
Abstract

To the Editor:
A 68-year-old patient arrived at our emergency department in poor general condition, having had abdominal pain for three days and a diminished level of consciousness. She had severe sepsis with tachycardia, tachypnea, high temperature, and arterial hypotension. Physical examination showed a large, painful, indurated mass on the lower abdomen. Laboratory studies revealed a C-reactive protein concentration of 38 mg/dL and neutrophilia. An abdominal computed tomography scan depicted an abscess on the subcutaneous lower abdominal wall, which appeared not to be in contact with the abdominal cavity (Fig. 1).
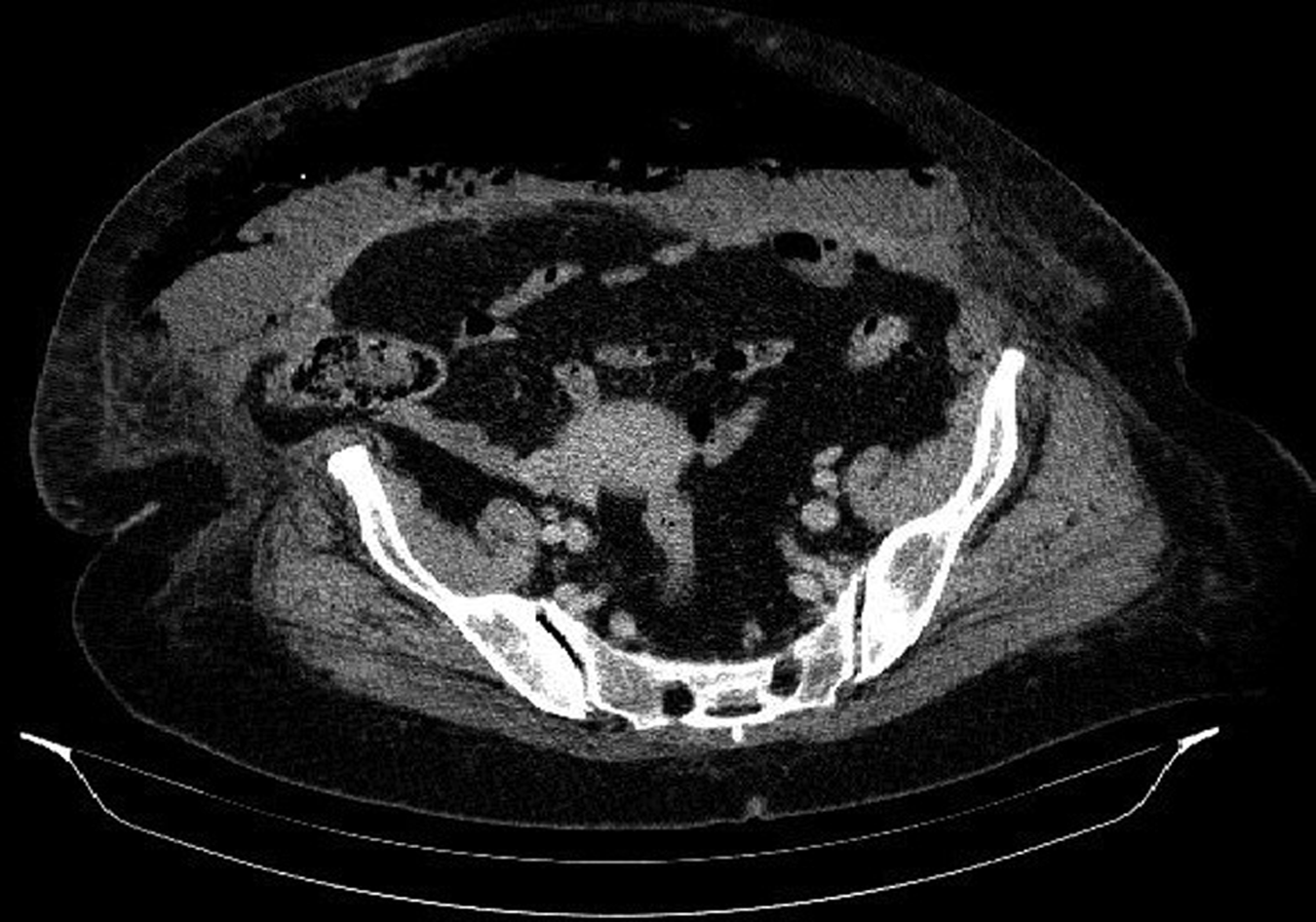
Abdominal computed tomography scan shows subcutanteous abscess on lower abdominal wall.
Urgent surgical intervention was carried out on the abscess, which contained a large quantity of pus and was incised and drained. Empiric antibiotic therapy was started with ertapenem 1 g given intravenously every 24 h. The results of the culture were obtained after nine days and were positive for Clostridium perfringens sensitive to ertapenem and resistant to clindamycin. The patient had a good clinical response.
Infection of soft tissue associated with C. perfringens usually appears in patients with recent wounds or injuries in the infected area. The antimicrobial treatment of infections caused by Clostridium species is penicillin G with or without clindamycin [1–3]. In our case, the patient had not undergone surgery recently and did not present any skin injury that might have caused the abscess. The cultures obtained during the operation yielded C. perfringens resistant to clindamycin.
The literature contains numerous cases of soft tissue infection by C. perfringens, but we found only one case of infection by a strain resistant to clindamycin. Resistance to antibiotics in anaerobic bacteria has increased in recent times, and this, together with allergy to penicillin, causes substantial problems in choosing the most suitable antibiotic to treat these infections. In these cases, the antimicrobial agent of choice is clindamycin, but the appearance of resistance to this drug in Clostridium species, above all C. perfringens, can cause a serious problem when treating soft tissue infections [2].
This is a rare case of a severe infection of soft tissue by C. perfringens that had no known entry point and was resistant to clindamycin. Our conclusion is that a sample should always be taken for culture in order to identify the microorganism that has caused the infection. This in turn allows physicians to adjust the treatment correctly and prevent resistance from developing.
Footnotes
Acknowledgment
We are grateful to the Language Service of the Rovira i Virgili University for translating the original text.