
Abstract

To the Editor:
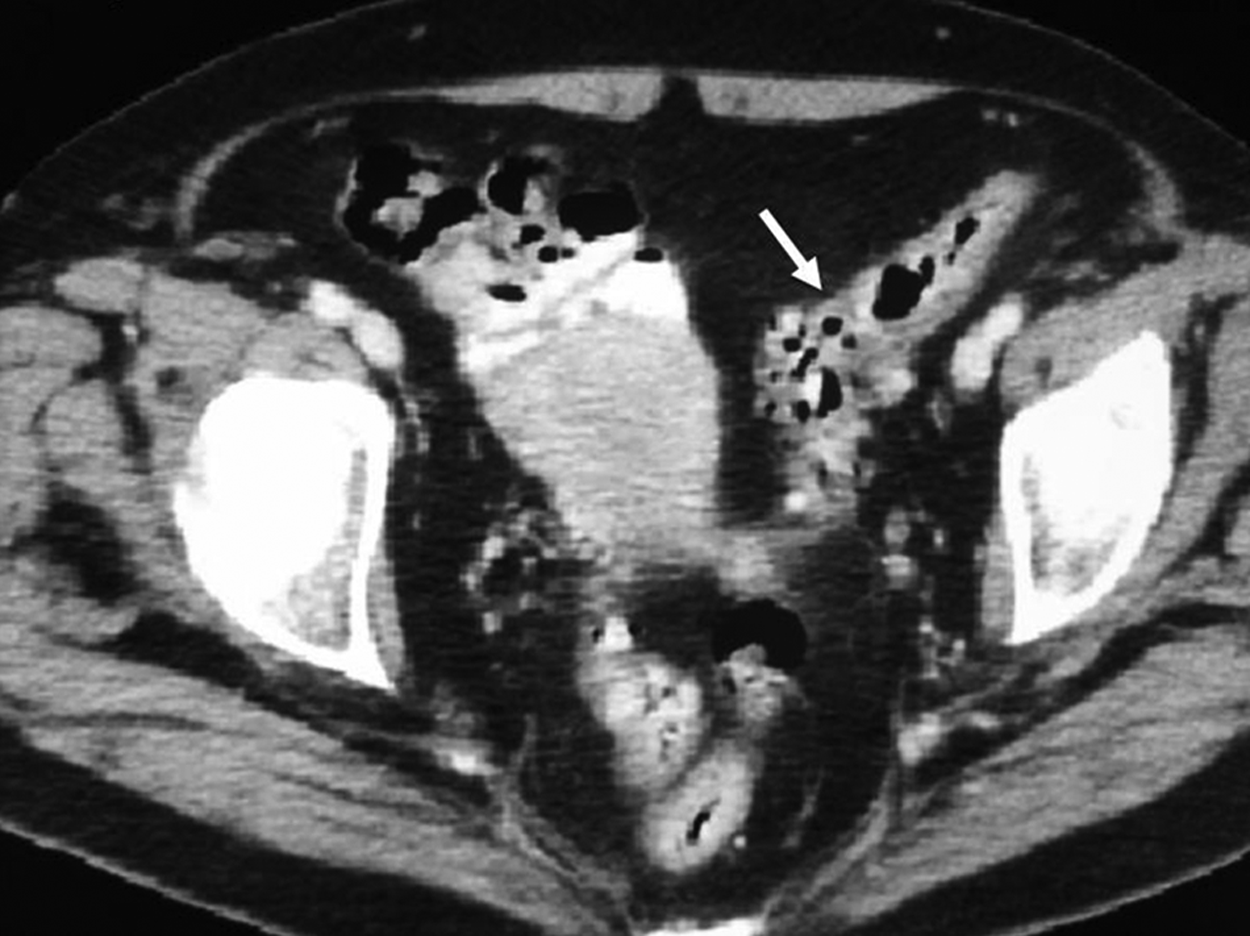
Wall thickening in sigmoid colon with diverticuli and regional adipose tissue involvement.
Three days later, the patient came again to the emergency department complaining of hypogastric pain and fever of 38.5°C. A new CT scan revealed findings similar to those of the previous episode. Tigecycline was started (100 mg loading dose continuing with 50 mg/12 h IV) that was maintained for 14 days, as determined by the Department of Infectious Diseases of our institution in cases of bacteremia. The blood cultures obtained at admission grew Enterococcus faecalis, Bacteroides fragilis, and Escherichia coli resistant to ciprofloxacin and metronidazole and sensitive to tigecycline. The patient was discharged after finishing antibiotic treatment. The patient did not present new episodes of acute diverticulitis in the next 12 months. Elective sigmoidectomy was performed 13 months after the reported episodes without complications. Tobramycin 300 mg and clindamycin 600 mg IV were used for prevention of surgical site infection; the micro-organisms that grew in the previous blood culture were sensitive to these antibiotics.
Micro-organisms involved in acute diverticulitis are mixed flora of aerobic and anaerobic bacteria in 70%–80% of cases. The bacteria isolated most frequently are E. coli, α-hemolytic Streptococcus, β-hemolytic Streptococcus, Streptococcus group D, Klebsiella spp., Bacteroides fragilis, Peptostreptococcus spp., and Clostridium spp. [1].
Tigecycline belongs to the glycylcyclines active against gram-positive, gram-negative, aerobic, and anaerobic multi-resistant micro-organisms, such as methicillin-resistant Staphylococcus aureus (MRSA), Streptococcus spp., Enterobacteriaceae resistant to vancomycin, and Bacteroides fragilis, suggesting it is indicated for the treatment of complex polymicrobial and multi-resistant intra-abdominal infections [2–5]. Its gram-negative activity spectrum and efficacy are similar to those of imipenem-cilastin (except for anti-pseudomonal activity, which tigecycline lachs) making tigecycline a treatment option in patients allergic to beta-lactam antibiotics [3,4]. Tissue penetration is excellent [6].
In the present case, tigecycline was employed, given the failure of the previous antibiotics that could not eradicate the causative agents, leading to recurrent symptoms.