
Abstract
Abstract
Background:
Surgical site infection (SSI) is the fourth commonest healthcare-associated infection and complicates at least 5% of open operations. In a randomized clinical trial, antimicrobial-coated sutures were compared with their conventional counterparts, polyglactin and poliglecaprone, for skin closure after breast cancer surgery to assess their role in reducing the rate of SSI.
Methods:
Between November 2008 and February 2011, 150 female patients presenting with breast cancer to a single center were randomized to skin closure with antimicrobial-coated or plain sutures. Postoperatively, SSI was defined using the U.S. Centers for Disease Control and Prevention (CDC) definitions and scored using the ASEPSIS or Southampton systems by trained, blinded observers with close post-discharge surveillance and patient diaries. Surgeons and patients were blinded to the type of suture used.
Results:
Using CDC criteria, the overall rate of SSI was 18.9% at six weeks. Six patients (4.7%) needed intervention or readmission for SSI. Skin closure with antimicrobial sutures showed a non-statistically significant reduction in the SSI rate, to 15.2%, compared with conventional sutures (22.9%). A uniform tendency for fewer SSIs in the antimicrobial-coated suture group was found using ASEPSIS and Southampton scores, but again, the difference was not statistically significant.
Conclusion:
The previously reported high rate of SSI related to breast surgery was confirmed. Using statistical modeling and earlier reports, the study was powered to show a difference using ASEPSIS scores, but the modification used in this trial failed to find a difference. Finding a statistically significant difference would have needed two to three times the number of patients recruited. Further evaluation of antimicrobial-coated sutures is merited, particularly if used as part of a care bundle to reduce SSI after breast cancer surgery.
Breast surgery is classified as “clean,” with the expectation of a low SSI rate. If close post-discharge surveillance is undertaken, this figure has been estimated to be as high as 15%–20% using strict U.S. Centers for Disease Control and Prevention (CDC) definitions [1,10] (the most widely applied in SSI research), which give categorical data, or systems such as ASEPSIS [11] or the Southampton wound score [12], which give interval data that help to determine the severity of SSI. The ASEPSIS score assigns points for
The reasons for the high rate of SSI after breast surgery are not clear but may be related to the breast containing epithelial ductal tissue with microbial contamination or poor healing relating to blood supply, residual hematomas or seromas, or acute biofilm formation. The value of antibiotic prophylaxis also is contentious in clean, non-prosthetic surgery [13,14]. Low reported SSI rates after breast surgery may reflect an increasing trend for this surgery to be undertaken as a day case, poor post-discharge surveillance, and the specific definitions applied. An SSI after breast cancer surgery may lead to a distressing delay when there is need for adjuvant chemotherapy or radiotherapy.
Guidelines to prevent and treat SSI have been published by the National Institute of Health and Clinical Excellence (NICE) [15–17], with key recommendations being incorporated into a high-impact intervention, the care bundle from the Department of Health [18]. Research recommendations in the NICE document include a wider appraisal of the potential of antiseptics. In this randomized controlled clinical trial, the value of antimicrobial-coated absorbable sutures in breast cancer surgery was evaluated.
Triclosan (2, 4, 4′-trichloro-2′-hydroxydiphenyl ether) is a broad-spectrum biocide that has been used safely for more than 30 years in various products such as toothpaste and soap [19–23]. Its mode of action is through multiple non-specific cytoplasmic and membrane targets. Triclosan also is an inhibitor of the FabI gene, which encodes enoyl-acyl carrier protein reductase, essential in fatty acid biosynthesis, thus blocking bacterial fatty acid synthesis [24]. Its action as an antiseptic, coated on or impregnated into synthetic absorbable polymer sutures, has been investigated in several experimental and clinical studies [25–33].
In this randomized controlled trial, the effect of triclosan coating of polyglactin and poliglecaprone sutures for skin closure after elective breast cancer surgery was assessed. The trial is reported using the updated CONSORT guideline for randomized trials [34].
Patients and Methods
In the period November 2008 to February 2011, women older than 18 years of age having breast cancer and undergoing primary elective surgery under the care of two breast surgeons (HS, SG) at the Cardiff and Vale National Health Service (NHS) Trust (single center) were invited to participate in the randomized controlled trial summarized in Figure 1. The trial was approved by the NHS Research Ethics Committee (South East Wales Research Ethics Committee), and patients were informed of the trial as outpatients when their diagnosis of breast cancer and surgical planning was confirmed. After an assessment of their eligibility, they were approached separately on the day prior to surgery by other members of the trial group (NW, NI, or DJL) and invited to join the trial after written informed consent was given with comprehension of an information sheet. The exclusion criteria were inflammatory breast cancer or skin ulceration; neo-adjuvant chemotherapy or radiotherapy; surgery for benign or reconstructive reasons; known immune deficiency or allergy to triclosan; and inability to give consent or suspicion that the patient was unlikely to comply with followup.
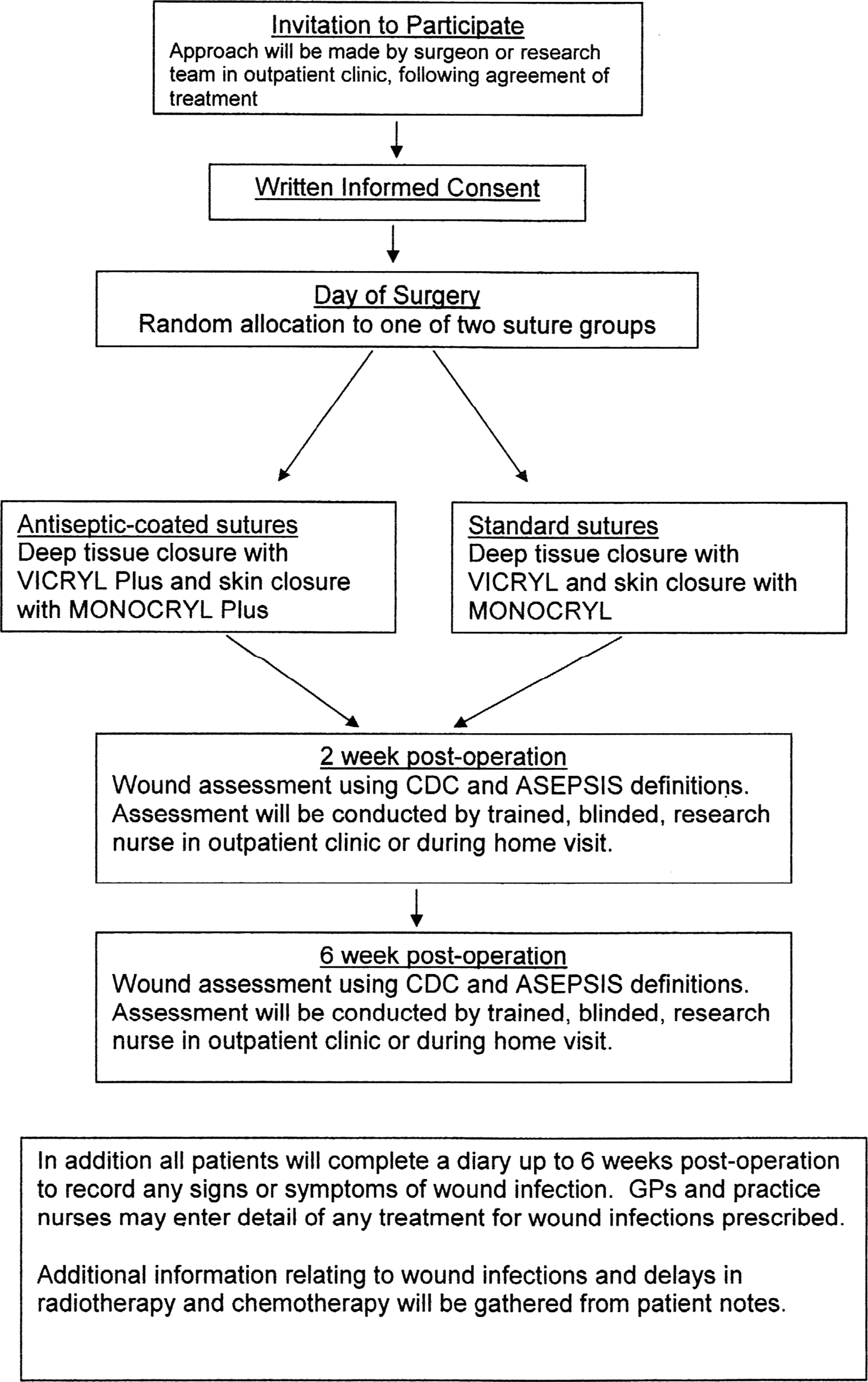
Summary of randomized trial of antimicrobial-coated sutures to prevent surgical site infection after breast cancer surgery.
All operations were undertaken with general anesthesia. Wounds were closed after surgery (Table 1) using subcutaneous polyglactin and subcuticular poliglecaprone, at the discretion of the operating consultant surgeon, with blinding to whether the suture was standard (Vicryl [polyglactin 910] and Monocryl [poliglecaprone 25])(Ethicon, Inc., Somerville, NJ) or triclosan-coated (Vicryl Plus and Monocryl Plus). In addition, wounds were dressed with Steri-Strips (3M, St. Paul, MN) and Tegaderm (3M) or Cosmopore (Hartmann USA, Rock Hill, SC) or Primapore (Smith & Nephew, Hull, UK), or Cosmopore alone, again at the discretion of the surgeon. Eight patients (three control subjects; five having antimicrobial sutures) received a single intravenous dose of 1 g of Augmentin (amoxicillin clavulanate; GlaxoSmithKline, Brentford, Middlesex, UK) antibiotic prophylaxis for surgery considered at risk (high body mass index, mastectomy, or axillary clearance). None subsequently developed an SSI. All other interventions, such as pre-medication, anesthesia, and phlebothrombosis prophylaxis, were standard for both groups.
ANC=axillary node clearance; SNB=sentinel node biopsy; WLE=wide lump excision.
Postoperatively, patients were reviewed regularly by the breast care nurses of the Cardiff and Vale NHS Trust and at two and six weeks postoperatively as outpatients or a home visit by two of the authors (NW and NI) with occasional help from nurses based in the Department of Wound Healing and Dermatology. All investigators were conversant with the CDC definition of SSI and the ASEPSIS and Southampton wound scores and were blinded to the type of suture that had been used. All outcomes were discussed and agreed on by NW, NI, and DL. In addition, all patients were given a diary [35,36] to record their opinions and post-operative incision site progress over the six weeks of post-operative study; substantial events were corroborated by an attending clinician. Diary entries were used to substantiate recorded SSIs using CDC, ASEPSIS, and Southampton data. At the end of the study, patients' notes were trawled for any additional information. Patients who had asked about the outcome of the trial were contacted and thanked again for their participation.
Randomization was undertaken in blocks of 50 using random computer numbers. Randomization was performed in the operating theaters using sequential sealed envelopes. Sutures used during the operations corresponded to the randomization code, but the surgeon, patient, and the assessor at followup were blinded to which type had been used. The power of the study was based on statistical modelling, involving the statistician of the Ethics Committee, using the interval data given by ASEPSIS scores and the anticipated SSI rates found in similar, published studies (reviewed in the Introduction and Discussion of this paper). The estimated sample size of 150 patients, 75 in each group, was considered to have 80% power to show a statistically significant difference of <0.05. Descriptive statistics were expressed as medians and ranges, and inferential statistics used χ2 analysis for categorical data and the Mann-Whitney U test for interval data.
Results
The target number of patients was recruited over the 26 months of the study. Approximately 50 more patients were approached to join the trial but declined. The demographics of the recruited patients (age, weight, type of operation) are shown in Table 1. None of the parameters were significantly different. Four patients were excluded from the two-week assessment of SSI and a further 19 from the six-week assessment. The reasons for this are given in Table 2; again, there are no differences between the groups.
The overall SSI rate using the CDC criteria was 13.7% (20/146) at two weeks and 18.9% (24/127) at six weeks. Most SSIs were manageable on an outpatient basis with conservative treatment; six patients (of the total 24 with recorded SSIs) needed an intervention to open/pack or aspirate axillary collections, three requiring re-admission; a seventh patient had a delay in starting adjuvant chemotherapy. For the two suture groups at two weeks, the SSI rate, based on CDC definitions, was 15.1% (11/73) in the standard suture controls and 12.3% (9/73) in the coated suture group; and at six weeks, the respective SSI rates were 22.9% (14/61) and 15.2% (10/66). None of these differences is statistically significant (Table 3). Although there was a uniform tendency for lower SSI rates in the coated suture group using ASEPSIS and Southampton scores, this did not reach statistical significance (Table 3).
Discussion
This study has shown a high overall SSI rate after breast surgery (13.7% at two weeks and 18.9% at six weeks) in keeping with other studies [37–42]. By definition, all the SSIs were superficial, and relatively few 6/127 (4.7%) necessitated admission or intervention. Had the CDC definitions been used to power the study, the differences in SSI rates between the two groups (control standard vs. antimicrobial-coated sutures) would have required approximately 400 patients to show a statistically significant difference at six weeks and more than 2,000 to show a significant difference at two weeks. The reason the interval data provided by ASEPSIS scores and the pre-study power analysis did not show a statistically significant difference is open to speculation. The ASEPSIS scores were relatively low and inflated mostly by the use of antibiotics, mostly in primary care, although such use perhaps was justified for early and minor signs of inflammation. The Southampton score measures wound healing/surgical outcome rather than infection specifically. Both were modified to allow scores to be computed for patients who were not inpatients. There was a consistent trend using the three methods of assessment in favor of the antimicrobial sutures.
Most studies use the 30-day surveillance CDC definition of SSI in soft tissues, which allow realistic comparisons between studies. It is inappropriate to devise even more definitions, which many other studies have done, although the interval data offered by ASEPSIS do allow some differentiation of the severity of SSIs. In this study, no ASEPSIS score reached 20, which is the cut-off for the finding of SSI. Consequently, there is little correlation between the CDC definition and the ASEPSIS score; the Southampton score did not identify patients with SSI with the same accuracy. The close post-discharge surveillance used in this study, with trained, blinded, experienced assessors and a diary, was highly resource dependent. Although desirable, it is unlikely that such a level of surveillance could be mounted in all Hospital Trusts, and it may over-diagnose SSI.
A high incidence of SSI after breast surgery has been reported in several studies [36–40] although such surveillance programs can reduce the infection rate [41]. Swabs taken from SSIs after breast surgery identify staphylococci as the main organism responsible, although others may be identified that express antibiotic resistance, but cultures often are negative, which suggests that mechanisms other than infection alone may be responsible for poor healing [42]. This might include delayed healing related either to poor blood supply or to acute biofilm formation and explains in part why antibiotic prophylaxis may be unjustified in breast surgery. The number of clinically important SSIs in this study was relatively low and may reflect the attention to detail given by the two surgeons.
Antimicrobial sutures may become part of an SSI prevention bundle [18], but further evaluation will need a larger cohort to show a statistically significant difference for skin closure after breast cancer surgery.
Footnotes
Acknowledgments
This study was supported by an investigator-initiated grant from Ethicon. The authors thank Professor Keith Harding and Sue Hagelstein of the Department of Wound Healing and Dermatology and the breast care nurses of the Cardiff and Vale NHS Trust for their support during this study. Also, we are grateful to Dr Robert Newcombe, Professor of Medical Statistics, Centre for Health Sciences Research, Cardiff University, for his help with statistical modeling.
Author Disclosure Statement
Professor Leaper has been a consultant for the Ethicon division of Johnson & Johnson. The remaining authors have no conflicting interests.
*
Clinical trials.gov identifier NCT008320271; REC reference 08/WSE03/35.