
Abstract

The Law of the Few
Gladwell considers “The Law of the Few” “whereby the success of any kind of social epidemic is heavily dependent on the involvement of people with a particular and rare set of social gifts” [1]. He names the particular players in this change network Connectors, Mavens, and Salesmen.
Let's consider for a moment, by reviewing how we have gotten to this tipping point, who the actors have been in the revolution in residency training. Although I am sure you all know these things, let's review the road we have traveled.
No doubt, Libby Zion, an 18-year old college student who presented to The New York Hospital emergency room on March 4, 1984 with a fever of 103.5°F, agitation, confusion, and odd muscle twitching, is a central player in this revolution. The emergency room physicians could not determine what was wrong with her, and her attending physician, Doctor Raymond Sherman, approved of her admission to the ward with a diagnosis of “viral syndrome” [2]. She was admitted to the medical service, where a Post-Graduate Year (PGY) I resident, Doctor Luise Weinstein, was responsible for her admission orders, and a PGY II resident, Doctor Gregg Stone, provided supervision. Although the exact details of the overnight hours have been subject to debate, Ms. Zion apparently became more agitated, twice discontinuing intravenous catheters. She was placed in five-point restraints and given meperidine and haloperidol. Her temperature continued to increase, ultimately to a peak near 108°F at the time of her death [2].
When examining the actions of the two physicians that night, it was found that Doctor Weinstein was called away to care for her more than 40 patients. Although she was contacted by the nursing staff about Ms Zion's fever and agitation, Doctor Weinstein did not see the patient again during the night. Further, Doctor Stone was not called by the nursing staff that night, and he was reported to have gone to rest after Ms Zion was admitted [2]. I believe he was using “strategic napping,” although of course he did not know it at the time.
Doctor Jon Perl performed an autopsy and provided an amendment to her Certificate of Death. The amendment said “acute pneumonitis four days following dental extraction and in the course of treatment with erythromycin. Hyperpyrexia (high fever) and sudden collapse shortly following injection of meperidine (Demerol) and haloperidol (Haldol) while in restraints for toxic agitation (emphasis added). History of therapeutic phenelzine (Nardil) injection. Unclassified” [4].
So why did Libby Zion die? Although it was widely reported that she had a positive test for cocaine, she had not reported its use in her history, and review of the radioimmunoassay results in retrospect suggest that the concentrations were in a gray zone in which a confirmatory test would be required. However, this test was never performed [4].
On reflection, the cause of Libby Zion's death could have been any of several factors, or a combination of causes. First, cocaine was a possible contributing cause, yet this was never verified with a standard confirmatory examination [4]. Libby Zion may have experienced a drug interaction caused by the combined use of meperidine in the setting of phenelzine use. The meperidine was given just 3 h before her death. Her extreme agitation also could have been caused by an interaction between the phenelzine and the ephedrine she was taking over the counter for congestion. Finally, Libby Zion had had an infected molar tooth extracted four days before her death, and her post-mortem pulmonary cultures grew Streptococcus and other organisms and she had petechiae on her skin. Perhaps she even died of a surgical site infection. We will never know for certain.
So why is Libby Zion important to this discussion? First, she may have died of unrecognized infection. Perhaps more importantly, her father Sidney Zion, a lawyer and journalist, propelled her story and his concerns about both resident supervision and fatigue attributable to sleep deprivation to the public, political avenues, and in fact, to the criminal courts [2]. His passion and persistence on this topic eventually caused district attorney Robert Morgenthau to ask a grand jury for murder charges against the hospital and trainees. The grand jury refused to indict the physicians, but it did indict the medical system. They “strongly criticized the supervision of interns and junior residents at a hospital in New York” [5]. Further, they found that “no attending physician had performed an examination; only an intern and junior medical resident had supervised the patient's admission; those two duty officers had each been working for 18 h at the time of admission (2:00
The civil suit brought by Sidney Zion against the physicians and The New York Hospital eventually was decided February 6, 1995. Doctors Sherman, Stone, and Weinstein were found negligent, and New York Hospital was cleared of wrongdoing. The physicians and hospital were instructed to pay the Zion family $750,000 for pain and suffering, which was reduced to $375,000 (owing to the theory of contributory negligence on the part of Ms. Zion, for withholding crucial medical historical information). Also awarded was $1 for wrongful death, trebled for punitive damages.
Although the civil suit took many years to unfold before a decision was announced, New York State Health Commissioner Doctor David Axelrod asked Doctor Bertrand Bell and a commission to examine the issues of supervision and sleep deprivation, as well as the fundamental structure of residency training in New York. The Bell Commission report resulted in New York State Department of Health Code, Section 405, also known as the Libby Zion law [6]. Effective July 1, 1989, post-graduate trainees would by law be required to work less than an average of 80 h over a four-week period and could not be scheduled to work more than 24 consecutive hours. Each two periods of work are to be separated by not less than eight non-working hours, and each resident should have at least one 20-h period of scheduled non-working time per week. Further, the rule stated that postgraduate trainees must have in-house supervision by a Board-eligible or -certified physician or someone who has completed a minimum of four post-graduate years in house 24 h/day, 7 days/week. In hospitals that documented that an attending physician was readily available by telephone and in person when needed, a resident in his or her final year of training or who had completed at least three years of training could serve as the supervisor [6]. Although surgery training programs initially were not included in the duty hour regulations, supervision guidelines for surgery included having an attending presence in the operating room and in any procedure requiring general anesthesia, pre-operative assessment by an attending physician, and post-operative assessment no less frequently than daily by the attending physician [6]. Thus for all specialties in New York, rules for attending physician supervision became a matter of law.
These regulations were enacted in 1989 in New York. In 2003, the Accreditation Council for Graduate Medical Education (ACGME) declared duty hour rules similar to Libby's Law. Thus, Sidney Zion had served as a Connector, the Bell Commission as Mavens, and the ACGME as Salesmen for duty hour regulation.
The Stickiness Factor
Gladwell next refers to the “Stickiness Factor:” The specific content of the message that renders its impact memorable. Clearly, the death of a young woman because of “fatigued,” “over-worked,” and “unsupervised” residents was a powerful message that rang true with both the public and political factions. Thus, the “epidemic” related to resident duty hours and performance shifted to the Institute of Medicine (IOM), which formed a workgroup assigned to “Optimizing Graduate Medical Trainee (Resident) Hours and Work Schedules to Improve Patient Safety.” They were tasked to synthesize the evidence regarding medical resident schedules and healthcare safety and also with the development of strategies to optimize safety in the healthcare work environment.
The IOM released its report on December 15, 2008 [7]. First, the report affirmed that a total of 80 h averaged over four weeks should continue to be enforced and that the maximum call in-house should not exceed every third night, without averaging. They recommended a 16-h shift, or a 30-h shift with strategic napping for 5 h between 10
Let us turn for a moment to examine the work of a resident while he or she is in the hospital. Schwartz et al. examined the conceptual frameworks of published research papers on this subject and considered by the IOM report and in the period following their report up until 2010 [8]. The authors considered resident activities in six areas: Patient care of high educational value, patient care of low educational value, educational non-patient care, rest on call, protected sleep, and administrative activities. Those authors found that many of the tested conceptual frameworks studying the effects of the duty hour changes were contradictory. For example, frameworks focusing on patient outcomes emphasized either reduction in errors by better-rested residents or increased errors attributable to lack of continuity and increased handoffs. Papers focusing on resident outcomes proposed improvements in the quality of life or health of residents from more sleep vs. concerns about skill reduction caused by reduced educational opportunities [8]. Faculty outcomes uniformly predicted negative outcomes from duty hour changes, and institutional perspectives focused on the costs of implementing the IOM's recommendations [8].
What do we know about the effects of the 2003 ACGME rules on resident and faculty outcomes? Jamal et al. recently published a systematic review on the effects of the changes on resident and faculty outcomes [9]. They identified 15 studies that examined the number of resident cases. Thirteen of these studies were either positive or neutral in their findings about resident case numbers, and only two studies suggested a decrement in resident cases [9]. Five high-quality studies reported a positive or neutral effect on examination scores, and no reports documented a decline in the American Board of Surgery In-Training Examination (ABSITE) or the qualifying examination scores after the 2003 rules were in place [9]. One concern about the duty hours was that residents would have less time to attend clinic and thus lose out on the pre-operative and post-operative learning that occurs exclusively in an outpatient clinic. Two papers addressed this issue, coming to opposite conclusions: One paper noted that clinic attendance was not altered, whereas the other reported that resident attendance at clinic was decreased [9]. Gelfand et al. noted that residents had less time for educational activities [10].
One of the major apparent benefits of the 2003 rules for residents was an improvement in resident quality of life and feeling of psychological well-being [9]. Using validated surveys such as the Symptoms Checklist-90 and the Perceived Stress Scale, residents at four surgical training programs were compared with residents in the same program before the changes and a control population [11]. Residents training under the 2003 rules had fewer psychological symptoms but the same level of stress perception. One additional study demonstrated lower levels of resident burnout and higher motivation after the 2003 rules were implemented [12]. Although a total of 56 studies examined resident well-being, except in the three studies described, the investigators did not use validated measures. Having noted this, it is important to point out that no study reported negative psychological changes or reduced quality of life with the 2003 restrictions [9].
Although the paper by Jamal et al. summarized the findings of high-quality studies of the effects on residents as generally positive or neutral, these authors concluded that surgical faculty experienced negative outcomes [9]. Although the majority of studies were of low quality, three papers considered of high quality reported specific negative outcomes for the surgical faculty: They were less satisfied with surgical training, with the quality of patient care, and with the continuity of patient care. Further, those authors reported a decrease in the quality of life for the surgical faculty. One study showed a quantifiable increase in faculty work hours and less job satisfaction. However, SIS Past President Doctor Mark Malangoni reported neither a change in faculty work hours nor any change in faculty productivity after the work hour changes [13].
Is this the whole story? There is no doubt that program directors, surgical chairs, and other leaders in surgical education had grave concerns about the effects of the 2003 duty hour changes on the quality of surgical training and patient outcomes. Residency programs adapted to these restrictions by reformatting resident schedules, often by combining services and using cross-coverage [9]. Some institutions changed resident workload by adding mid-level practitioners, or by shifting responsibilities from one resident level to another. In some cases, this allowed more-junior residents to assume more responsibilities.
The world now is a different place (http://www.youtube.com/watch?v=ihbL8ewkP-o)[14]. In spite of the concerns about what might happen, the published literature on the 2003 rules does not support a decrement in the quality of our surgical trainees, nor does the literature show any significant changes in patient care outcomes. We do not know exactly how specific programs have adapted to these restrictions, and we do not know the real costs of these changes. It is possible that institutions where resident operating room experiences were maintained have invested funds to support the work performed by residents outside the operating room at the cost of outpatient experience or some other educational work. We do know, however, that our trainees apply more often to fellowship training programs, although the reasons they do this are not entirely clear. Is it because they are less confident, because they believe further training will improve their practice opportunities, or some combination of these factors?
Who Applies to Residency Programs?
Before we consider what effect the newest rules may have on our residents and ultimately on our society, let us step back and look at our applicants. Prior to 1990, there were more applicants to general surgery training programs than there were eligible positions. However, in the 1990s, the number of applicants began to decrease, and the number of U.S. graduates of general surgical programs declined from 1,381 to 931: For the first time, a number smaller than the number of positions offered, by about 100. However, since 2002, this trend has not worsened. Figure 1 shows the relatively steady number of positions filled in general surgery since 2006, with 1,075 positions offered and filled in 2010. The increase in positions is notable both in emergency medicine, now outnumbering positions in surgery by about 500, and in anesthesiology, which still is fewer than surgery but having increased substantially over the last four years.
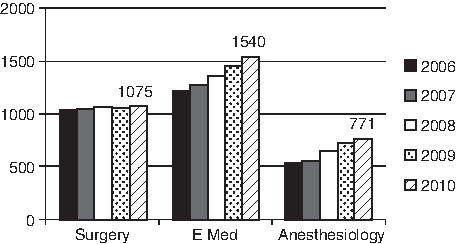
Number of applicants to residency programs in surgery, emergency medicine, and anesthesiology.
Do we understand why these changes have occurred? Do we still have a problem attracting students? Are surgical training programs getting the best students? How do we define the best students? If we consider the U.S. Medical Licensing Examination (USMLE) scores in Step I, the mean score for U.S. seniors who matched in their specialty was 225, and the general surgery applicants' mean score was 224 [15]. For USMLE Step II, general surgery applicants were also at the national mean of U.S. seniors applying successfully. Applicants to both anesthesiology and emergency medicine training programs were similar to general surgery applicants [15]. General surgery training programs attracted 30.9% of their applicants from one of the top 40 U.S. medical schools with the highest National Institutes of Health funding, 2.9% of applicants had a Ph.D., and 9.9% had another advanced degree. Again, these numbers are similar to those of the applicants in anesthesiology and emergency medicine. The most competitive specialties are plastic surgery, with mean Step I and II scores of 245; dermatology at 242 and 251, respectively; otolaryngology at 240 and 246; diagnostic radiology at 238 and 242; orthopedic surgery at 238 and 241; radiation oncology at 238 and 241; and neurological surgery at 239 and 237. Applicants in the other major specialties, internal medicine, pediatrics, and obstetrics and gynecology, were similar to those in general surgery [15]. Thus, whereas selected programs may attract applicants similar to those in the most competitive specialties, the average general surgery applicant from a U.S. medical school is, by the criterion used across specialties to screen and select applicants, similar to those in most of the other large specialties. In particular, the general surgery applicants are similar to those in the specialties that may be considered to have a more attractive lifestyle such as anesthesiology and emergency medicine.
Aside from perceptions of lifestyle, students and residents may consider other factors in selecting a career such as the cost of higher education and the ability to repay loans, the geographic location of their specialty, perception of career satisfaction, and the changing political and social climate of medicine, to name a few. Further, the demographics of students entering medical school has changed substantially, with women now accounting for almost one-half of the student body. Park et al. identified both real and perceived barriers to female students applying to general surgery [16]. In this Canadian study in 2004, the perceived barriers included gender-based discrimination and a lack of female role models. Students believed that general surgery was inconsistent with a rewarding family life, a happy marriage, and having children. Yet female surgeons surveyed at the same time did not share these concerns [16].
One might ponder whether student interest in selecting non-surgical careers is influenced by many of the same factors observed in studies of students concerning surgical careers. DeZee et al. surveyed all fourth-year students who had a Department of Defense commitment with questions about primary care careers and whether financial considerations influenced their career plans [17]. Two-thirds of the respondents did not apply for primary care, yet 30% of this group stated they would have if they had been given a median bonus of $27,5000 (interquartile range [IQR] $15,000–$50,000) before and after residency. Further, 41% of the students stated they would have applied for a military primary care residency if they had a median military salary after residency of $175,000 (IQR $150,000–$200,000). Interestingly, students who choose a non-primary-care specialty with a controllable lifestyle (e.g., radiology) were more likely to be influenced by this hypothetical salary increase than students who selected a non-controllable lifestyle such as surgery [17]. Thus, it seems that for some students, at least those in whom a military commitment was present, financial considerations were important in selecting a career. However, the minority who were interested in surgery could not be influenced by a financial reward to change to primary care! Perhaps we are a rare but “stable” breed?
But are money and lifestyle what is important to current students? Recruiting students into surgery who are not well suited to the specialty can be associated with a high attrition rate, either because programs make unfavorable decisions about residents or residents determine that a surgical career does not match their life plans. Naylor et al. examined the results of their 115 categorical residents who matched in their general surgery training program and identified success as those residents who completed training and passed the ABS examinations on the first attempt [18]. There were 25 individuals (22.5%) who did not complete training and three who did not pass the Board examination on the first attempt. Ten of the residents separated from the program because of performance issues, with the remaining residents leaving the program when they changed their minds because of a desire to train in another specialty (n=7), lifestyle or family issues (n=3), marriage (n=4), or health (n=1) [18]. The authors suggested that applicants older than 29 years of age, lack of superlative comments in the summary in the Dean's letter, no participation in team sports, and having a merit scholarship in medical school were predictive of attrition from this program. Although these findings may be unique to that particular surgery program, we do know that attrition rates in categorical surgical programs are running between 15% and 20%. In the 2007–2008 resident survey data, the only factor that could be identified with attrition from general surgery training programs was postgraduate level, with the highest rates of attrition in postgraduate years I–II and in the research years [19]. Do we have to worry that general surgery will become a forgotten specialty and that as a small unidentified group, we in the SIS will languish as well?
In the seminal report by Yeo et al. surveying 4,402 current surgical residents, 31.7% of the residents were women [20]. Those authors found that a number of differences in the survey answers depended on the gender of the resident. Fewer female trainees were satisfied overall with their training (86.6 vs. 82.2% male vs. female, respectively), and more women considered leaving training (19.1% vs. 13.6%). Fewer female trainees thought support was available when they were struggling (66.6% vs. 74.5%), and that they did not believe they could turn to faculty when they had difficulties (66.4% vs. 74.5%). Furthermore, fewer female residents were likely to think that they could count on other residents to help them (82.1% vs. 85.2%). Female residents were more worried about whether they would be confident to perform at the end of their residencies (37.9% vs. 22.5%). Male residents noted more commonly that expectations about good financial compensation influenced their decisions (38.0% vs. 21.7%), and they also were more worried that other professionals would take over (62.5% vs. 55.5%). Interestingly, male trainees also believed the training was too long (22.0% vs. 17.2%). Many of the concerns of residents were noted in the PGY II and PGY III years of training [20]. This study demonstrated that although most surgical trainees are satisfied with their experiences, some residents experience difficulties in their middle years of training. Further, this study suggests that the residency training experience in surgery may differ for male and female residents, and program directors should be aware of these potential differences.
Why Are There Fewer Applicants to Surgery Programs?
Let us now return to the question of whether we have any understanding of why applicants have moved away from surgery and what, if anything, we can expect from our current residents in the future. To help examine this issue, we will turn to some data on the generational differences among those of us who have been in practice more than 20 years, those just beginning their practices, and those in training [21–25]. These issues may have a profound impact on the organizations and associations our future colleagues will choose.
First, we will define the terms used to describe the generations. “Veterans” are those individuals born between 1900 and 1945. This generation was influenced during childhood by the Great Depression, World War II, and a feeling of patriotism. Prominent members of this generation include Lee Iacocca, George Herbert Walker Bush, Jimmy Carter, and John Glenn [25]. The defining trait of this generation is said to be loyalty, and they value consistency, respect for the law, and a job well done. Their management style consists of a military chain of command. Our founding fathers were of this generation and established this Society on firm grounds. Among the 388 members on whom we have a record of the date of birth, we have 45 “veterans.”
Many of our members are of the Baby Boom Generation, born between 1945 and 1965. As a generation, we were greatly influenced by the Cold War, prosperity, television, the space race, civil rights activism, and the Vietnam War [25]. Our defining trait is optimism, and we are said to value growth and expansion. Because we grew up during a period of prosperity, we are said to believe anything is possible. Prominent members of this generation are Bill and Hillary Clinton, Oprah Winfrey, and Bill Gates [25]. The management style of the Baby Boomers is change of command; new leaders are accepted as a matter of growth. Many in the audience, our most recent leaders, have been of the Baby Boom generation. Of those on whom we have data, Baby Boomers are a large group, at 140.
A smaller group nationally than the Baby Boomers is the group born between 1965 and 1980. They have been named Generation X (Gen X). During their childhoods, they were influenced by the fall of institutions, political scandals, divorce, latchkey life, the Music Television Channel (MTV), acquired immunodeficiency syndrome, and computers. Michael Jordan and Kurt Cobain are (were) prominent members of this generation [25]. Their defining trait is skepticism, and they value work–life balance, short-term employment, and self-command as a management style. Our largest recorded group of members is Generation X, at 190. Whether this large number is based on a bias of data collection is not clear. Is the SIS now defined by Generation X, and, if so, have we met their needs?
The Millennials, also called Generation Y, have been influenced by multiculturism, school violence, competition, mass media, and the technology boom. Mark Zuckerberg and Prince William are prominent members of this generation. They have a defining trait of realism. They value education and technology, and they embrace challenges. They believe in collaboration as a management style [25]. Not surprisingly, this is a small group of our current membership, at only 10 identifiable members, but they are our future.
Millennials are demographically more diverse [21]. When comparing what is most important to this generation with what is important to those over age 30, being a good parent and a high-paying career were considered most important. Millennials are much less likely to be married early in life; they are still single and never married between 18–28 years of age. When compared with the other generations, they are much more likely to use a social networking site, to use wireless tools when away from home, to enter videos of themselves on an on-line video site, and to use Twitter [21]. Millennials are likely to visit a social networking site one or more times a day vs. once a week for Baby Boomers [21]. Millennials are much less likely to stay at their current jobs, with progressive differences between their generation and Generation X and the Baby Boomers [22,23]. Will this generation's members stay with an association? What will hold their attention?
In the workplace, these generational differences may cause conflict [22,23]. Veterans and Baby Boomers may have fundamental differences in their job expectations and priorities; seeing the job as a vocation, whereas Gen X members may see the job simply as a day activity. Generation X may have a desire for independence and a lack of respect for authority. However, their independence is one of their greatest assets. They are highly motivated and independent learners, and they are not dependent on continuous feedback [21–23]. They value efficiency, economy, and change. They will want to lead, and our Society must be ready and willing to let them bring forward their ideas and changes. I call on this group of younger members to lead.
When dealing with management or authority, the conflicts with Generation Y may differ [22]. Members of Generation Y require instant communication and feedback. As a group, they are impatient for advancement and change [22]. They desire collaboration, yet they are socially bold and are not afraid to ask questions and perhaps even less afraid to give their opinions. For those in the older generations, these traits can feel like lack of respect and thus cause conflict. This younger generation can be impatient when mastery of skill is required. Because they have a desire to pursue multiple interests, their dedication may be questioned. Millennials may delay career and life decisions as they pursue their multiple interests [21,22]. Will this group be willing to join a society early in their careers, or will they try different societies and associations first? Will membership be durable? Do we know enough about the durability and engagement of our own membership?
Are We Ready?
Why did I choose to speak about a tipping point in surgical training and generational differences during my Surgical Infection Society Presidential Address? Simply put, I am not sure we are ready for the changes that may be coming. For the last 30 years, this Society has had wonderful leadership and has accomplished much. During the first decade, it had a period of rapid growth in membership, faced up to many of the challenges, and was dedicated to our mission statements. Founding member Doctor J. Wesley Alexander, in his Presidential Address in 1986, set forth five challenges, which he reviewed a decade later. Let us reconsider his five challenges now, 25 years later [26].
Challenge 1 was to ensure the lowest possible surgical site infection rate in our patients. Doctor Lena Napolitano addressed this issue in her address two years ago, so I will comment only briefly [27]. Today, we have the Surgical Care Improvement Project, checklists, pay for performance, and public reporting, yet can we honestly say we have the lowest possible infection rates? Are the rates of surgical site infections in colorectal surgery and pancreatic surgery the lowest they can be? Have we considered all of the biologically plausible factors to study and improve? Are surgical site infections really inevitable in some patients? Some of our non-surgical colleagues have been creative in studying aspects of infection we did not consider, such as normothermia, oxygen, and glucose effects. Have we exhausted our questions and maximally developed our technology to help fight surgical site infections? Have we lost interest in this issue because of our success?
Doctor Alexander's second challenge was to expand the international scope of the society [26]. I would like to take this moment to remember those who have perished and suffered in the tragedies around the world, especially those recently in Japan. In the past, we have had joint meetings with the Surgical Infection Society–Europe and have asked our colleagues in Japan to join us. But have we maximized our international membership when we consider that technology has made the world a smaller place? Have we thought about fully utilizing technology for our future meetings to reach international members simultaneously?
Challenge 3 was to build the membership by self-expansion [26]. In 1986, there were 315 members. We now have 533 members. Yet, in the last decade, our membership has been stable, not growing. Do we understand our membership sufficiently to know that we are meeting their needs? We have a small, dedicated group of members who attend the Annual Meeting, typically about 25% of the membership. Do we know whether the same small group attends our Annual Meetings year after year? What will happen as this group ages? Will we be able to bring in new members? Our membership typically has been from general surgery, yet surgical practice has changed dramatically over the last 30 years. Today, virtually all residents are selecting fellowship training. As a Society, have we planned for this specialization and attracted those with a special interest in surgical infections? Does our membership need to be those with a special interest in surgical infections, or can we attract a more general audience? How do we make surgical infections relevant in 2011 and beyond? Will our more fleeting interactions with residents affect their interest in our area? I say we need to understand our membership better than we currently do.
Doctor Alexander pointed out that critically ill and injured patients with sepsis and multiple organ dysfunction during their hospital stay are highly relevant to members of our Society [26], but these patients and their fundamental problems also are relevant to the members of other societies, such as the Society of Critical Care Medicine and the Shock Society, to name but a few. Doctor John Marshall encouraged us to consider our alliance with acute care training and practice [28]. Have we optimized this association? What could we do as a Society to make us more relevant? Because surgical infection is not a specialty of itself, our expertise is scattered through core surgical training and is focused in acute care and critical care training, but our content also is present in every surgical specialty. Can we become more relevant to surgical education and training by being more active in core residency training? Two of our members have partnered in the development of modules for the SCORE Project dealing with basic aspects of surgical infection. Past President Doctor Michael West and Doctor Raul Coimbra have authored several sections of SCORE. Just a few weeks ago, Doctor Mary Klingensmith notified program directors that SCORE would be expanding to include fellowship materials. Having advanced material on surgical infections, the pathophysiology of sepsis, and inflammation available for residents may encourage their interest in surgical infections. I ask the Education and Awards Committee to review both the General Surgery and Surgical Critical Care curricula and consider whether we should volunteer to develop modules with advanced content for SCORE. We surely have all of the experts we need in this Society to educate our residents and fellows.
Perhaps it is in the area of membership that we should consider the possibility of disruptive innovation and combine this with education and the tipping point in residency education. There is no doubt that our healthcare system will change dramatically in the coming years. We must reduce costs, and we must embrace the idea of disruptive innovation [29]. What is disruptive innovation? In his book The Innovator's Dilemma, Christensen defines disruptive innovations as “cheaper, simpler, convenient products of services that start by meeting the needs of the less-demanding customers” [30]. Has what the SIS offered in our meetings and journals focused on meeting the needs of physicians and scientists and the high end of the market at the cost of missing the simpler, more convenient, and less costly potential members and services? Should we be offering alternatives designed to appeal to the least demanding members at the low end of the marker?
Let me provide an example of disruptive innovation from the airline industry. Southwest Airlines provided a low-cost, no-frills alternative to paying “through the nose” or not traveling at all [29]. Of course, they rapidly took market share from established carriers and brought new travelers to the airlines.
The central keys to successful disruptive innovation for us are:
• To know our current and potential members, not just from a demographic standpoint, but also from a lifestyle point of view; • To recognize what business we are in and how we contribute strategically to the betterment of society by our distinction; • To be innovative in what we do in a way that is valued by the people we serve and aligns with our core principles and competencies; • To have a culture that encourages innovation as a core principle of our society; • To reach for excellence and raise the expectation of what excellence is among all that work with us; • To use technology as a tool that encourages value and innovation; and most importantly: • To have the moxie to be different in a way that shifts the paradigm of what is, so that our contribution improves society [29,30].
Challenge 4 was to increase our interactions and bonds with basic scientists [26]. Surely, our Society has shown great strength in presenting outstanding basic science each year at our Annual Meeting and in our support of young surgical scientists. Several years ago, we developed two parallel tracks at our meetings to allow additional focus on basic or clinical science. Have we investigated formally whether this change has been beneficial to our membership? Our abstract submission rate has increased slightly in recent years. Have we surveyed our membership about what, if any, changes should be made to the Annual Meeting? Could we attract additional attendance and membership by joining with other groups for simultaneous or adjacent meetings such as has been done during Digestive Disease Week? We need to have a clear and comprehensive strategic plan for the next five years, and we need to ensure our tactical plans fit with this strategic plan. We need to ensure that this plan satisfies the needs of our membership and considers the changes in our potential members and what they will experience in residency training. We also need to be aware of the potential threats to our Society from external forces or political changes.
One of these external threats is addressed by the fifth challenge offered by Doctor Alexander [26]. This challenge is perhaps the most controversial in today's times of conflict of interests and industry relationships. Over the years, our Society has greatly benefited from activities with industry. These activities have included scientific contributions to our meetings through our peer-review process, contributions to our Foundation for the support of research grants to our young members, and support of educational symposia. Given the political pressures on associations to sever relationships with industry, we must ensure that we remain transparent in our actions with our corporate sponsors. However, we must also recognize the great benefits that have come over the years from the SIS Foundation grants. The awardees have contributed routinely to our Society during and after their awards. This year, we had 24 grant applications submitted, verifying that we do have ongoing interest in our field and in the scholarship attached to discovery. We are appreciative of the work of Doctor Craig Coopersmith and of the Fellowship and Grants Committee. Doctor Heather Evans and her Information Technology Group have highlighted some of the contributions of these award recipients on our website. We should quantify the important contributions of our recipients and acknowledge the continuing importance of our Foundation. Our Society is truly remarkable in the degree of support it has generated for scholarships each year, and we must continue to support the Foundation. I challenge every person here today to donate to our Foundation. Today, right now, make a contribution. I have donated and hope each of you will do the same.
Just five years ago, in his Presidential Address, Doctor Edward Deitch queried “Is the Glass Half Full or Half Empty?” and warned that American surgery, and the SIS in particular, may be in the midst of an identity crisis as the traditional values we have held as surgeons may not be valued by others [31]. For example, our ability to make quick decisions may be viewed as not being collaborative and willing to be part of a team [31]. Our past dedication to our patients and careers may be in direct conflict, not only with the 80-h work week, but with the generational differences I have discussed. These differences may well alter the willingness of our youngest colleagues to participate in Society activities, and how they participate may differ greatly from the past. The SIS and American surgical leaders must recognize these fundamental changes in our applicants and must step forward to acknowledge the challenges we face. In preparing for his Presidential Address, Doctor Deitch sent a survey to our membership [31]. Now, more than six years later, I will be charging our Membership Committee and Executive Director to perform another, more comprehensive survey of our membership; and I propose a study of potential members from the senior residency years. I think we need to be disruptive; we need to reach out to mid-level practitioners. We should invest in a greater understanding of these issues to help us chart our future through these potentially turbulent waters.
Conclusion
I titled this talk “Passing in the Night: A Tipping Point in Surgical Training” because we are at a crucial time, when the fundamental structure of our training programs for junior residents is changing. We need not consider this a grim and fatal blow for our field. Past President Doctor Steven Lowry spoke of mentors and our connectedness to others [32]. We know who the Connectors have been in our society, but we need to develop a Maven trap, whereby surgical residents will be attracted to who we are and what we do. Will we accomplish this by working side by side with them during the night, in research laboratories during academic time, or by meeting and mentoring them in other ways? We must take the opportunities we have with residents and turn them into epidemics.
None of us will be here forever. Gladwell tells us that Ivory Soap identified “Soap Mavens” by putting their telephone number on the soap bar, knowing that only those who really cared about soap would call and that these same callers would be people who others asked about soap [1]. How will we identify our SIS Mavens? Will our tactics and strategies develop immunity to post-residency societies and associations, or we will be able to have an SIS epidemic?
I challenge our members—those in primary laboratory work and those in clinical and administrative work—to consider how we will keep the SIS relevant and vibrant in the years following. We must use our collective Connections to keep the “Stickiness” we need in this time of both generational and surgical residency change. The mission and vision of the SIS is as relevant today as it was 31 years ago when our founding fathers brought us together.
As was true for those who have gone before me, it is a great pleasure and honor to have been selected to serve as your president this year. Since this honor is never granted to the one standing at the podium alone, I want to spend a moment to thank a few people who have greatly influenced my interest and enthusiasm for this society. I thank Doctor Adrian Barbul for telling me about this Society and inviting me to my first meeting. To Doctors Donald Fry, E. Patchen Dellinger, Irshad Chaudry, Ori Rotstein, and John Marshall, who never failed to speak to me and about my interests, thank you for making me feel welcome and for serving as inspiring mentors for so many. I thank Doctors Philip Barie and Lena Napolitano for their friendship and close counsel. I thank our Executive Director, Lynn Hydo, and her team for their hard work and wish her well in her fight for good health. To the many members of the Education and Awards Committee, the Program Committee, and the Council with whom I have served over the years, I thank you for the past and future success of the Society and for your support.
I must thank the many students, residents, and fellows who have wanted to study surgical infections so they could come to this meeting, often for their first presentations. You have always been very courteous in asking them questions and in your collegiality. I thank my colleagues at Johns Hopkins who have always supported my passion for infection prevention and infection studies. I thank Sandy Swoboda, who serves as my research program coordinator and dear personal friend. Most of our presentations here would not have happened without her. Finally, I wish to thank my many patients, whether passing in the night or in the light of day. I continue to serve and learn from them every day.
Footnotes
Author Disclosure Statement
The author has no potential conflicts of interest related to this article.