
Abstract
Abstract
Background:
There has not been an appraisal of outcomes of appendectomy for more than 10 years. More reliable diagnostic techniques and minimally invasive surgery are now in widespread use, yet the impact of these advances remains unknown.
Methods:
A retrospective review was performed of 453 patients who underwent appendectomy for appendicitis at a single hospital from 2004 to 2009. Patient demographics, operative characteristics, procedure cost, and pathologic diagnoses were analyzed.
Results:
The overall rate of complicated appendicitis was 13%, with a negative appendectomy rate of 4.9%. The average age was significantly greater for patients with complicated versus uncomplicated appendicitis (47 vs. 33 years, respectively; p<0.001), and by logistic regression, age (as a continuous variable) was a significant factor for complicated appendicitis (p<0.001). The hospital length of stay was 2.3 times longer for patients with complicated appendicitis (4.4 vs. 1.9 days; p<0.001), and the average cost was 86% higher ($14,125 vs. $7,595; p<0.001), the difference in cost being attributable mostly to pharmacy and nursing costs.
Conclusions:
Advances in diagnostic and surgical technique may be altering traditionally accepted rates of complicated appendicitis and negative appendectomy. For the first time, age is shown to be related to the rate of complicated appendicitis as a continuous variable rather than simply an extreme. Patients with complicated appendicitis still stay in the hospital longer, and there is a large cost difference as a result.
Most series report rates of complicated appendicitis between 20% and 30%, and despite advances in medical and surgical care, complicated appendicitis still results in higher rates of morbidity and death [2,9–12]. Because of the impact complicated appendicitis can have on patient outcome, numerous studies have attempted to determine patient-specific factors that predict perforation. One of the more commonly reported, but poorly characterized, risk factors for perforated appendicitis is extremes of age [3,11,13–17]. An explanation for this finding has been a disadvantage of communication or limitations in access to healthcare, resulting in later presentation and subsequent disease progression.
The last major study undertaken to characterize patients with complicated appendicitis was from patients treated in 1993, before the widespread adoption of CT scans and laparoscopy [11]. The current study aimed to characterize differences in patients who have complicated versus uncomplicated appendicitis in terms of basic characteristics, operating room utilization, and overall cost.
Patients and Methods
Study population
The study was approved by the University of Pittsburgh Institutional Review Board. The study population was derived from the operating room database at a single teaching hospital from June 2004 to June 2009. Inclusion criteria consisted of all patients with a Diagnosis-Related Group (DRG) descriptor of appendectomy or laparoscopic appendectomy. Of the 459 cases found, six were excluded because of findings that eliminated appendicitis as the primary reason for the operation (e.g., trauma laparotomy).
Data
Cases derived from the operating room database were matched with hospital data from compatible databases, and chart review was performed to obtain the final pathologic diagnosis. The time points gathered for each patient were the case start date and time (skin incision), case end date and time (drapes down), and discharge date and time. Durations between these points were derived from the data and included case length (start time to end time) and length of stay (LOS; start time to discharge time). Other data collected were age, gender, American Society of Anesthesiologists (ASA) class, intra-operative blood product transfusion, open or laparoscopic surgery, total cost, specific cost breakdown, and pathologic diagnosis (normal appendix, appendicitis, gangrenous or perforated appendicitis).
Patients were classified as having complicated appendicitis if the final pathologic diagnosis included the terms “gangrenous,” “perforated,” or “abscess.” This definition was chosen as the historically accepted definition and made comparisons with prior studies more relevant. In three cases where the final pathologic diagnosis was not clear regarding perforation, the operative note was reviewed for confirmation of the diagnosis. All other cases were considered to be uncomplicated appendicitis, which included those where pathologically normal appendices were found.
Statistical analyses
One-way ANOVA and chi-square analyses were performed to compare complicated and uncomplicated cases for continuous variables and proportions, respectively. The p values for each analysis were considered significant at 0.05.
Histograms, means plot with 95% confidence intervals (Tukey method), and quantile plots were created as indicated. Goodness-of-fit to the uniform distribution for quantile plots was evaluated with the Kolmogorov-Smirnov test and was considered significant at p<0.05. Logistic regression was performed for complicated appendicitis as a function of age (as a continuous variable), ASA class, and gender. Odds ratios were calculated by segregating patients by age (per decade) and comparing that with the rest of the sample population. Sample averages are reported ±standard deviation. All statistical analyses were performed with Statgraphics Centurion XVI (Warrenton, VA).
Results
Patient characteristics and complicated appendicitis
Of the 453 patients, 13% (59) were classified as having complicated appendicitis. There were no in-hospital deaths. Only 4.9% of the patients (22) had pathology findings consistent with a normal appendix and no other abnormality. Forty-three percent of the patients (194) were female, and there was no significant difference in the proportion of female patients in the complicated appendicitis group (45.8% vs. 42.4%; p=0.625) (Table 1). Logistic regression found gender to be unrelated to complicated appendicitis (p=0.926). The average ASA class was slightly higher in patients with complicated appendicitis (2.1±0.8 vs. 1.7±0.7; p<0.001), but logistic regression found ASA class to be unrelated to complicated appendicitis (p=0.390) (Table 1).
ASA=American Society of Anesthesiologists; NS=not significant.
The average age for all patients was 34.9±16.4 years (range 13–92 years). The average age for complicated appendicitis was significantly higher (47.4±18.3 vs. 33.0±15.3 years; p<0.001) (Table 1). Age distributions of the entire study population and the patients with uncomplicated appendicitis revealed a skew toward younger ages, whereas the distribution for complicated appendicitis was more even (Fig. 1). Quantile plots revealed a uniform distribution of complicated appendicitis by age, which was not observed in the overall population or the uncomplicated cases (confirmed with a Kolmogorov-Smirnov test for goodness-of-fit) (Fig. 1). Logistic regression revealed a significant relation between age (as a continuous variable) and complicated appendicitis (complicated=expη/(1+expη), where η=− 3.75648+0.0468278*AGE; p<0.001) (Fig. 2). Furthermore, when the patients were segregated by age in decades, the odds ratio for complicated appendicitis displayed an increasing trend from the second through the seventh decade (Fig. 3).

Histograms and quantile plots of age for (

Logistic regression for age and complicated appendicitis (complicated=expη/(1+expη), where η=−3.75648+0.0468278*AGE; p<0.001).
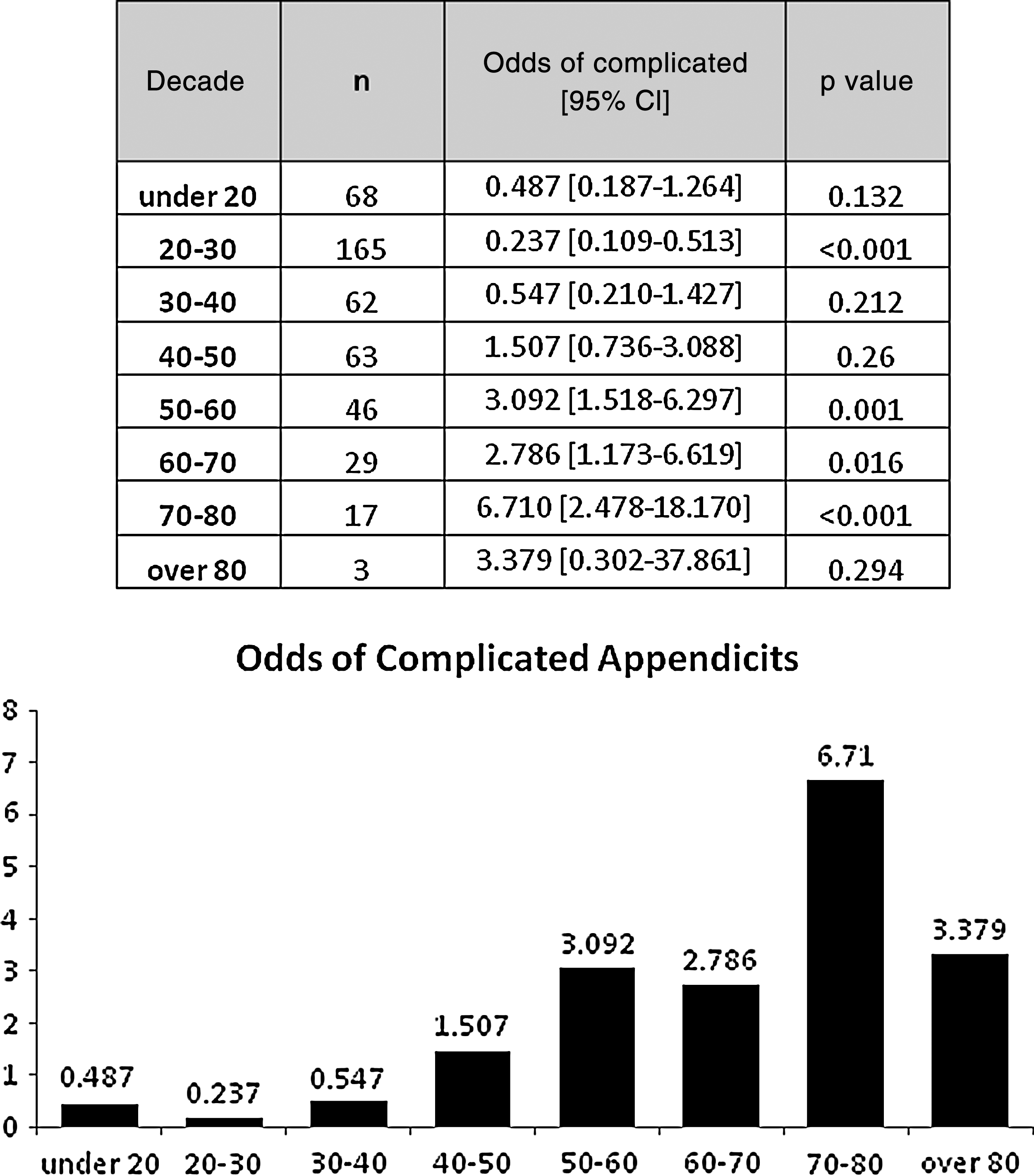
Odds ratios for complicated appendicitis by decade.
Operative characteristics and complicated appendicitis
For all 453 cases, the average procedure length was 69.3±25.6 min (range 20–212 min). The average case duration for the complicated versus uncomplicated appendicitis cases was not significantly different (73.9±25.8 min vs. 68.6±25.5 min; p=0.138) (Table 1). Transfusion of blood products was required in three cases (0.7%), and there was no difference between complicated and uncomplicated appendicitis (1.7% vs. 0.5%, respectively; p=0.294) (Table 1). However, whereas 24.5% of all cases were done in an open fashion, a significantly higher percentage of complicated than uncomplicated appendicitis cases were open operations (40.7% vs. 22.1%, respectively; p=0.002) (Table 1).
Costs
The average hospital LOS for all patients was 2.2±2.3 days (range 0.42–17.89 days), and the average hospital LOS was 2.3 times longer for patients with complicated appendicitis (4.4±3.2 vs. 1.9±2.0 days; p<0.001) (Fig. 4). Additionally, although the average total cost for all patients with appendicitis was $8,445±$12,347 (range $2,150–$222,709), the total cost associated with complicated appendicitis was on average 86% higher than with uncomplicated appendicitis ($14,125±$28,568 vs. $7,595±$7,022; p<0.001) (Fig. 5). When cost was analyzed further by specific allocation within the hospital, it was found that the greatest contributors to this cost disparity in absolute dollars were pharmacy costs ($5,046±$25,979 vs. $996±$5,624; p=0.007) and nursing costs ($2,822±$3,089 vs. $1,127±$1,568; p<0.001) (Fig. 5). The surgical costs associated with complicated vs. uncomplicated appendicitis were not significantly different ($3,829±$1,443 vs. $4,081±$1,621, respectively; p=0.2596) (Fig. 5).
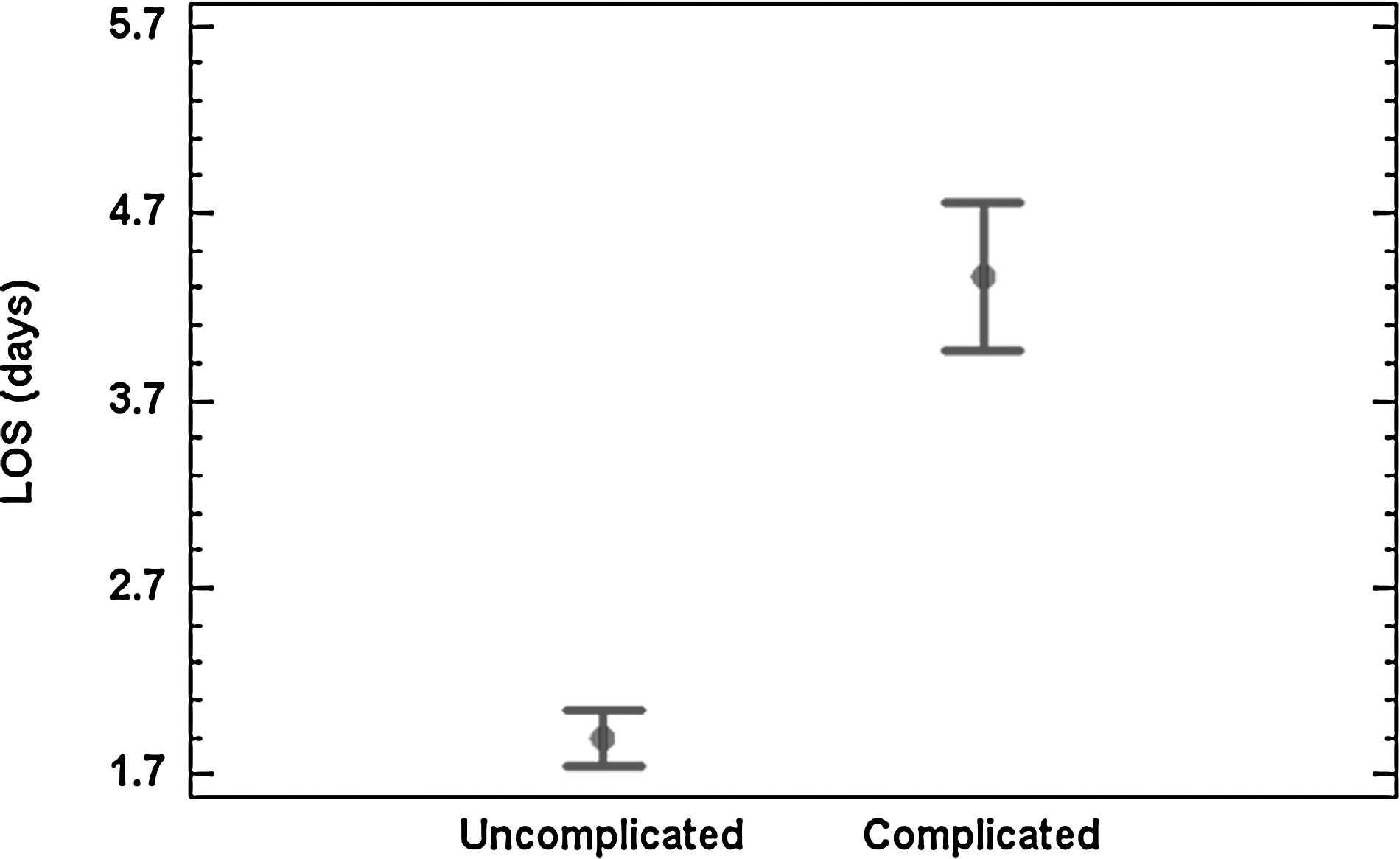
Means plot for hospital length of stay (LOS) for uncomplicated and complicated appendicitis. Bars represent 95% confidence intervals.

Costs associated with uncomplicated and complicated appendicitis. * indicates costs for which there is a statistically significant difference.
Discussion
Because complicated appendicitis is associated with greater morbidity, for more than 100 years the surgical literature has attempted to describe factors linked to this condition [1–3, 9–11,13,16]. Advances in pharmacologic therapies and medical technology in the 20th century greatly improved the outcomes of appendicitis, and in the last decade, the widespread utilization of CT scans and laparoscopy have reduced the morbidity associated with this disease [4–8]. However, there has not been a contemporary appraisal of patients who undergo appendectomy.
This study describes characteristics associated with surgically managed complicated appendicitis. The key findings are: (1) The risk of complicated appendicitis is a function of age, not just extremes of age; (2) on average, patients with complicated appendicitis stay in the hospital more than twice as long as patients with uncomplicated appendicitis; (3) on average, patients with complicated appendicitis cost the healthcare system 86% more than patients with uncomplicated appendicitis, which is attributable mainly to higher pharmacy and nursing costs; and (4) the rate of negative appendectomy is only 4.9%.
Many studies have evaluated age as a risk factor for perforated appendicitis and have concluded that there is a greater risk of perforation in the elderly population [3, 11, 13–17]. In the current study, in a logistic regression analysis, complicated appendicitis in adults was related to age as a continuous variable, and “extremes of age” alone was not a sufficient descriptor of the relation between age and complicated appendicitis. That is to say, in our population, a 35-year-old carried a greater risk of complicated appendicitis than a 30-year-old, but not as much as a 40-year-old. Therefore, the risk of complicated appendicitis should not be considered higher with an arbitrary age cutoff but rather as a continuous function of age.
Interestingly, even though this study did not include a pediatric population, we found that the relative risk of perforation was higher for those under the age of 20 than in 20- to 30-year-olds and even 30- to 40-year-olds. This may represent the younger population that traditionally has been found to have higher rates of complicated appendicitis. This raises a question about previous explanations for this phenomenon that suggested patients at the “extremes of age” have a higher risk of perforation because of the inability to communicate symptoms, instead of a true physiological reason that predisposes humans to appendicitis at different ages. It also should be noted that the odds ratio for complicated appendicitis is low in the older-than-80-years category. This finding is somewhat difficult to interpret, however, as there were only three patients in this category.
In this study, the average hospital LOS was 4.4 and 1.9 days for complicated and uncomplicated appendicitis, respectively. This is much shorter than reported in previous studies of complicated and uncomplicated appendicitis: The last such review of patients from 1993 had an average LOS of 7.2 and 3.4 days, respectively [11]. This change is partly a reflection of the utilization of laparoscopy for both complicated and uncomplicated cases, which reduces hospitalization and shortens recovery time [6–8,18]. It is not surprising that patients with complicated appendicitis stay longer than those with uncomplicated disease, but it is interesting that they still stay more than twice as long, which is similar to the findings of older studies [2,11].
A finding from this study that differs from what traditionally has been reported in the literature is our rate of complicated appendicitis of 13%, whereas most studies report between 20% and 30% [2,9–12]. The age distribution of our patient population mimics closely what has been described previously, and although it was not specifically studied, our patient demographics are those of a large teaching institution. The factor most closely associated with rates of complicated appendicitis has been time to treatment, usually determined by the patient and not the hospital [19–21]. Perhaps better diagnostic techniques have led to a number of patients undergoing non-operative intervention (percutaneous drainage and antibiotics), who are not accounted for in this study. Alternatively, there may be a difference in the population seen at this institution in terms of accessibility to healthcare, resulting in earlier presentation after the onset of symptoms. Also possible is that there are institutional factors that relate to rates of complicated appendicitis that have not been accounted for in other reports. Although this study was not designed to answer these questions, it would be interesting to examine this phenomenon further. Nonetheless, this finding points to a reduction in the number of patients with complicated appendicitis who undergo an operation.
Another finding is the rate of negative appendectomy, which was only 4.9%. Again, this could be attributed partly to a difference in the population at this institution not accounted for by this study, or perhaps the utilization of CT scans has reduced the rate of negative appendectomy significantly from the traditionally accepted 10% to 20%. Again, although this study was not designed to answer this question, it would be interesting to see how many patients had suspected appendicitis ruled out by CT scan.
Finally, the current study shows for the first time that on average, complicated appendicitis costs the hospital 86% more than uncomplicated appendicitis. These differences are distributed through many cost centers of the hospital, but the largest impact comes from pharmacy and nursing. Interestingly, there was a large discrepancy between the percent of complicated versus uncomplicated appendicitis cases done by open surgery (41% vs. 22%, respectively), which usually is associated with a lower cost. However, our analyses show no significant difference in the average surgical costs of complicated and uncomplicated appendicitis cases. Because most prior studies have not found hospital factors to be associated with complicated appendicitis, but rather that it is the natural course of the disease and the propensity of the patient to seek care timely, perhaps the higher cost associated with complicated appendicitis can be mitigated only by better access to early evaluation for symptoms of the disease [19–21].
There are limitations to this retrospective study that do not allow it to address the disease process of appendicitis as a whole, but only the patients who undergo operation for appendicitis. Thus, we could not account for patients who were managed non-operatively because of frank abscess or patient directives that limited surgical intervention. Although including these patients might enhance the interpretability of the current data, because non-operative management of appendicitis is a relatively recent option, this study can be compared with most previous studies. The data still reflect how the operative management of appendicitis is evolving.
In conclusion, we found that (1) The risk of complicated appendicitis is a function of age (not simply extremes of age); (2) the hospital LOS is shorter than historical norms, yet complicated appendicitis still predisposes the patient to a significantly longer hospital stay; and (3) complicated appendicitis is more costly for the healthcare system. We also found that there may be changes associated with the overall rates of complicated appendicitis and negative appendectomy that could be related to the adoption of CT scanning for diagnosis or earlier presentation after the onset of symptoms. As the treatment and outcomes of appendicitis evolve with the utilization of new technology, it is important to understand how better patient and system outcomes can be attained through the intervention of surgeons and greater access to early evaluation and treatment.
Footnotes
Author Disclosure Statement
None of the authors has competing financial interests to disclose.