
Abstract

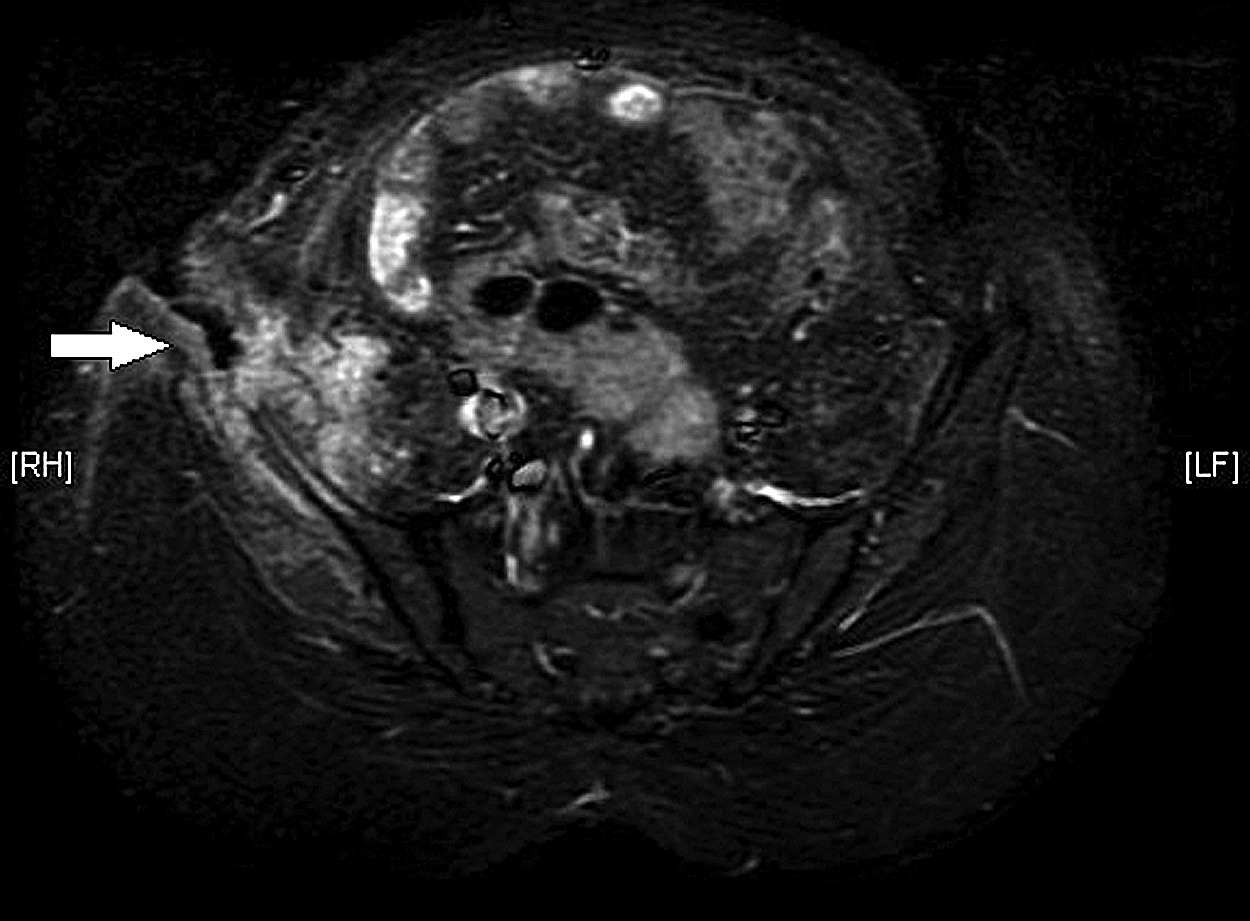
Magnetic resonance imaging (MRI) of pelvis showing sinus tract (arrow) with extensive involvement of underlying soft tissue and ilium.
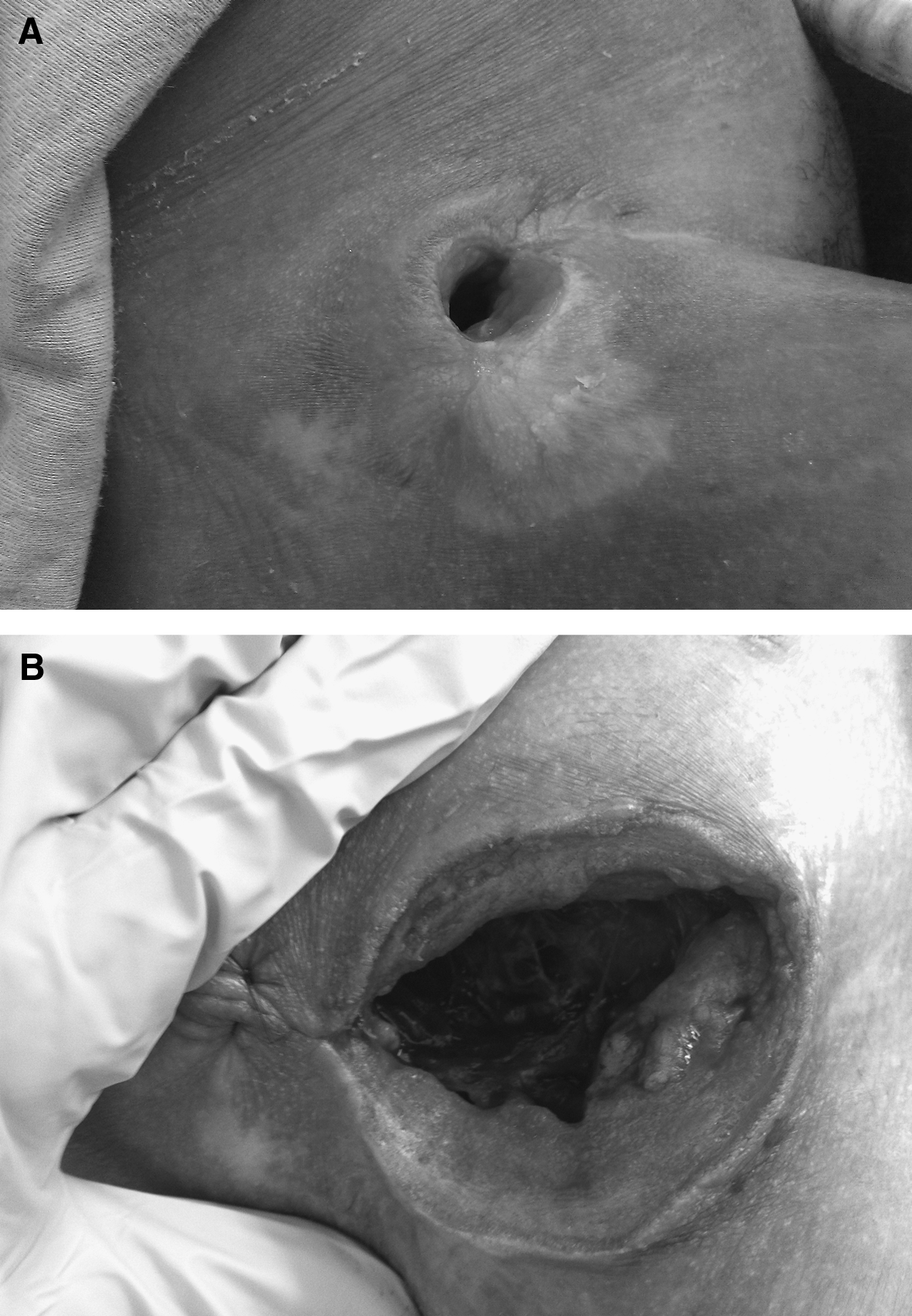
Views of ulcer. (
Osteomyelitis of the pelvis can result from direct trauma, post-operative infection, decubitus ulcers, or hematogenous dissemination [1,2]. Diagnosis is based on clinical suspicion coupled with imaging. Most infections are polymicrobial, and the most frequent pathogens are Staphylococcus spp., Pseudomonas aeruginosa, and B. fragilis [2]. Management includes debridement, antibiotics tailored to the inciting pathogens, and wound care. If prolonged intravenous antibiotic therapy is unsuccessful, surgical intervention is warranted. This can be as minimal as soft tissue debridement with or without local bone debridement or as extensive as hemipelvectomy or even hemicorporectomy. A standard hemipelvectomy includes a lower-extremity amputation, whereas an internal hemipelvectomy allows anatomic limb salvage, albeit without function. The incision can either be left open or managed with flap closure. In a series of eight patients undergoing hemipelvectomies for severe decubitus ulcers, the 30-day mortality rate was 25%; however, quality of life was improved for the survivors [3]. Rarely, hemicorporectomy can be used to treat terminal pelvic osteomyelitis. Although hemicorporectomy is extremely morbid, there are reports of patients surviving more than 20 years after surgery [4].