
Abstract
Abstract
Background:
We evaluated drug efficacy and safety among patients with and without vascular disease who were treated with linezolid or vancomycin for a lower-extremity complicated skin and skin structure infection (cSSSI) caused by methicillin-resistant Staphylococcus aureus (MRSA).
Methods:
We pooled data from two randomized clinical trials evaluating the efficacy and safety of linezolid 600 mg intravenously (IV) or orally every 12 h and vancomycin 15 mg/kg or 1 g IV every 12 h for the treatment of cSSSI caused by culture-proved MRSA.
Results:
There were 477 patients for analysis. Among patients with vascular disease (linezolid n=139, vancomycin n=135), the clinical success rate was 80.4% and 66.7% (p=0.02) for patients treated with linezolid and vancomycin, respectively. Among patients without vascular disease (linezolid n=91, vancomycin n=112), the clinical success rate was 94.5% and 89.4%, respectively (p=0.24). Linezolid-treated patients had fewer IV catheter-site complications and less kidney impairment but more frequent thrombocytopenia than those who received vancomycin, regardless of the presence or absence of vascular disease.
Conclusion:
Linezolid is an effective treatment for patients with and without vascular disease who have a lower-extremity cSSSI caused by MRSA. The safety data were consistent with the known safety profiles of linezolid and vancomycin given for this indication.
Patients and Methods
We pooled data from two randomized clinical trials [9,10] evaluating the efficacy and safety of linezolid 600 mg intravenously (IV) or orally every 12 h and vancomycin 15 mg/kg [9] or 1 g [10] IV (dose adjusted for creatinine clearance) every 12 h for 7–28 days for the treatment of cSSSI caused by culture-proved MRSA. We included all patients ages 18 years and older with a lower-extremity cSSSI caused by MRSA. On the basis of the patient's medical history and physical examination at trial entry, the investigators identified patients with and without vascular disease and lower extremity cSSSI through check boxes on the case report forms. There was a third prospective open-label clinical trial that evaluated the efficacy and safety of linezolid and vancomycin in the treatment of suspected or proved MRSA infections, which was completed in 2003. Data from this trial were not included in the pooled analysis because of the small number of patients who met the inclusion criteria for this study, specifically, proved MRSA and lower-extremity infection, and the differences in the classification of vascular disease status, the main exposure variable.
The patients included in this study had signs or symptoms of a cSSSI involving deep tissues and at least two of the following: Purulent drainage, erythema, swelling or induration, tenderness or pain, and local warmth. In addition, patients had at least one sign of systemic infection, such as fever, hypotension, increased white blood cell count (≥10,000 mm3), or more than 15% immature neutrophils regardless of the total peripheral white blood cell count. Specific enrollment criteria were applied for patients with diabetic foot infections, which included evidence of a deep infection extending below the subcutaneous tissue of the foot, ankle, or lower leg that necessitated a surgical procedure. Alternatively, patients with diabetic foot infections could be enrolled if there was an identifiable wound, such as an open lesion, ulcer, or puncture, with evidence of purulence and either erythema of more than 50% of the surface area of the foot, ankle, and lower leg or medial arch streaking.
Patients with known or suspected necrotizing fasciitis, gangrene, septic arthritis, or osteomyelitis or who were treated previously with an MRSA-active antibiotic were excluded from the original clinical trials; therefore, data on these types of patients could not be included in this analysis [9,10]. The presence of MRSA was confirmed by wound specimens obtained within 24 h of enrollment. Acceptable specimens included deep cultures from normally sterile sites, aspirations, and biopsy samples or scrapings from wounds. The study protocols disallowed culture specimens obtained by a superficial swab.
We examined the clinical and microbiologic success rates and predictors of clinical failure among patients with and without vascular disease who were treated with linezolid or vancomycin for a lower-extremity cSSSI caused by MRSA at end-of-study (EOS; 6–28 days after the end of therapy). Missing or unknown values were excluded from the clinical response and the microbiologic outcome analyses. A central laboratory provided the final pathogen identification and determined susceptibility to study drugs by broth microdilution, according to the Clinical and Laboratory Standards Institute guidelines. The clinical response at EOS in each study was defined as one of three categories:
• “Clinical success”: Resolution of all clinical signs and symptoms of infection identified at baseline; • “Clinical failure”: Persistence or progression of clinical signs and symptoms of infection after at least two days of treatment or development of new clinical findings consistent with active infection; and • “Unknown”: Extenuating circumstances that precluded any other classification.
The microbiologic outcome at EOS was defined as one of the following:
• “Microbiologic success”: Repeat culture from the original infection site with no MRSA isolated or no culture data but a clinical outcome defined as success; and • “Microbiologic failure”: Repeat positive culture for MRSA from the original infection site; no culture data available but clinical failure; or a positive culture for MRSA from the original infection site at EOS when a culture was negative at the end of treatment.
Statistical comparisons between groups were performed using the chi-square test for categorical variables and one-way analysis of variance for continuous variables. Logistic regression was used to assess the relation between baseline covariables and the probability of clinical failure at EOS for all patients and separately for patients with and without vascular disease. For each patient population, the analysis was conducted in two steps: Covariable screening and final model building. At all stages of the analysis, cases with missing observations on either the outcome or covariable(s) were excluded, except for prior hospitalization, where a “missing” category was created because of the high frequency of missing data to retain more patients in the final model. Covariables with a p value≤0.25 met the screening criteria and were used in final model building. All covariables meeting the screening criteria were added in a multi-variable model and reduced by backward elimination. The Breslow-Day test was used to assess homogeneity between the studies for clinical and microbiologic success by treatment group and by vascular disease status.
Results
In total, 477 patients with lower-extremity cSSSI caused by MRSA were included in the analysis. Compared with patients without vascular disease (n=203; 42.6%), patients with vascular disease (n=274; 57.4%) were more likely to be older and heavier and to have co-morbidities (diabetes mellitus, renal impairment, coronary artery disease, hyperlipidemia), polymicrobial infections (MRSA–mixed), and infected ulcers (Table 1). Among patients with vascular disease, there were no differences in baseline demographics or clinical characteristics between treatment groups. Among patients without vascular disease, more linezolid-treated patients were female (39.6% vs. 22.3%, respectively; p<0.01), had a higher prevalence of prior hospitalization (44.2% vs. 25.7%, respectively; p=0.03), and were treated longer (11.5 vs. 9.5 days, respectively; p<0.01) than vancomycin-treated patients. Homogeneity between the studies was demonstrated with the clinical and microbiologic success by treatment group and by vascular disease status, therefore allowing comparisons among the defined subgroups.
Variable collected in only one of the two pooled studies; sample sizes indicated.
CAD=coronary artery disease; IV=intravenous; SD=standard deviation.
Among patients with vascular disease, the clinical success rate at EOS was significantly higher among linezolid-treated patients than among vancomycin-treated patients (80.4% vs. 66.7%, respectively; p=0.02) (Fig. 1), and microbiologic success was numerically more common among linezolid-treated patients than vancomycin-treated patients (68.0% vs. 56.9%, respectively; p=0.07) (Fig. 2). Among patients without vascular disease, clinical (94.5% vs. 89.4%, respectively; p=0.24) (Fig. 1) and microbiologic (78.3% vs. 67.3%, respectively; p=0.10) (Fig. 2) success rates at EOS were similar among linezolid- and vancomycin-treated patients.

Clinical success of lower-extremity complicated skin and skin structure infection caused by methicillin-resistant Staphylococcus aureus among patients with and without vascular disease by treatment at end of study.a
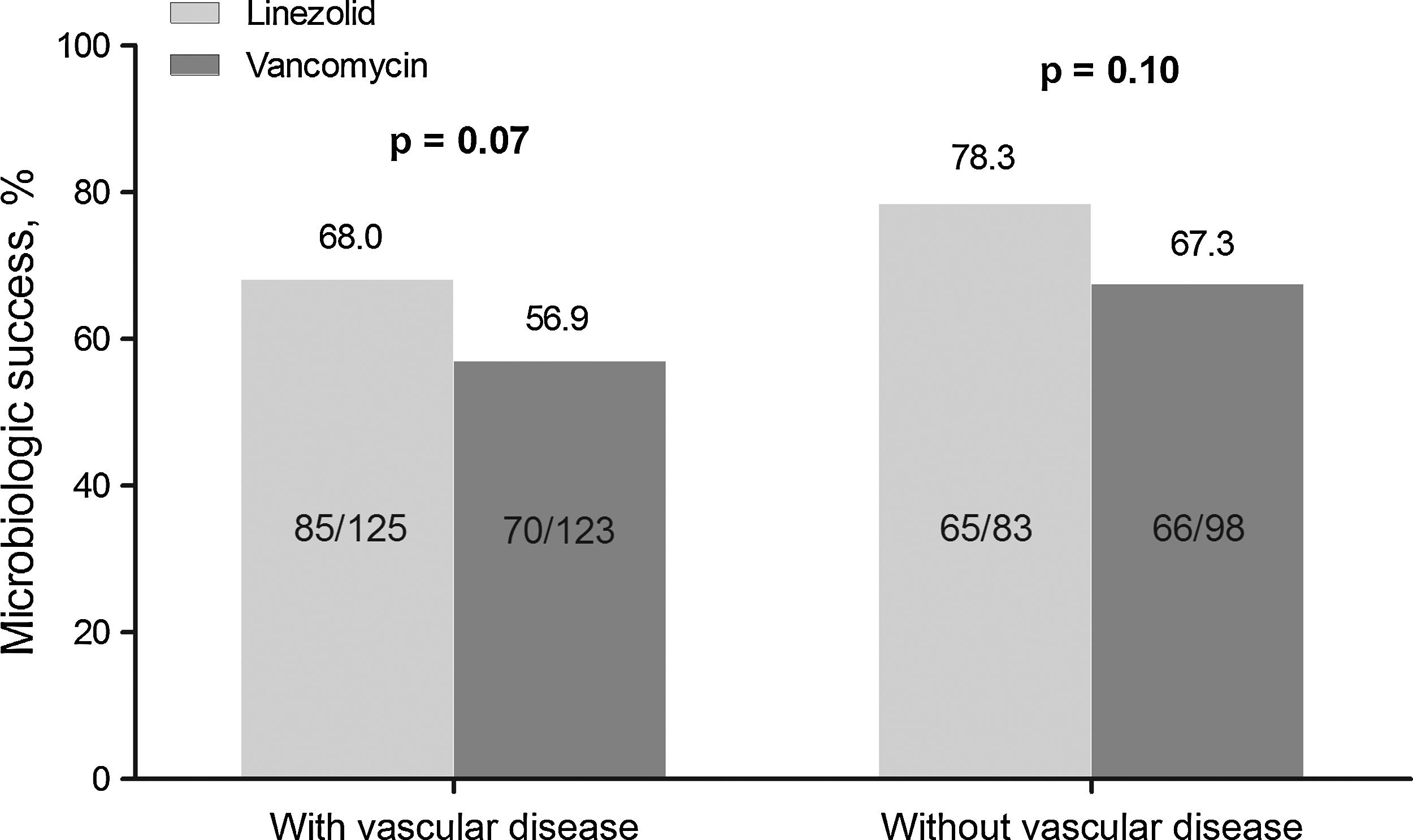
Microbiologic success of lower-extremity complicated skin and skin structure infection caused by methicillin-resistant Staphylococcus aureus among patients with and without vascular disease by treatment at end of study.a
In patients both with and without vascular disease, the majority of infections were MRSA only. However, the patients with vascular disease had a higher prevalence of polymicrobial infections (32.1%) than patients without vascular disease (19.7%). Among patients with vascular disease, 29.2% (linezolid n=47; vancomycin n=33) of patients had a diabetic foot infection caused by MRSA. Among these patients, neither clinical nor microbiologic success at EOS was significantly different among linezolid-treated patients versus vancomycin-treated patients (clinical success rate 71.1% vs. 69.0%, respectively; p=1.00; microbiologic success 57.5% vs. 58.1%, respectively; p=1.00). Among patients without vascular disease, 4.9% (linezolid n=6; vancomycin n=4) of patients had a diabetic foot infection caused by MRSA. Among these patients, the numbers were too small to draw any conclusions (clinical success 100% [4/4] and 100% [4/4] for linezolid and vancomycin, respectively; microbiologic success 80% [4/5] and 75% [3/4], respectively).
Multivariable logistic regression modeling identified factors associated with a clinical outcome of failure at EOS for patients with lower-extremity cSSSI caused by MRSA. For all patients, vascular disease (odds ratio [OR] 4.2; 95% confidence interval [CI] 2.21, 8.05) and vancomycin treatment (OR 2.0; 95% CI 1.19, 3.52) were associated with clinical failure at EOS. Among patients with vascular disease, vancomycin treatment (OR 2.2; 95% CI 1.17, 4.08) and prior hospitalization (OR 2.8; 95% CI 1.25, 6.09) were associated with clinical failure at EOS. Among patients without vascular disease, there were no variables significantly associated with clinical failure at EOS.
Compared with patients without vascular disease, patients with vascular disease had a higher frequency of one or more adverse events, serious adverse events, and adverse events leading to study drug discontinuation (Table 2). The reasons for discontinuation were consistent with what is expected, but given the small numbers, no trends could be identified. For patients with and without vascular disease, linezolid-treated patients had fewer IV catheter-site complications and less kidney impairment but more frequent thrombocytopenia than vancomycin-treated patients (Table 2).
AE=adverse event.
IV=intravenous.
Discussion
To our knowledge, this is the first trial to evaluate the outcomes of patients with and without vascular disease treated with linezolid or vancomycin for lower-extremity cSSSI caused by MRSA. We found that both the clinical and the microbiologic success rates were lower in patients with vascular disease. Although the clinical and microbiologic success rates were similar between treatment groups, for patients without vascular disease, they were higher for patients with vascular disease who were treated with linezolid than for those receiving vancomycin. These findings may be explained by linezolid's excellent tissue penetration [11,12] and effectiveness in the treatment of multi-drug-resistant MRSA even when concentrations at the infection site are diminished because of impaired blood flow [13].
There are several possible explanations for the outcome differences between patients with and without vascular disease. Patients with vascular disease have an impaired blood supply, which can impair tissue viability and wound healing and limit the delivery of neutrophils to the infected area. A poor vascular supply also can result in poor delivery of antibiotics to infected tissues [14,15]. More of our vascular patients had diabetes mellitus, which commonly is associated with macrovascular disease below the knee as well as with microvascular disease of the tissues [16]. This vascular disease pattern has the potential for limiting drug delivery to lower-extremity tissues. Diabetes mellitus increases the risk of vascular disease three- to four-fold [17]. Peripheral vascular disease in diabetic patients is one reason these patients have a five- to ten-fold greater need for major amputation than do non-diabetic patients with peripheral vascular disease [16]. Our vascular-disease patients also had more diabetic foot infections. Diabetes mellitus is associated with peripheral neuropathy and decreased resistance to infection, both risk factors for foot ulcers and infections [17]. Furthermore, the patients with vascular disease were more likely to have mixed infections, particularly with gram-negative pathogens, which may correlate with the high prevalence of diabetes mellitus and diabetic foot infection in this population. Gram-negative coverage should be considered in the treatment regimens for this population. Renal impairment and cardiac disease also were more common among the vascular-disease patients. Renal impairment can alter host defenses, and cardiac disease can produce peripheral edema, both of which could increase the risk of infection and limit treatment effects [18]. Another possible explanation for the differences between the two groups is the type of infection. Patients with vascular disease had more infected ulcers and fewer abscesses than patients without vascular disease. Abscesses generally are easier to cure, as surgical drainage is a major part of their treatment. It is possible that the vascular disease results in reduced ability of the host to localize the infection, which leads to fewer abscesses and greater numbers of ulcerations.
In this study, the percentage of patients with adverse events, including those that were serious, was higher in patients with vascular disease in both treatment groups. The higher risk of adverse events among patients with vascular disease is explained by non-drug–related events (i.e., adverse events associated with underlying co-morbidities such as diabetes mellitus, renal impairment, or coronary artery disease). The overall safety profiles of linezolid and vancomycin were similar in patients with and without vascular disease. Drug-related thrombocytopenia was identified among 4.3% and 2.2% of patients with and without vascular disease treated with linezolid, respectively. In linezoid-treated patients, the mean±standard deviation time to thrombocytopenia was 16.0±5.9 days and 14.5±4.9 days, respectively, among patients with and without vascular disease. Drug-related IV catheter-site complications and renal impairment were observed more frequently in vancomycin-treated patients. The catheter-site complications may have been secondary to the longer duration of catheter use among patients treated with vancomycin. The ability to use an oral formulation (i.e., linezolid) may reduce this complication.
The limitations of this evaluation include those inherent in all retrospective pooled analyses. Simple pooling of patients from the two trials could lead to underestimation of standard errors because it ignores potential heterogeneity across studies (when generalizing beyond these two studies); however, a heterogeneity test of treatment across studies did not demonstrate significant differences (p>0.30). In our analyses of two randomized clinical trials with predetermined endpoints of clinical and microbiologic response rates, linezolid did not demonstrate superiority over vancomycin for these endpoints in either study. For these reasons, the results of the analyses presented here are considered suggestive, not definitive.
Surgical care was not specifically defined in these two studies; therefore, source control of infection could not be compared. The lack of surgical intervention data is a potential confounding factor that could not be assessed in the outcome analysis. We admit it could be a factor, as there were more abscesses in the patients without vascular disease and more ulcers in the vascular-disease group. However, the distribution between treatment groups was similar for patients with and without vascular disease. Whether this diagnostic variation would produce a significant difference in source control between the groups is unknown. However, although source control clearly is an important issue for many infections, in cSSSIs, it probably is not as important as it is in organ-space infection such as in the abdominal cavity [23]. Source control for abscesses usually is fairly simple and effective. Source control for ulcerated lesions may not be a major issue, as the wound is open and, usually, draining already.
Vancomycin dosing was different in the most recent study (15 mg/kg every 12 h) [9] from that in the other study (1 g every 12 h) [10]. However, the clinical success rate in the most recent study (64.2%) [9] was similar to that in the other study (70.2%) [10]. Furthermore, in the most recent study [9], there was no correlation between vancomycin trough concentrations and clinical outcome or microbiologic outcome at EOS. These results are consistent with published findings [19,20]. We lacked a definitive diagnostic procedure for the classification of vascular disease and relied on the clinical assessment by the investigators at study enrollment based on checked boxes from the case report forms. Although there is a potential for selection bias, there were 63% and 41% of patients with a diagnosis of diabetes mellitus and coronary artery disease, respectively.
In summary, in this pooled analysis of two randomized, controlled trials of patients with cSSSI caused by MRSA, clinical and microbiologic success rates were lower in patients with vascular disease than in those without vascular disease. The clinical success rates were similar for patients without vascular disease treated with either linezolid or vancomycin but were higher with linezolid treatment among patients with vascular disease. The demonstrated benefit of linezolid in this group of patients can guide physicians in their antimicrobial selection to optimize patient outcomes, thereby avoiding further complications such as IV catheter-site problems, renal impairment, and possibly amputation [16,21,22]. This analysis provides useful data on the treatment of lower-extremity cSSSI caused by MRSA based on the patient's vascular disease status.
Footnotes
Acknowledgments
The study was sponsored by Pfizer Inc. Programming support was provided by Diane Ruzzi, of Pfizer Inc. Editorial support was provided by Lisa Baker of UBC Scientific Solutions and was funded by Pfizer Inc.
Author Disclosure Statement
TMD and JAW are consultants for Pfizer Inc. TMD and JAW were not paid for their contributions to this manuscript. LAP is an employee and shareholder of Pfizer Inc. DBH was an employee and shareholder of Pfizer Inc at the time the study was conducted.
a
Missing or unknown values were excluded from the analyses.
a
Missing or unknown values were excluded from the analyses.