
Abstract
Abstract
Background:
The objective was to conduct a meta-analysis of randomized controlled trials evaluating the efficacy and morbidity of the management of acute uncomplicated (no abscess or phlegmon) appendicitis by antibiotics versus appendectomy.
Methods:
Appropriate trials were identified. The seven outcome variables were overall complication rate, treatment failure rate for index hospital admission, overall treatment failure rate, length of stay (LOS), utilization of pain medication, duration of pain, and sick leave. Both fixed and random effects meta-analyses were performed using odds ratios (ORs) and weighted or standardized mean differences (WMDs or SMDs, respectively).
Results:
Five trials totaling 980 patients (antibiotics=510, appendectomy=470) were analyzed. In three of the seven outcome analyses, the summary point estimates favored antibiotics over appendectomy, with a 46% reduction in the relative odds of complications (OR 0.54; 95% confidence interval [CI] 0.37, 0.78; p=0.001); a reduction in sick leave/disability (SMD −0.19; CI −0.33, −0.06; p=0.005), and decreased pain medication utilization (SMD −1.55; CI −1.96, −1.14; p<0.0001). For overall treatment failure, the summary point estimate favored appendectomy, with a 40.2% failure rate for antibiotics versus 8.5% for appendectomy (OR 6.72; CI 0.08, 12.99; p<0.001). Initial treatment failure, LOS, and pain duration were similar in the two groups.
Conclusions:
Non-operative management of uncomplicated appendicitis with antibiotics was associated with significantly fewer complications, better pain control, and shorter sick leave, but overall had inferior efficacy because of the high rate of recurrence in comparison with appendectomy.
Several earlier retrospective studies [15–23] implied that acute uncomplicated appendicitis can be treated successfully with antibiotics alone, and an earlier meta-analysis of three randomized controlled studies [24] showed a trend toward fewer complications in the patients treated non-operatively. Individually, the results from the randomized trials are inconsistent, with one trial [13] showing non-inferiority of antibiotics to appendectomy, whereas the others were either inconclusive or showed equivalence of appendectomy and non-operative management with antibiotics [8–12].
The objective of this review was to compare the study-related efficacy and morbidity of antibiotic therapy alone with appendectomy in the treatment of patients with acute uncomplicated appendicitis. Effectiveness outcomes were therapeutic success during the index hospital admission, pain control, length of hospital stay (LOS), time to return to work, recurrence, and morbidity outcomes, namely, any complication of either non-operative or operative management. The primary topic therefore was whether non-operative management with antimicrobial therapy given to patients with a suspicion of appendicitis could be effective source control without a need for appendectomy.
Patients and Methods
Data sources
A systematic review of the literature was performed to identify all randomized controlled trials (RCTs) in which treatment with any antibiotic regimen was compared with appendectomy in patients with suspected appendicitis. Medline, Embase, the Cochrane Central Register of Controlled Trials, and relevant meeting abstracts published between January 1950 and May 2011 were searched using the following MeSH terms: appendectomy/; appendicectomy/; appendicitis/; non-operative/; conservative/; and antibiotic therapy.
Study selection criteria
Only RCTs comparing management with any antimicrobial regimen with appendectomy for appendicitis were included. Two authors (R.J.M., A.M.) reviewed the citations for relevance and extracted the data. The data captured were the method of diagnosis, antibiotic regimen, operative technique, pathology findings, LOS, pain assessments, complications, and duration of followup. The data extractors were not blinded to the study hypothesis. Disagreement between the reviewers was resolved by a consensus meeting with a third reviewer (H.S.). Patients of any age and either sex with suspected acute uncomplicated appendicitis based on clinical presentation with or without radiologic confirmation were included.
Given the nature of the interventions, blinding of the surgeon, patient, and outcome assessor was not possible and therefore was not an exclusion criterion. There were no restrictions on the type of antibiotic, duration of antibiotic, or the appendectomy technique (open or laparoscopic). Studies enrolling patients with known complicated appendicitis at the time of randomization, including subjects with periappendicular abscess or phlegmon, were excluded.
Data extraction, quality appraisal, and outcomes of interest
The studies were assessed for methodological quality using the Jadad scoring system [25] in which each study was assigned a score between zero (lowest quality) and five (highest quality) based on reporting of randomization and blinding and description of withdrawals.
The seven outcome variables analyzed were: (1) Initial treatment failure rate; (2) overall treatment failure rate; (3) overall complication rate; (4) duration of pain; (5) utilization of pain medication; (6) LOS; and (7) duration of sick leave. The treatment failure rate during the initial hospitalization was determined from the absence of therapeutic efficacy. For antibiotic treatment, success was defined as definite improvement without need for surgery and subsequent hospital discharge without an operation. Efficacy for surgical treatment was pathologically confirmed appendicitis after surgery or another appropriate surgical indication for operation. Thus, patients with a pathologically proved normal appendix were classified as treatment failures. Overall treatment failure was determined during the followup period up to one year. This included any patient in the antibiotic group who required an appendectomy because of recurrence of appendicitis after the initial hospitalization. Complications included any antibiotic-related or surgery-related morbidity. As stated above, the data extractors were not blinded to the study hypothesis, and two of the outcome variables, namely, the initial and overall treatment failure rates, are subject to interpretation bias. The other five outcome variables were objective outcomes and not subject to interpretation bias.
Statistical analysis
All analyses were performed using RevMan 5.1 (The Nordic Cochrane Centre, The Cochrane Collaboration, Copenhagen, Denmark). The meta-analysis was performed according to the recommendations of The Cochrane Collaboration and the Cochrane Handbook for Systematic Reviews of Interventions [26].
Initial and overall treatment failures are reported using odds ratios (ORs) with 95% confidence intervals (CIs). Study heterogeneity was determined using the I2 statistic and the p value from the χ2 test. Interpretation of the I2 statistic was based on the guidelines in the Cochrane Handbook in which 0% to 40% may be unimportant heterogeneity and 30%–60% indicates moderate, 50%–90% indicates substantial, and 75%–100% indicates considerable heterogeneity [26]. Pooled analyses were performed with the Mantel–Haenszel method using a random effects model because these outcomes are influenced by the context of care. Length of hospital stay was assessed using weighted mean differences (WMDs) with the 95% CI and a random effects model. Because the trials used different types and dosages of pain medication and determined duration of pain and sick leave/disability differently, we assessed these outcomes using standardized mean differences (SMDs) with 95% CIs and a random effects model. Complication rates are reported using ORs with the 95% CIs. Morbidity after appendectomy and the side effects associated with the antibiotics was uncommon. Pooled estimates of effect therefore were calculated using Peto's odds ratios, because simulation studies have shown that this measure is most robust when events are rare and the numbers of patients in the control and the experimental groups are similar [27]. Funnel plots were assessed to provide a visual assessment of whether treatment estimates were associated with study size and to detect publication and other biases. Significance was set at a p value of 0.05.
Sensitivity analysis
In the trial published by Hansson et al., only 52.5% of the patients assigned to the antibiotic arm (106/202) and 92.2% of patients assigned to the appendectomy arm (154/167) actually received the assigned treatment. In the main analysis, the crossover patients were analyzed in their assigned group using an intention-to-treat method. In the sensitivity analysis, we analyzed the data first excluding the trial by Hansson et al. [10] and then by calculating the statistic using a per-protocol analysis with the patients analyzed according to the treatment they actually received. This step was performed in an attempt to replicate the “real world” result.
Results
The Medline and Embase literature search identified 306 potentially relevant papers. We excluded 298 studies, 214 because they were non-randomized, and 84 because they studied other treatments. We then retrieved and reviewed eight full reports and excluded three more studies: Two because they enrolled patients with known complicated appendicitis and one [12] because there were no usable secondary outcome data and because it did not truly randomize patients between antibiotic treatment and appendectomy. Five studies including 980 patients were included in our meta-analyses [8–11,13].
Description of the trials
A description and summary of each trial's methodology is shown in Table 1. All studies had only two arms, antibiotic or appendectomy, and the treatment strategy in all five was similar. Because of the nature of the treatment arms, none of the studies was blinded. Three of the groups of authors performed a sample size calculation to support enrollment numbers. Two of the studies had a sample size of <50 per group [8,11]. The age range of the patients was 17 to 94 years; all studies excluded children. Four of the studies [8,10,11,13] included both male and female patients, and one study included only men [9]. Together, the five studies enrolled 671 male and 309 female patients. Selection of the patients in four of the studies was mainly on clinical grounds. In one study, computed tomography (CT) scans were obtained on every patient [13], two of the groups of investigators [8,11] used ultrasound scanning routinely, and one study [10] used ultrasonography and CT selectively to confirm the clinical suspicion of acute uncomplicated appendicitis. Four studies also utilized serum C-reactive protein (CRP) to aid in screening.
In the patients undergoing operation.
Recurrence using per-protocol analysis.
CRP=C-reactive protein; CT=computed tomography; US=ultrasonography.
There were differences in the choice of antibiotic, antibiotic dosage, and duration of antibiotic therapy. The antibiotics used were divided into nine major groups; the details are summarized in Table 2.
In three studies, the technique of appendectomy, whether open or laparoscopic, was defined poorly (Table 2). In the study of Stryud et al. [9], 6% (8/128) and in the trial by Vons et al. [13], 66% (78/119) of the patients underwent laparoscopic appendectomy.
Formal followup ranged from 7 mos–1 yr. Recurrence of appendicitis later than 30 days after successful non-operative management was reported in all five studies [8–11,13], and the rate ranged from 6.9%–35% (Table 1), for a mean overall recurrence rate of 13%. The mean time to recurrence ranged from 4–8 mos. Complications were reported in all five studies (Table 3).
Organ space infection occurs within 30 days after the operation or appendicitis and appears to be related to the operation or appendicitis. It involves any part of the anatomy (e.g., organ or space) other than the appendix or the incision created or manipulated during an operation.
Other complications were enteritis, thrombophlebitis, rectus muscle hematoma, sensoric loss in leg, urticaria, scrotal edema, diarrhea, reoperation, wound dehiscence, incisional hernia, ileocecal resection, caval vein thrombosis, ileus, bladder dysfunction, aspiration at extubation, pulmonary embolism, postoperative cardiac problems, vaginal or anal fungal infections, clostridium infection, and tooth injury.
Specific details not provided but reported mostly as surgical site infections.
NR=not reported.
Quality appraisal
The quality of the five studies ranged from poor to fair (mean Jadad score 1.8 of 5), with each study having some methodologic flaws (Table 4). All studies reported random allocation, although only three had an appropriate method of randomization. None of the studies reported blinding of the outcome assessors, as blinding is impossible. Only one paper described withdrawals and dropouts from the study.
Methodological quality
Funnel plots (mean differences, SMDs, or log ORs) demonstrated asymmetry for initial and overall treatment failure, suggesting the presence of publication bias and study heterogeneity for these outcomes (Fig. 1). No points fell outside the 95% CIs for complications, LOS, utilization of pain medication, duration of sick leave, or pain, suggesting the absence of publication bias and heterogeneity for these outcomes.
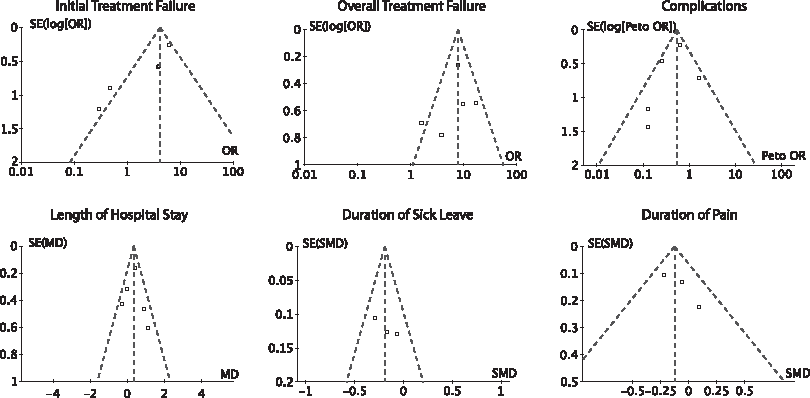
Funnel plots demonstrate asymmetry of initial treatment failure, overall treatment failure, and length of hospital stay, suggesting presence of publication bias and heterogeneity. No points fall outside 95% confidence limits for any other variable, suggesting absence of publication bias and heterogeneity.
Outcomes
Data for initial treatment failure and LOS were analyzed in all five trials. All trials reported data on complications and overall treatment failure, three trials had data for duration of pain and sick leave/disability, and only two trials had usable data on pain medication (Table 5). In three of the outcomes, the summary point estimates favored antibiotic therapy over appendectomy. These studies reported: (1) A 46% reduction in the relative odds of any complication in patients treated non-operatively (antibiotic group 11.8%, appendectomy 18%; OR 0.54; 95% CI 0.37–0.78; p=0.001; Fig. 2); (2) a reduction in the duration of sick leave or disability (SMD −1.19; 95% CI −0.33, −0.06; p=0.005; Fig. 3) in the patients treated non-operatively; and (3) decreased utilization of pain medication in the antibiotic-treated group (SMD −1.55; 95% CI −1.96, −1.14; p<0.0001; Fig. 4).
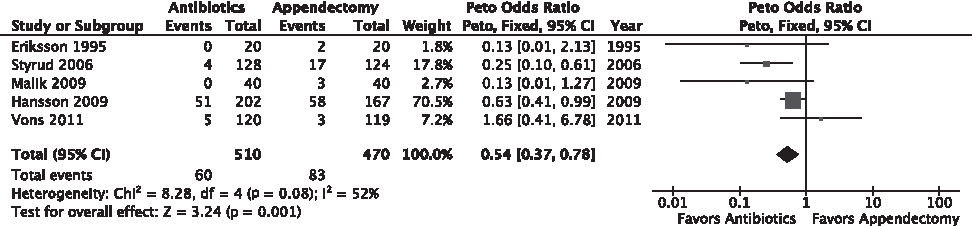
Forest plot of antibiotics versus appendectomy for overall complications, depicted as Peto odds ratios. Diamond represents overall treatment effects, and squares are treatment effects for individual studies, with 95% confidence intervals indicated by horizontal lines. CI=confidence interval.

Forest plots of antibiotics vs. appendectomy for duration of sick leave or disability, depicted as standardized mean differences using random effects model. Diamond represents overall treatment effects, and squares are treatment effects for individual studies, with 95% confidence intervals indicated by horizontal lines. These data were not reported in three studies. CI=confidence interval; SD=standard deviation.

Forest plots of antibiotics versus appendectomy for utilization of pain medication, depicted as standardized mean differences using random effects model. Diamond represents overall treatment effects, and squares are treatment effects for individual studies, with 95% confidence intervals indicated by horizontal lines. These data were reported in only two studies. CI=confidence interval; SD=standard deviation.
Mean length of stay reported incorrectly in the original manuscript. Error corrected after personal communication with authors; however, no standard deviation (SD) supplied, so we imputed the SD as the mean value.
The only outcome that favored the appendectomy group was overall treatment failure, which showed a 30% reduction in relative risk with appendectomy. The overall treatment failure rate in the antibiotic group was 40.2% versus 8.5% in the appendectomy group (OR 6.72; 95% CI 3.48–12.99; p<0.00001; Fig. 5).
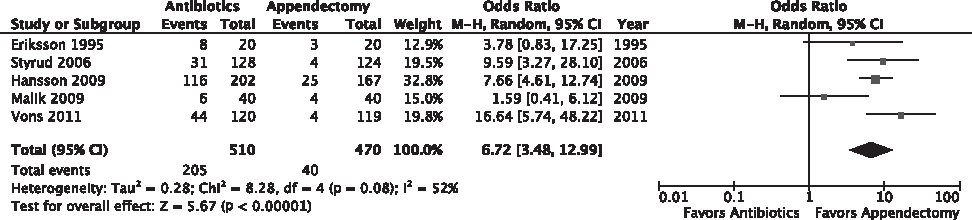
Forest plots of antibiotics versus appendectomy for overall treatment failure, depicted as odds ratios using the Mantel–Haenszel random effects model. Diamond represents overall treatment effects, and squares are treatment effects for individual studies, with 95% confidence intervals indicated by horizontal lines. CI=confidence interval.
For the remaining three outcomes, there were no significant differences between antibiotics and appendectomy. For the initial hospitalization, the therapeutic failure rate for antibiotics was 26.8% and that for appendectomy 8.9% (OR 2.43; 95% CI 0.94–6.33; p=0.07; Fig. 6). There was no significant difference in the LOS (WMD 0.34; 95% CI −0.06–0.73; p=0.09; Fig. 7) or duration of pain (WMD −0.13; 95% CI −0.28, 0.03; p=0.11; Fig. 8). Pooled summary statistics for the seven outcomes are shown in Table 6.
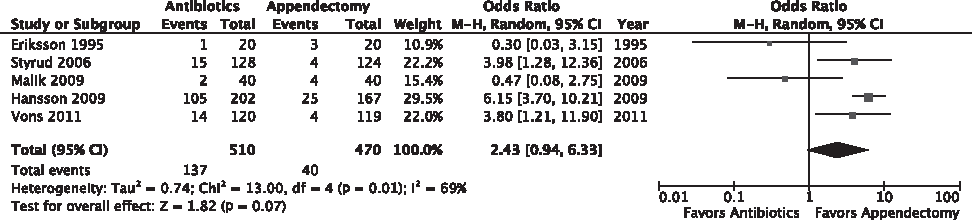
Forest plots of antibiotics versus appendectomy for treatment failure for index hospital admission, depicted as odds ratios using Mantel–Haenszel random effects model. Diamond represents overall treatment effects, and squares are treatment effects for individual studies, with 95% confidence intervals indicated by horizontal lines. CI=confidence interval.
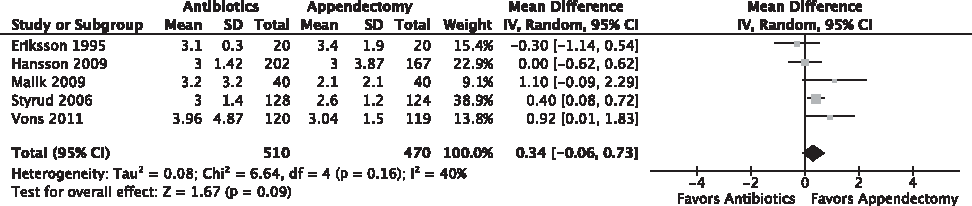
Forest plots of antibiotics versus appendectomy for length of hospital stay, depicted as standardized mean difference using random effects model. Diamond represents overall treatment effects, and squares are treatment effects for individual studies, with 95% confidence intervals indicated by horizontal lines. CI=confidence interval; SD=standard deviation.

Forest plots of antibiotics versus appendectomy for duration of pain, depicted as standardized mean difference using random effects model. Diamond represents overall treatment effects, and squares are treatment effects for individual studies, with 95% confidence intervals indicated by horizontal lines. Duration of pain was not reported in three studies. CI=confidence interval; SD=standard deviation.
CI=confidence interval.
Significant heterogeneity, as evidenced by the values of the Q statistic and I2 index, was present for the initial treatment failure rate (Q=13.00; p=0.01; I2 69%). No heterogeneity was detected for any other outcome measure (Table 6).
Sensitivity analysis
The sensitivity analysis, in which we considered the real-world scenario and analyzed the data of Hansson et al. as treatment received using a per-protocol analysis, the findings for all seven outcome measures were exactly the same as for the main analysis in which we used an intention-to-treat analysis (Table 7). Summary estimates still favored antibiotics over appendectomy for developing any complication, duration of sick leave, and utilization of pain medication. Overall treatment failure was still better with appendectomy and initial treatment failure, LOS, and pain duration were similar in the antibiotic and appendectomy groups. In the second scenario, when we excluded the data of Hansson et al. from the analysis, the summary estimates were the same as those found in the main analysis for all the outcome measures except duration of sick leave, which no longer favored the antibiotic group but rather showed equivalence to the appendectomy group (Table 7).
Pain medication usage not shown, as this was not reported in the paper by Hansson et al.
CI=confidence interval.
Discussion
In trials with both a surgical and a non-surgical arm, comparisons between treatment groups inevitably are associated with a bias for both investigators and patients. As pointed out by Jadad [25], when concealment in patient allocation is lacking, open assessment tends to yield a statistically significantly larger estimate of treatment effects. Thus, in summarizing the treatment outcomes in trials such as those reviewed here, point estimates are likely to favor appendectomy, as it has been considered the gold standard for the treatment of acute appendicitis. Therefore, rather than focusing on whether appendectomy is superior or similar to antibiotic therapy, we should examine the safety of antibiotics and the reduction in surgically-related morbidity by using antibiotics as the first-line treatment option for patients with uncomplicated appendicitis. This meta-analysis showed that patients who underwent antibiotic therapy were at a significantly lower risk of any complication than those undergoing appendectomy. This finding is in keeping with an earlier meta-analysis [24] that included only three studies and showed a trend toward fewer complications with antibiotics. Thus, one advantage of non-operative management of uncomplicated appendicitis is the absence of any surgery-related morbidity, which appears to be more frequent after appendectomy than antibiotic therapy. It is interesting that in the pooled analysis, 37% (22) of the complications seen in the 60 antibiotic-treated patients actually were surgery-related. However, because all studies correctly used an intention-to-treat analysis, these complications were assigned to the original randomization group. In addition to the absence of any surgery-related complications, there is an absence of incisional pain in the patients treated non-operatively. In the two studies that reported analgesic consumption, both showed significantly less pain medication usage in the patients treated with antibiotics than in those undergoing appendectomy. Furthermore, the meta-analysis showed a trend toward a shorter duration of pain in the antibiotic-treated group.
As expected, reduced pain and decreased complications were associated with a significantly shorter duration of sick leave/disability in the patients treated non-operatively. Although no difference was found in the LOS, this may have been attributable to the protocol-driven nature of the trials that dictated a mandatory period of hospitalization in the antibiotic-treated group of patients and the initial uncertainty associated with an unproved therapeutic modality.
There were no deaths in any of the studies. There has always been a concern that expectant management of patients with appendicitis would lead to serious complications or fatalities. The fact that no deaths were reported could be related to the close monitoring and mandatory period of hospitalization to which the patients in these trials were subjected. By contrast, standardized mortality ratios have shown a seven-fold excess rate of deaths after appendectomy compared with the general population [28], and the excess rates for patients with non-perforated and non-surgical abdominal pain suggest that some of the deaths may be caused by surgical trauma. The unanswered question is whether the standardized mortality ratios with non-operative treatment of uncomplicated appendicitis using antibiotics only also is associated with an excess rate of deaths. Future large multi-center trials are needed to answer this question.
No difference in treatment efficacy was demonstrated between antibiotic therapy and appendectomy for the index hospital admission for acute uncomplicated appendicitis. There was a trend toward a lower risk of failure in the appendectomy-treated group. However, we believe that there are a number of caveats in interpreting this outcome. First, optimal surgical therapy was not compared with optimal antibiotic therapy in any of the studies. Amoxicillin-clavulanic acid was the antibiotic in two studies, and this combination has been associated with considerable Escherichia coli non-susceptibility, with the rate of resistance to this antibiotic in Europe being as high as 66% [29,30]. Second, the technique of appendectomy, whether laparoscopic or open, influences morbidity [31,32], and in none of the studies was the operative technique standardized or reported accurately. The laparoscopic appendectomy technique has been associated with fewer post-operative complications [31,32], and in all but one of the studies in this meta-analysis, laparoscopy appeared to be the least-favored surgical technique. Third, the studies all included a high proportion of patients with either a perforated or a gangrenous appendix, the rate ranging from 5% for perforation to 48% for gangrenous appendicitis [9,10]. Even in the study reported by Vons et al. [13], in which a CT scan was used routinely for diagnosis, the perforation rate was extremely high at 21%. In none of the studies was the presence of an appendicolith a contraindication to non-operative management, yet there is increasing evidence [13,22] that patients with an appendicolith have a high incidence of failure with non-operative management, and these patients therefore should be excluded from this treatment. The fact that only one trial routinely used a CT scan to aid diagnosis is problematic, and not the U.S. standard of care [7]. Computed tomography scanning is essential in all patients to exclude non-appendicitis and to identify perforated appendicitis or an appendiceal abscess. Future trials need to exclude all patients with perforated appendicitis and compare the best antibiotic therapy with the best surgical technique. Furthermore, routine imaging should be used during followup to ensure that there is no bias.
The overall therapeutic failure rate was significantly better for the patients treated with appendectomy. However, in nearly all the studies, the design protocol dictated that a recurrence of appendicitis mandated appendectomy. An alternative would be to give another course of antibiotics, such as is used for recurrent attacks of diverticulitis [33], or a different antibiotic, as recurrence may be an indication of antibiotic resistance. However, the recurrence rates described in the present meta-analysis may not be representative of the true recurrence rates after antibiotic therapy because of the relatively short followup for most of the patients, the lack of diagnostic definitions for recurrence, and the absence of uniform selection criteria for patients with minimal appendicitis. No trial looked at recurrence rates beyond 12 months, and there currently are no data available on the long-term risk of appendicitis after non-operative treatment.
There was bias in all the studies in that those patients in the appendectomy group who were found at operation to have perforation were treated with antibiotics post-operatively. Strictly speaking, these patients should be classified as treatment failures of appendectomy, that is, failure of surgery to provide adequate source control. In contrast, patients in the antibiotic group who needed to have surgery to provide adequate source control were all considered treatment failures. None of the trials addressed this bias, and the outcomes might have been different if patients in the surgery arms of these studies had not been given this preferential treatment.
There were design flaws in each of the studies reviewed, and two in particular are worthy of mention. In the study by Vons et al. [13], “complicated appendicitis with peritonitis identified at surgery” was the primary endpoint in evaluating patients in the antibiotic treatment group but not the appendectomy group. As pointed out by the authors in their paper [13], this condition likely had been present at the time of randomization. So, in this study, the lower observed rate of complicated appendicitis in the antibiotic group probably represented antibiotic treatment success rather than antibiotic treatment failure. Therefore, there clearly is a significant bias introduced by using “complicated appendicitis with peritonitis identified at surgery” as the primary binary endpoint for the antibiotic treatment group but not the appendectomy group. A major treatment selection bias was observed in the study by Hansson et al. [10], where nearly one-half of the patients randomized to antibiotics crossed over to the appendectomy group prior to receiving any drug. In the main intent-to-treat analysis, these crossover patients were classified as antibiotic treatment failures, a practice some would consider highly misleading. To address this question, we performed a secondary sensitivity analysis. When assessing the patients of Hansson et al. [10] by treatment received using a per-protocol analysis, we found results identical to those when the crossovers were classified as failures for all seven outcome measures.
To a degree, the meta-analysis was adversely affected by the poor methodology of the studies. Three of the trials had small patient numbers, and the sample size even after pooling may have been too small to detect a difference when the events of interest are so infrequent. One also must consider that the nature of the intervention makes it difficult to blind the surgeons, patients, and outcome assessors. In several instances, the outcomes were easily influenced by the prejudices of the care providers (e.g., duration of disability). Further affecting the quality of the evidence is the lack of definitions for many of the outcomes (e.g., site infections), and this increases the risk of bias when definitions have not been established at the outset. The variability of clinical factors, including diagnostic criteria, selection of inclusion, technique of appendectomy, type of antibiotic, and duration of antibiotic therapy and of followup all contributed to the heterogeneity encountered in this review. Incorporation of many patients with perforated and gangrenous appendicitis also limits the generalizability of the results.
The above notwithstanding, the available evidence suggests that antibiotic therapy is at least as effective as appendectomy for the treatment of appendicitis for the initial or index hospitalization period. Antibiotic therapy offers a significantly lower risk of complications than does appendectomy. Furthermore, the use of antibiotics alone is superior to appendectomy for pain control and time off work/school. Finally, antibiotic therapy could be considered as an alternative option in the treatment of patients with acute uncomplicated appendicitis if the patient is willing to accept initial failure and a subsequent recurrence rate of about 40% in exchange for the possibility of forgoing surgery and its associated risks.
Footnotes
Acknowledgments
We would like to acknowledge Jolene Moroney for writing assistance.
Author Disclosure Statement
The authors have no conflict of interests to disclose.