
Abstract
Abstract
Background:
The prosthetic arteriovenous grafts (AVG) being used increasingly to create hemodialysis access are prone to infections that pose potentially life-threatening infectious and bleeding complications, as well as loss of dialysis access. In this study, we identified the bacteriologic agents of infected AVGs by site swab, blood culture, and prosthesis cultures, and to evaluate the role of microbiological findings in the management of the infection.
Methods:
We focused on 51 patients with 53 AVGs operated on in our clinic from January 2006 to December 2009. An infected AVG was identified by clinical, ultrasound, and microbiological findings. Sensitivity to antibiotics was determined for all bacterial strains. Isolates were identified by pulsed-field gel electrophoresis (PFGE) of bacterial DNA. In a few cases, positron emission tomography-computed tomography (PET-CT) examination was performed.
Results:
Strains of Staphylococcus spp., especially S. aureus, were the most frequent cause of infected AVG. All S. aureus strains were sensitive to methicillin. With the exception of a single case, isolates obtained simultaneously from the skin site and the vascular prosthesis were identical genetically.
Conclusions:
Our results suggest that bacterial infectious agents detected in site swab, blood, or graft culture confirm a suspicion of AVG infection. A PET-CT examination can provide confirmation. The combination of microbiologic and radionuclide findings can improve the management of the AVG infection, but surgery remains essential.
Infected vascular access for hemodialysis usually is caused by gram-positive bacteria, in particular, strains of Staphylococcus aureus, which are documented in as many as 68% of infections [10,11]. Gram-negative bacteria are an uncommon cause of infection, with a prevalence below 28% [10,12]. Infections caused by S. aureus may produce complications such as metastatic infection of bones, joints, endocardium, and brain. That is, the infected graft becomes a source of septic emboli, which circulate through the arterial system. These complications have been found in 12% of infected grafts [10], and the risk of death in patients with vascular graft infections caused by S. aureus is 13%–44% [13,14]. Methicillin-resistant S. aureus (MRSA) is a growing problem for dialysis centers, as it increases the 90-day mortality risk by 70% [15]. One risk factor for MRSA infection is previous use of antibiotics. There also has been an increase in the prevalence of vancomycin-resistant enterococci (VRE) in dialysis patients [18,19]. A likely cause is the increased use of antibiotics, especially vancomycin and third-generation cephalosporins [18,20].
The aim of this study was to identify the bacteriologic agents of infected AVGs in site swab, blood, and AVG cultures and to evaluate the role of microbiologic findings in the management of the infection.
Patients and Methods
Patients
All 1,221 patients who underwent creation/revision of their vascular access (AVF or AVG) in our clinic over the three-year period from January 1, 2006, to December 31, 2009, were included in a prospective study group. They were monitored regularly in the dialysis center and in our clinic for infection of their vascular access (local findings, laboratory tests including C-reactive protein concentration). These 362 male and 228 female patients were followed up twice a month for at least six months. Of 590 patients, 51 had AVGs (two of these had an AVG implanted in both arms) and the remainder AVFs.
An infected AVG was identified by clinical findings (clinical presentation was categorized as systemic sepsis, draining sinus tract, exposed graft, purulent drainage, erythema, pain overlying the graft, or hemorrhage), ultrasound examination, and cultures. Three patients whose body temperature was slightly above normal but who were not febrile (subfebrile condition) with pain over the graft prosthesis were investigated further by positron emission tomography-computed tomography (PET-CT). To confirm sepsis, a blood culture was obtained at least twice during followup. As the infected prosthesis was removed, site cultures always were collected perioperatively for microbiologic examination. The prosthesis was cultured.
Isolation and identification of bacteria
Bacterial strains were isolated from clinical materials (preoperative material, pus, blood, removed prosthesis) and identified by standard microbiologic methods and the Phoenix automated system (Becton Dickinson, Franklin Lakes, NJ).
Determination of sensitivity to antibiotics
Sensitivity to antibiotics was assessed using a standard dilution micromethod that met the Clinical and Laboratory Standards Institute (Wayne, PA) and European Union Committee on Antimicrobial Susceptibility Testing standards [21,22]. Reference strains Escherichia coli ATCC 25922, Escherichia coli ATCC 35218, and Pseudomonas aeruginosa ATCC 27853 from the American Type Culture Collection (Manassas, VA) were used for protocol quality control. The test for methicillin-resistant staphylococci by detection of penicillin binding protein (PBP) 2a was performed using the MRSA-Screen test (Denka Seiken Co., Tokyo, Japan). The PBP2a detection was confirmed by mecA gene detection using polymerase chain reaction (primers mecA-F: 5′-TCCAGATTACAACTTCACCAGG-3′ and mecA-R: 5′-CCACTTCATATCTTGTAACG-3′) [23] using a modified approach [24].
Determination of the identity of bacterial isolates
Molecular typing was performed by pulsed-field gel electrophoresis (PFGE) of bacterial DNA. Genomic DNA was isolated according to procedures described by Shi et al. and digested overnight with SmaI restriction endonuclease [25]. The PFGE was run in 1.2% gel for 24 h at 6 V/cm and pulse times of 2–35 s. After PFGE, the gel was stained with ethidium bromide (Sigma-Aldrich, St. Louis, MO) (1 mcg/mL) and examined under ultraviolet illumination. The acquired restriction maps of individual isolates were compared using the GelCompar II software and 1.0% tolerance Dice coefficients, and their relations were determined.
Results
Infectious complications were found in 15/53 (28.3%) AVGs and in 9/537 (1.7%) AVFs. In two patients, a prosthesis was implanted at different times on both upper limbs, which explains the 15 infected prostheses in 13 patients.
The most common presentations of infected AVG were draining sinus tract and afebrile condition (six patients). Purulent drainage, hemorrhage, and sepsis were found in three patients. In another three patients, the purulent secretion from the needle puncture site was treated surgically, and graft exposure was present. In all cases, there was pain overlying the graft as a manifestation of the infection. Duplex sonography was performed on all patients, and fluid around the graft was apparent in four patients as effusions around the prosthesis. For the rest, the ultrasonography findings had no utility in the diagnosis. In three patients with afebrile body temperature and pain over the graft, a PET-CT scan was performed. The examination showed increased accumulation of labeled glucose in the graft, and this was the basis for the revision and removal of the graft. Infected grafts were removed completely, and the arterial and venous anastomoses were treated surgically.
The most common infectious agents in AVGs were strains of Staphylococcus, constituting 86.7% of all agents. The most frequent species was S. aureus, which accounted for 53.8% of the isolates of staphylococci. Staphylococcus aureus was detected in seven cultures from graft site swabs and in one blood culture. The second most frequent species was S. epidermidis, detected in four cultures from site swabs, two blood cultures, and two AVG cultures. Staphylococcus haemolyticus and S. hominis were each detected in one site swab. Strains of Enterococcus faecalis and Pseudomonas aeruginosa were detected occasionally.
The sensitivity of the Staphylococcus isolates to selected antibiotics is given in Table 1. There was resistance to methicillin only in the case of S. epidermidis. The species P. aeruginosa, isolated as an etiologic agent in one patient, was sensitive to all antibiotics tested (piperacillin, aztreonam, meropenem, ceftazidime, cefoperazone, cefepime, gentamicin, amikacin, colistin, ofloxacin, and ciprofloxacin). Enterococcus faecalis, which was found in postoperative material and at the same time in removed AVGs, was sensitive to ampicillin, chloramfenikol, erythromycin, nitrofurantoin, tigecycline, vancomycin, teicoplanin, and linezolid.
CIP=ciprofloxacin; CLI=clindamycin; CMP=chloramphenicol; COT=co-trimoxazole; ERY=erythromycin; GEN=gentamicin; LNZ=linezolid; MET=methicillin, PEN=penicillin; TEI=teicoplanin; TET=tetracycline; TIG=tigecycline, VAN=vancomycin.
Determination of the identity of the isolates obtained from the same patient in different clinical materials by comparing the genomic DNA via restriction maps showed that the strains isolated from site swabs taken during the surgery and in blood and vascular prostheses were identical (similarity>95%) (Table 2). The only exception was one patient with S. epidermidis isolated from the graft site and blood that were genetically different, but if the isolates were obtained at the same time from the site and the vascular prostheses, they were always identical (Fig. 1).
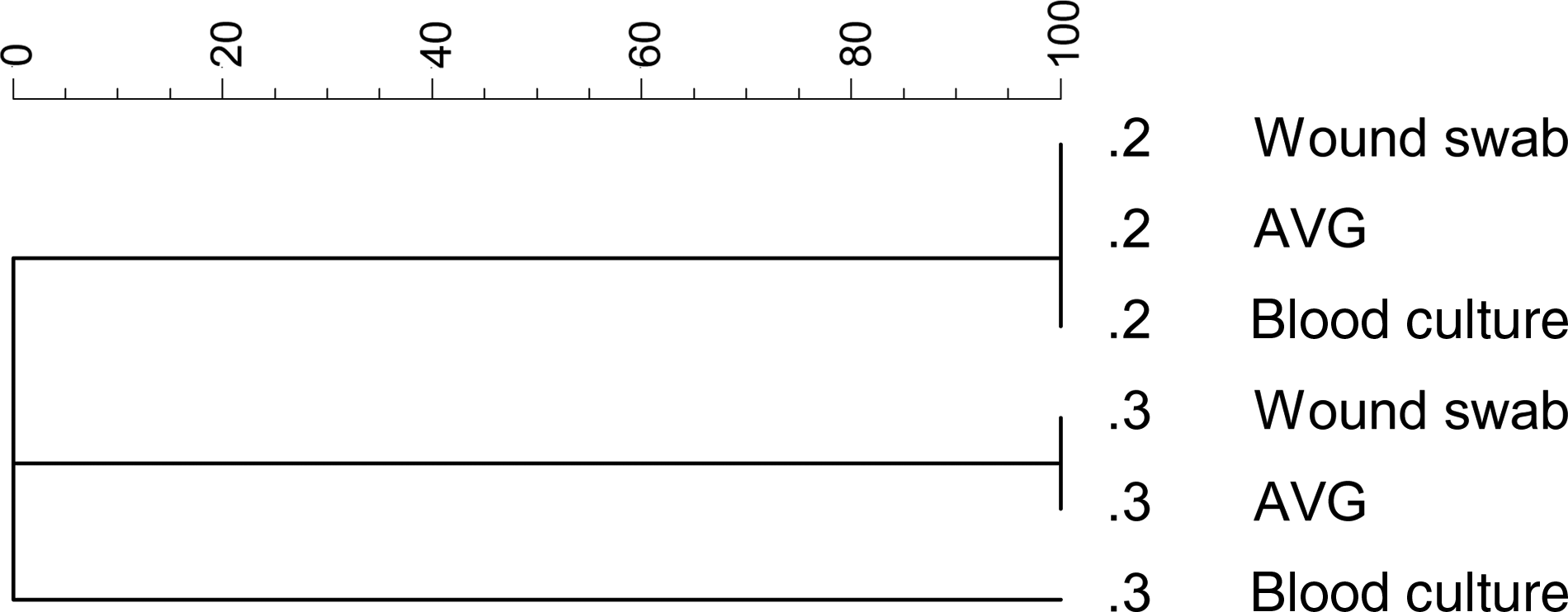
Two strains isolated from graft site swab, arteriovenous graft (AVG), and blood culture are identical. Three strains isolated from graft site swab and AVG are identical; strain from blood culture is different.
Discussion
In Europe, infected fistulas require comprehensive management, as in most cases, the patient has exhausted autologous venous circulation, and an AVG is the only option for ensuring access for dialysis without central venous cannulation. The infection carries the threat of both local and systemic complications. Risk factors for graft infection are numerous. Infections may occur at the graft site (the lower limb is infected more often) because of the lack of asepsis during implantation (cannulation techniques themselves involve the risk of infection), hematoma formation, or clogging. Obviously, the longer the graft is used, and the more often it is cannulated, the greater the risk of infection. In patients prone to infection and subsequent graft involvement, there obviously are a number of other factors, including immunosuppression resulting from neutrophil dysfunction, uremia, patient obesity, diabetes, hypoalbuminemia, and poor personal hygiene. Another risk factor is human immunodeficiency virus (HIV) infection. Implants, as with all other vascular prostheses, are prone to infections caused by penetration of the hematogenous route. The experience with AVG confirms the well-known experience in vascular surgery. Antibiotic treatment can suppress the symptoms of infection, but it cannot eradicate infection of a vascular prosthesis. Proved infection in 28% of AVGs, which resulted in removal of the graft and termination of access to dialysis, must be considered a high prevalence. In our clinic, we prefer to remove infected AVGs completely, in accordance with the recommendation of Ryan et al. [11].
Dialysis patients are hospitalized twice as often as the normal population, and the cause of hospitalization is infection in 20% [26]. The majority of infections are attributable to routine dialysis. Repetitive breaks in skin integrity allow infection to reach the AVG. Bacteria adhere more strongly to the synthetic material of the AVG, leading to resistance of the host defences compared with native AVFs [27,28]. This is confirmed by our experience. In 60% of patients, the infection occurred at the site of the AVG needle insertion. There was erosion of overlying skin and secretion from the site, sometimes leading to graft exposure.
Three afebrile patients with pain over their graft prosthesis were investigated by PET-CT. The examination showed increased accumulation of labeled glucose around the graft in all cases, and the grafts were revised. In two cases, infection was shown, and the prostheses were removed. In one case, there was a concurrent perigraft reaction [29], and the graft was retained. When infection was confirmed by culture, however, the graft was removed. The equivocal local findings related to temperature in these patients with infected AVGs caused us to consider investigation of leukocyte markers or using PET-CT. The PET-CT method is easier and more accurate than the method using indium-labeled leukocytes [27,30]. Owing to limited experience with these methods, however, we were unable to distinguish the perigraft reaction from AVG infection. The real contribution of these technologies to the problems of infected hemodialysis grafts is difficult to evaluate, as only one recent study has been published.
Epidemiologic data demonstrate that the type of vascular access for hemodialysis affects the overall chance of infection significantly [28,31]. The highest risk is with a common central venous catheter, followed by tunnelized catheter or arteriovenous graft; the least risky is an autologous fistula. Infected AVGs have been found in 11%–35% of patients [4]. Infectious complications that have their origin in grafts are about one-third more common than complications of autologous fistulas [32].
Our results showed that strains of Staphylococcus, especially S. aureus, were the most frequent cause of infected AVGs. The fact that the most frequent etiologic agent of AVG infections was Staphylococcus spp. strains is attributable to their ability to form a biofilm. Biofilm analysis was not a part of this study. One positive finding was that there were no cases of MRSA. Our teaching hospital applies a strict antibiotic policy, described by Kolar and Latal [33]. In short, the application of antibiotics requires the approval of the center for antibiotic control, which is part of the Department of Microbiology. This restriction is for both individual patients and epidemiologic study. The microbiology department examines the most common bacterial pathogens resistant to antimicrobial agents. In 2010, the frequency of MRSA strains was <1% (unpublished data), and these results are reflected in the present study. For this reason, we were able to use common antibiotic agents effective against S. aureus, namely methicillin/oxacillin, in our patients.
The antibiotic treatment of AVG infections has a major impact on morbidity in dialysis patients and requires a comprehensive approach, from prevention through to diagnosis and treatment. All measures that reduce the incidence of infection represent patient benefits and reduce the cost of vascular access for dialysis.
Over the past 30 years, since AVGs were introduced, there have been no improvements in their long-term patency. The best replacement remains the ePTFE graft. Preimplantation conditions must be created with the suppression of infectious sources, but it is clear that these steps will lead to the selection of resistant bacteria. Preserving the sterility of a prosthesis requires compliance with safeguards. The diagnosis of infection usually is made on the basis of the clinical findings. Our results suggest that bacterial agents detected in graft site swab, blood, or AVG culture confirm the suspicion of AVG infection. Further confirmation can be provided by PET-CT examination. The combined microbiologic and radionuclide findings can facilitate decision making.
The principle of therapy remains unchanged. Essentially, it is surgery. The radicality of surgical treatment of prosthesis infection depends on the experience of individual centers, but the general view is that it is safer to remove all the infected prostheses and provide access to dialysis via a central venous catheter. The length of use and functionality of the prosthesis also can influence decisions about the extent of the surgery. In the case of repeatedly revised prostheses for stenotic and thrombotic complications or suspected infection, it is better to remove the prosthesis completely. The sensitivity of the isolated bacterial pathogen to antimicrobial agents should be determined, and the antibiotic treatment should targeted to the particular bacterial strains isolated.
Footnotes
Acknowledgment
This work was supported by grants IGA NT 11062-5/2010 and MSM6198959205.
Author Disclosure Statement
No competing financial interests exist.