
Abstract
Abstract
Background:
The Surgical Infection Society Guidelines for the treatment of complicated skin and soft tissue infections (SSTIs) were published in October 2009 in Surgical Infections, and an overview of these guidelines was provided at the Thirtieth Annual Meeting of the Society. A summary of this overview is provided.
Methods:
Review of relevant papers related to complicated SSTIs published between 1966 and 2008 with graded recommendations and summations of general epidemiology and recommendations.
Results:
The frequency of SSTI has increased over the past decade, predominately because of an increase in infections caused by community-acquired methicillin-resistant Staphylococcus aureus. Drug resistance is increasing among all pathogens. A total of 61 graded recommendations were made in the complete guidelines, 28 of which are presented here, separated into those for non-necrotizing and necrotizing infections.
Conclusions:
Appropriate antibiotic therapy should be provided in complicated SSTIs. Early diagnosis and treatment of necrotizing infections is paramount, as time to therapy alters morbidity and mortality rates.
RCT = randomized controlled trial.
The final SIS Guidelines contain 61 total graded recommendations. However, because of the lack of adequate studies and data, only four level “A” recommendations could be made, whereas 49 level “C” recommendations were made. When considering risk vs. benefit, 52 strong (1) and 9 weak (2) recommendations were made. The guidelines deal exclusively with those SSTIs considered “complicated” under the U.S. Food and Drug Administration (FDA) classification [3]. Most SSTIs, managed by surgeons are complicated. The FDA definition of complicated SSTIs includes those that are deep or necrotizing, usually requiring surgical intervention, including infected ulcers, infected burns, and major abscesses; that occur in patients with specific major co-morbidities; and that necessitate hospitalization. Thus, the definition excludes all superficial skin infections without necrosis and those abscesses that can be treated by incision and drainage alone. The expert panel specifically chose the term “skin and soft tissue infection” rather than the FDA term “skin and skin structure infection,” as necrotizing infections may involve the deep fascia and muscle, tissues not considered part of the skin structure (Fig. 1). For all randomized studies of therapeutic agents in SSTIs, necrotizing infections are specifically excluded. Thus, recommendations are extrapolated from studies of non-necrotizing infections.
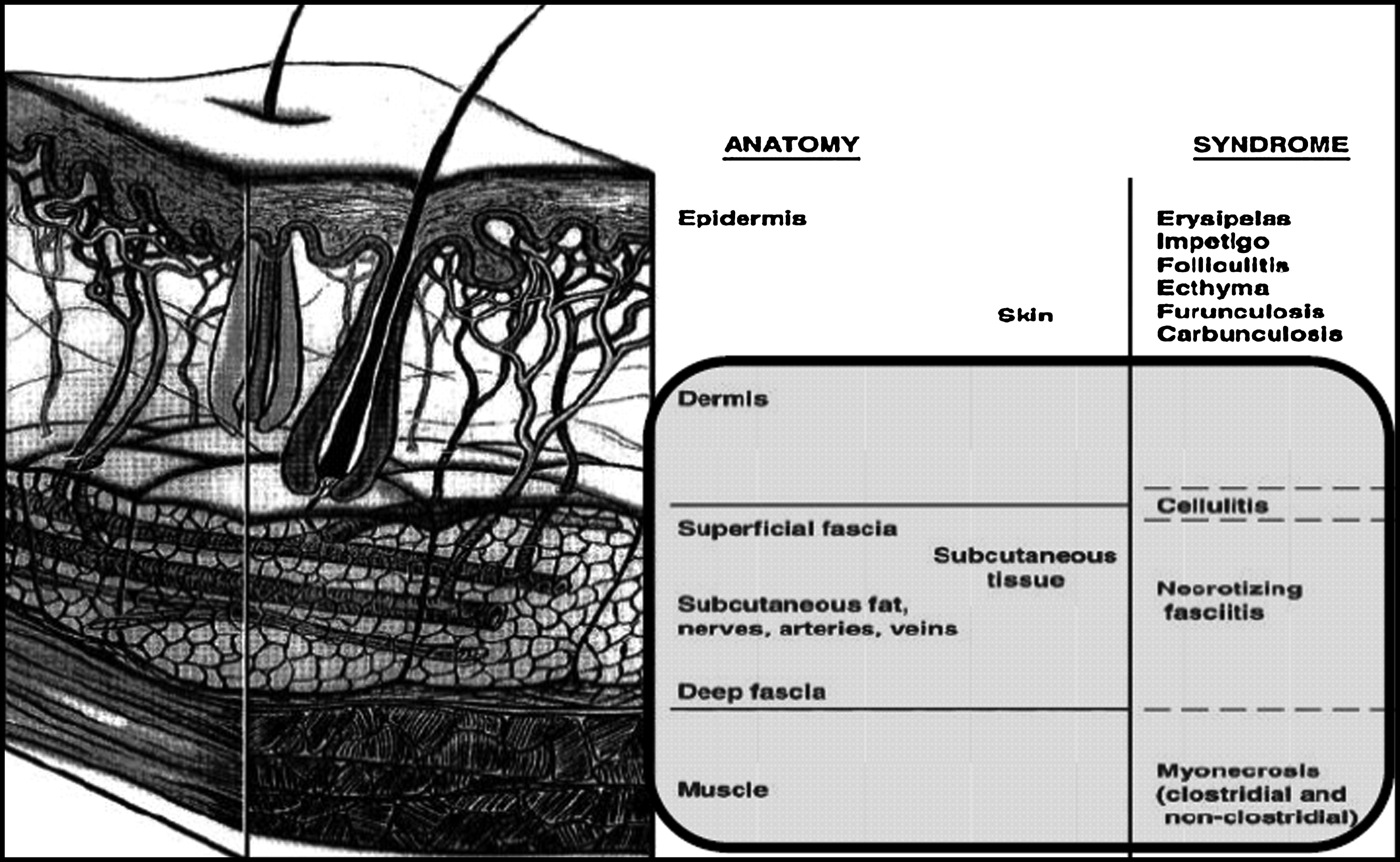
Focus of Surgical Infection Society skin and soft tissue infection guidelines.
Table 2 provides an outline of the complete guideline contents. The total document is 32 pages in length and contains 344 references. For this summary, abbreviated recommendations are presented in two categories: Non-necrotizing and necrotizing infections. For non-necrotizing infections, the epidemiology of complicated SSTI and the treatment of non-necrotizing cellulitis and complicated abscesses are discussed. For necrotizing infections, epidemiology, diagnosis, and treatment are discussed with a focus on rapidly progressing necrotizing SSTIs.
The epidemiology of complicated SSTIs has changed somewhat in the last decade. As shown in Figure 2, the frequency of SSTI has increased significantly since the late 1990s, predominately because of an increase in infections caused by community-associated methicillin-resistant Staphylococcus aureus (MRSA) [4]. Staphylococcus aureus remains the most common pathogen isolated from complicated SSTIs. Table 3 provides the rank order of bacterial pathogens isolated from SSTI [5]. These data come from the SENTRY Program, which includes 5,800 consecutive patients admitted to hospitals in Canada and 32 states in the U.S. and includes both community- and hospital-acquired infections. In these data, S. aureus accounts for greater than 40% of all isolates, with Pseudomonas aeruginosa being the second most common isolate at 11%. Over the period from 1998 to 2004, the number of SSTI pathogens resistant to at least one antibiotic increased for S. aureus, Enterococcus spp., P. aeruginosa, Escherichia coli, and Klebsiella spp., with nearly 50% of the S. aureus isolates now being resistant to methicillin [5]. The epidemiology of surgical site infections (SSIs) is slightly different, with an even greater shift toward gram-positive pathogens (S. aureus, coagulase-negative staphylococci, and Enterococcus spp.—greater than 50% of isolates) [6]. In this population of patients, MRSA isolates now equal or exceed methicillin-sensitive strains of Staphylococcus. Graded treatment recommendations for complicated, non-necrotizing SSTIs are presented in Table 4.

Increasing frequency of skin and soft tissue infections. Reprinted with permission from Pallin DJ, Egan DJ, Pelletier AJ, et al. Increased U.S. emergency department visits for skin and soft tissue infections, and changes in antibiotic choices, during the emergence of community-associated methicillin-resistant Staphylococcus aureus. Ann Emerg Med 2008;51:291–298.
MRSA = methicillin-resistant Staphylococcus aureus.
Alphanumerics in parenthesis refer to grading (see Table 1).
Necrotizing SSTIs are discussed separately for several reasons. These infections are greater in severity and may involve a different spectrum of pathogens than non-necrotizing infections. Because of the severity and rapidity of progression, establishing an accurate diagnosis and instituting timely appropriate antibiotic therapy and surgical debridement is of much greater importance. Unfortunately, no randomized or large, well-designed non-randomized studies exist to help establish therapy of necrotizing SSTIs. The overall mortality rate for necrotizing SSTI remains significant (∼24% overall), ranging from 9%–73% in 67 studies published between 1980 and 2008 [7]. Because of the severity and specific pathogenicity, these infections frequently involve deeper layers of tissue, including the deep dermis, subcutaneous fat, fascia, and muscle.
Necrotizing infections may be divided into two categories: Those caused by a mixture of pathogens and those involving a single more virulent pathogen that have rapidly progressive courses. Necrotizing SSTIs caused by mixed pathogens are more common and typically arise from an inciting source that may have been indolent, including peri-rectal infections, colonic pathology, intravenous drug use, trauma, chronic diabetic ulceration, and SSIs. Such mixed infections involve an average of four organisms and typically spread along the fascia and fascial planes where the blood supply is tenuous [8]. In contrast, infections that are rapidly progressive involve pathogens that are more virulent, typically producing exotoxins that contribute significantly to the pathogenesis of the infection. These infections are characterized by rapid clinical deterioration and fast spread through tissues. Fortunately, such infections are rare, as they have a high mortality rate. Both gram-positive and gram-negative pathogens may cause infections of this nature, the most common being Group A Streptococcus, Clostridium spp., community-acquired MRSA, Vibrio spp., Aeromonas hydrophilia, and Pasteurella spp.
Table 5 includes the graded recommendations for the diagnosis and treatment of necrotizing SSTI. Delays in diagnosis contribute to delays in appropriate antibiotic and surgical therapy, leading to greater morbidity and a higher mortality rate. There are several signs and clinical findings that are fairly specific for necrotizing infection, but most occur late in the course of disease and are not highly sensitive. Thus, a high index of suspicion is mandatory, and in the presence of specific findings, exploration is warranted.
MRSA = methicillin-resistant Staphylococcus aureus.
See Table 1 for definitions of alphanumeric grades (in parenthesis).
Footnotes
Author Disclosure Statement
No conflicting financial interests exist.