiration of oropharyngeal secretions every 4 h without naso- or oro-pharyngeal rinsing (31 patients). There were only three VAP cases in the povidone-iodine group (8%), compared with 12 in the saline group (39%; p = 0.003) and 13 in the control group (42%; p = 0.001). This study corroborated the results of the studies that used chlorhexidine [63,68,69].
Conclusions
Despite reasonably sound evidence accrued over nearly 30 years that SDD reduces the rate of pneumonia and, more recently, that it reduces the mortality rate, the practice has yet to become the standard of care in American ICUs. High cost, emerging resistance, and labor intensity have been cited as reasons for this lack of adoption. Most available data support the concept that SDD with either antibiotics or antiseptics reduces the overall incidence of nosocomial pneumonia. There also is a growing body of literature in support of the position that SDD may reduce mortality rates, especially if parenteral antibiotics are administered with the topical regimen. It has been difficult for any investigator to identify any impact on microbial resistance patterns, although a more prevalent experience over a longer term may prove otherwise. The costs of SDD or SOD can be offset only if it results in less therapeutic antibiotic use. It also is apparent that topical antiseptics (either chlorhexidine or povidone-iodine) for SDD may be more effective with less expense and less potential for resistance than antibiotic-based SDD regimens.
The recent inclusion of chlorhexidine oral rinses in the ventilator bundle by the IHI may mean that effective SDD will become standard. However, it remains unclear whether the 0.12% concentration recommended by the IHI is adequate to be effective, given that it is the most dilute strength that has been tested. It will be interesting to see if increasing experience with oral decontamination will lead to even more effective protocols, with the ultimate goal of bringing the VAP incidence down to zero.
Footnotes
Author Disclosure Statement
No conflicting financial interests exist.