
Abstract

A 58-year-old female presented with immobilizing lower back pain, fever, and chills. The patient had undergone multiple gynecologic operations because of a malignant melanoma of the vagina. After a radical colpectomy and lymphadenectomy, vaginal reconstruction with a sigmoid interpolate had been performed. Because of a prolapse of the neovagina, a sacral colpopexy with a polypropylene mesh graft to the S2 and S3 segments had been necessary three years ago.
At clinical admission, the laboratory studies showed only an elevated C-reactive protein concentration (72.26 mg/L). A magnetic resonance imaging (MRI) scan revealed inflammatory processes involving the sacrum, the fifth lumbar vertebral body, the corresponding disk, and the presacral fascia (Fig. 1A). Repeat laparotomy with removal of the neovagina and the surrounding tissue, debridement of the infected tissue, and excision of the intervertebral disk L5/S1 with replacement through a bone graft from the iliac crest was performed (Fig. 1B). In a second surgical session two weeks later, dorsal instrumentation of the segments L5 and S1 followed (Fig. 1C). The microbiologic findings of the intraoperative cultures identified Proteus mirabilis, Morganella morganii, Staphylococcus warneri, and Enterococcus faecalis. Specific antibiotic therapy was administered for three months with ciprofloxacin and rifampicin.
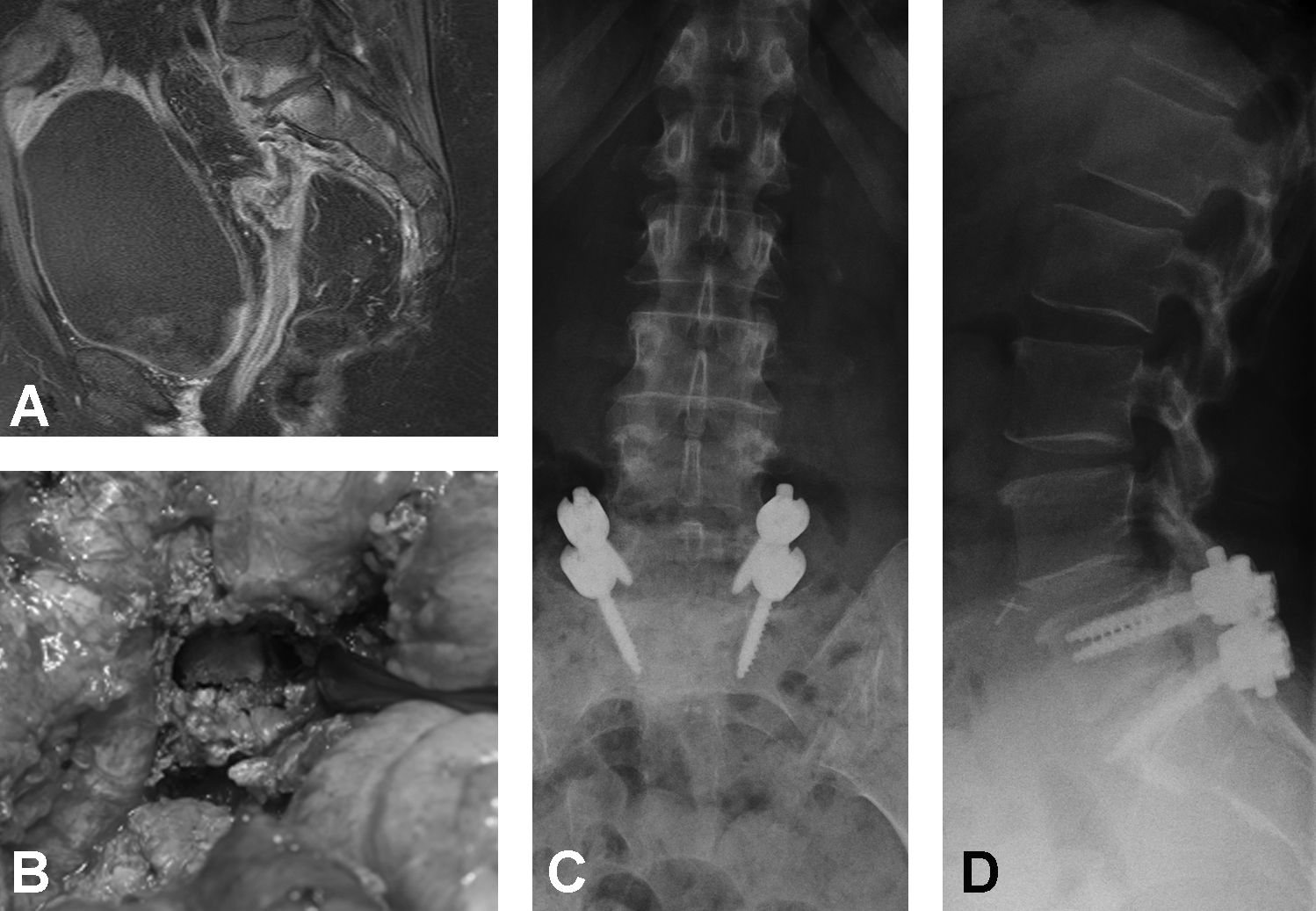
Turbo inversion recovery magnitude sequence of initial pelvic magnetic resonance scan showing inflammatory processes in sacrum, fifth lumbar vertebral body, corresponding disk, and presacral fascia (
In the followup examinations, the patient was in a good clinical condition. No radiologic signs of inflammatory processes were seen, and the laboratory studies showed normal values.
Few cases of lumbosacral spondylodiscitis after gynecologic procedures have been described in the literature [1,2]. Clinical findings range from back pain to neurologic symptoms. The imaging method of choice is MRI. With it, nearly 100% of all florid infections of the spine can be detected [3]. Treatment can be non-operative or operative, and depends on the distinctive symptoms and diagnostic findings. Identifying the responsible pathogen by tissue samples is needed for specific antibiotic therapy [4]. The aim of surgical treatment is debridement of all necrotic tissue, realignment of the spine, stabilization to induce fusion, and prevention of nerve compression or achievement of decompression of the neural structures [5]. In patients with a history of gynecologic surgery who present with persistent back pain and symptoms of an infection, spondylodiscitis should be considered.