
Abstract
Abstract
Background:
Surgical site infection remains a concern in orthopedic surgery, and contamination of C-arm covers is a potentially modifiable risk factor.
Methods:
A single-cohort study was conducted using 30 consecutive patients undergoing operative fracture fixation. Cultures were obtained from the C-arm cover after initial draping and every 20 min thereafter. The total number of persons in the operating room (person-hours/h of study time) and the number of door openings were recorded. The C-arm position changes and the time to contamination were monitored.
Results:
The median time from the start of the operation to contamination was 20 min. There was a 17% contamination rate on initial draping, 50% at 20 min, 57% at 40 min, and 80% by 80 min. The C-arms in five cases were not contaminated during the surgery. Time to contamination correlated significantly with lateral position changes (correlation [r]=0.64; p=0.003) but was not related to C-arm position changes (r=0.22; p=0.34), number of door openings (r=0.20; p=0.39), or person-hours/h (r=0.04; p=0.85).
Conclusions:
Contamination of the C-arm drape occurs often and early during surgery for orthopedic fractures. We recommend minimal contact with the C-arm to avoid contamination of the surgical field.
Many factors contribute to colonization of the operative site and subsequent infection, not all of which are modifiable. Medical co-morbidities, morbid obesity, advanced age, poor nutritional status, an immunocompromised state, rheumatoid arthritis, and admission to the hospital from another health-care facility are related to a higher incidence of post-operative surgical site complications [3–7]. Unfortunately, such factors often are difficult, if not impossible, to control.
Additionally, there are numerous modifiable peri-operative and intra-operative risk factors. Peri-operative factors such as glycemic control and appropriate administration of antibiotics can influence SSI [3–6,8]. Intra-operative variables also have been examined (e.g., duration of procedure, glove perforation, irrigation fluids, surgical basins, and contamination of scalpels, surgical gowns, and implant trays) with the goal of decreasing contamination and surgical site bacterial load [9–21]. Despite use of the most current techniques to minimize contamination during surgery (e.g., laminar flow operative rooms, ultraviolet lighting, sophisticated implant sterilization, peri-operative antibiotics, and modern surgical preparation and draping procedures), SSI rates for open reduction of fractures continue to range from 0.8% to 5%, depending on patient risk factors [1,22]. Such rates suggest that investigations to identify modifiable risk factors be continued with the objective of improving patient outcomes.
Operative fracture care frequently involves the use of intra-operative imaging, with fluoroscopy being most common. Biswas et al. were the first to publish a report on the sterility of intra-operative fluoroscopy [23]. They demonstrated a high rate of contamination at the end of 25 operative spine cases, with the upper portions of the C-arm intensifier more likely to be contaminated. A time-dependent analysis of the “sterile” C-arm cover as a potential source of intra-operative contamination has not been performed. Thus, the aim of this study was to determine the time to contamination of sterile C-arm covers during surgical fracture care.
Patients and Methods
Institutional Review Board approval was obtained prior to initiation of the study, and all patients signed an informed consent form prior to participation. The study sample consisted of 30 consecutive cases (32 fractures) performed by two of the authors (RTL and MJP) from March to April 2009. Exclusion criteria were an open fracture, a known infection, non-use of a C-arm, and lack of informed consent. In fact, no patient refused to participate in the study. The fracture locations were the distal radius (3), humeral shaft (3), proximal humerus (2), intertrochanteric hip (4), supracondylar femur (1), patella (2), tibial plateau (6), tibial shaft (3), pilon (3), ankle (2), and calcaneus (1). Two other fracture-related procedures were a triple arthrodesis (1) and a subtalar arthrodesis (1).
General Electric OEC 9800 Plus mobile fluoroscopic imaging systems were used (General Electric Company, Fairfield, CT). Cultures were obtained from the top and side-handle areas of the image intensifier cover after initial draping with a sterile C-arm cover and every 20 min thereafter until completion of the operation. The two culture locations were chosen because they had the highest probability of being contacted by the surgeon and are reported to have a greater incidence of contamination [23]. The surgeon and other operating room personnel were not allowed to touch the C-arm during the case.
Cultures were obtained in a standardized fashion. First, the cap of the culture tube (BBL cooked-meat medium; Becton, Dickinson and Company, Sparks, MD) was removed and placed with its sterile side up on a table. Next, a sterile cotton-tip applicator was dipped into the medium and then swabbed against the C-arm cover at the designated locations with gentle pressure for a distance of approximately 10 cm in a single motion. The tip was inserted into the culture tube and leveraged against the side of the tube to break off the tip for a “no-touch” sterile technique. The cap was secured in place immediately using sterile technique. If any break in sterility was suspected, the specimen was discarded and the process repeated. Gloves were worn at all times. Cultures were transported to a local laboratory (CompuNet, Dayton, OH) and evaluated for aerobic and anaerobic bacteria.
Operating room traffic was monitored by observing the cumulative amount of time personnel spent in the room during the procedure (person-hours/h of study time) as well as the number of door openings throughout the case. Person-hours/h included all individuals in the operating room at initial C-arm draping and those who entered subsequently until the conclusion of the case or after the last culture was obtained. Time was rounded to the nearest minute. One door opening consisted of any individual passing into or out of the operative suite.
Movement of the C-arm was recorded by transitions into and out of the operative field as well as rotation into the lateral position. Physician preference determined position change. The amount of time in or out of the operative field and the duration of fluoroscopic exposure were not monitored.
Equal interval survival analysis was performed to evaluate the time to first contamination. Pearson correlation was used to relate the time of contamination to person-hours/h, door openings, transitions into/out of the operative field, and rotations to the lateral position. A power analysis was performed to determine the recommended sample size. At alpha=0.05 and a planned effect size of 0.5 of a standard deviation, 30 subjects were needed to obtain a power of 81%. Inferences of significance were made at the 0.05 level.
Results
For the 30 cases, the mean study time was 1.70±0.65 h, the mean person-hours/h 9.62±1.49, the mean door openings 68±22, the mean C-arm transitions into and out of the operative field 3.10±1.56, and the mean rotations to the lateral position 1.63±1.54.
The median time from the start of the operation to contamination of the C-arm cover was 20 min (95% confidence interval [CI] 2, 38 min). There was a 17% contamination rate on draping, 50% at 20 min, 57% at 40 min, and 80% at 80 min (Fig. 1). In five cases (16.7%), the C-arm did not become contaminated during surgery.
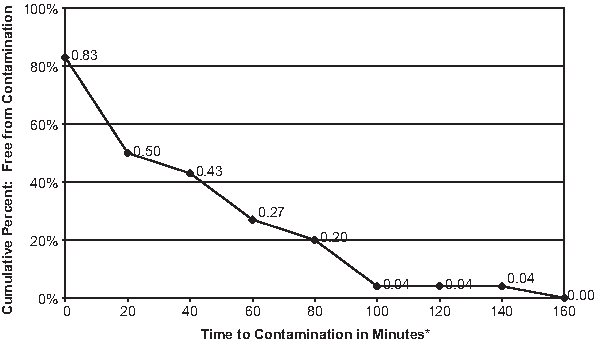
Time to C-arm drape contamination in 30 fracture repairs. (*Rates after 80 minutes based on 25 procedures because five procedures ended at 80 minutes [censored].)
Because five cases were contaminated at the start of the operation and five other cases were not contaminated by the end of the procedure, 20 cases were suitable for the correlation analysis. Time to contamination correlated significantly with lateral position changes (correlation [r]=0.64; p=0.003) but was not related to C-arm position changes (r=−0.22; p=0.34), number of door openings (r=0.20; p=0.39), or person-hours/h (r=0.04; p=0.85). The bacteria detected were Staphylococcus (62%), Corynebacterium spp. (31%), Micrococcus (5%), spp. and other isolates (3%). There were no post-operative surgical site infections.
Discussion
Previous studies have investigated the prevention of surgical infection from specific sources of potential contamination [9–21]. A notable amount of contamination occurs on the C-arm drape by the end of a spine case [23]. We found that C-arm drape contamination occurred rapidly (median time 20 min) and extensively (80% contamination by 80 min).
In this study, bacterial shedding is only one possible source for contamination of the C-arm. Many sources have been cited as potential causes of bacterial contamination of the surgical field: Sneezing surgeons [24], sweating surgeons [25], compressed-air tool exhaust [26], residual contamination of the sterilely prepared limb [27], and individually wrapped orthopaedic implants [28,29]. We believe that contamination of the C-arm drape is frequently airborne, meaning that the arm does not become contaminated through direct contact with a non-sterile object. Subsequent contact with the C-arm cover can then lead to cross-contamination of the surgical field. Further study is required to determine definitively the source and significance of these contaminants.
Intra-operative fluoroscopy is a key component of modern fracture fixation. The C-arm alignment and subsequent adjustments often are guided manually by the surgeon to expedite the desired image projections instead of allowing the radiology technician alone to maneuver the image intensifier into position. Large C-arms have a substantial surface area for exposure to airborne particulate and microbial matter and should be considered part of the surgical field, as a case typically requires numerous transitions into and out of the operative field and position changes. Biswas et al. reported that potentially harmful contamination develops when the C-arm is close to the surgical incision for spine cases [23], and our study results are consistent with their findings for orthopedic fracture repair.
Our study has several limitations. First, contamination during the handling and preparation of specimens cannot be excluded. However, we standardized the procedure for obtaining the culture samples and provided formal instruction to the staff. Only two individuals were involved in specimen collection.
Second, if the hypothesis is the more C-arm movement there is, the earlier the contamination, we would expect a negative correlation between time to contamination and number of transitions into and out of the operative field and number of lateral position changes. Whereas the correlation was negative for the former (r=−0.22; p=0.34), it was positive for the latter (r=0.64; p=0.003). This moderately strong correlation of 0.64 suggests that the greater the number of movements into and out of the operative field, the longer the time to contamination, an unexpected finding. We speculate that our reduced sample size for correlation analysis (only 20 of the 30 cases were eligible) might be a partial explanation. Additional studies are needed to determine whether reducing C-arm movement has a protective effect against contamination.
Third, the bacteria isolated were not all common pathogens for surgical site infection. Yet more than 60% of the isolates were Staphylococcus, which remains a common cause of orthopedic infections. The organisms identified in this study were not speciated, nor was sensitivity analysis performed. Finally, we cannot relate the presence of C-arm drape contamination to post-operative infections, as no post-operative infections were observed in the study sample despite early and frequent contamination of the C-arm drapes.
The operating suite is not as sterile as many assume. Several investigators have concluded that staff members play an important role in the contamination of the operating suite through variable rates of natural bacterial shedding [30–32]. Ritter et al. reported that human beings shed an average of 1,000 to 10,000 bacteria/min and that 30% of operating personnel carry Staphylococcus [32]. Additionally, 1% of premenopausal women, 5% of postmenopausal women, and 13% of men shed at rates exceeding 10,000 bacteria/min [33]. Clothing or coverage of the body does not seem to reduce or affect this process. However, we found no association between time to contamination and intensity of operating room personnel (i.e., person-hours/h) or door openings. In contrast, Ritter reported an increase in the number of colony-forming units when five persons were present in the operating suite [34,35].
We and others recommend the following measures for reducing the bacterial load in the operative setting: (1) Initial cleansing with alcohol followed by use of a bactericidal solution; (2) limiting the number of persons in the operating room; (3) using laminar air flow or ultraviolet lighting to reduce contaminants; (4) using prophylactic antibiotics when an implant is placed; and (5) realizing that the host remains one of the most important factors [31].
In summary, contamination of the C-arm drape occurs often and early during surgery for orthopedic fractures. We recommend that the surgeon refrain from touching the C-arm cover to manipulate the machine. If there is hand contact with the C-arm cover by the surgeon, a change of gloves is suggested to minimize the risk of colonization of the wound. If an extremity contacts the C-arm cover, as often occurs with a mini C-arm, protection with a fresh sterile towel or sheet is recommended.
Author Disclosure Statement
No conflicting financial interests exist.