
Abstract
Abstract
Background:
Tuberculosis (TB) is a serious infection afflicting a multitude of people worldwide. Recently, its prevalence has increased. The incidence of skin involvement generally is low. Bacillus Calmette-Guérin (BCG) is a live attenuated strain of Mycobacterium bovis that typically is administered as a vaccine to stimulate the immune system when treating some early neoplasms or to guard against tuberculosis.
Methods:
Case report and literature review.
Case Report:
The authors describe a young man with osteosarcoma of the left hemipelvis who received intradermal BCG injection for immune stimulation prior to surgery. In the course of neoadjuvant chemotherapy, he developed cutaneous tuberculosis.
Conclusion:
It is our opinion that BCG injection should be avoided in all patients requiring surgery, especially in oncologic patients, where the immunodeficiency brought on by chemotherapy predisposes to active opportunistic infection.
Bacillus Calmette-Guérin (BCG) is a live attenuated strain of Mycobacterium bovis that typically is administered as a vaccine to stimulate the immune system when treating some early neoplasms or to guard against tuberculosis [4]. Occasionally, such vaccination results in CTB [5,6].
The authors herein describe a young man with osteosarcoma of the left hemipelvis who received intradermal BCG injection for immune stimulation prior surgery. In the course of neoadjuvant chemotherapy, he developed CTB.
Case Report
A 14-year-old Caucasian male was referred to our Department of Oncological Orthopaedics for evaluation of a tumor in the left hemipelvis. Symptoms had begun five months earlier, and radiographs obtained the following month showed a primitive bone tumor. By magnetic resonance and computed tomography (CT) scans, the lesion appeared to involve the iliac wing broadly to the sacroiliac joint, the roof of the acetabulum, and the entire range of gluteus muscles. Imaging was highly suggestive of osteosarcoma, so a needle biopsy was performed. Histopathology examination confirmed high-grade osteosarcoma; a total body CT scan was negative for distant metastasis.
In another hospital, an attempt to stimulate the patient's immunity with intradermal BCG injection proved ineffective, so he was referred to an oncologist. This physician was unaware of the prior BCG use. Neoadjuvant chemotherapy with high-dose methotrexate (12.0 g/kg), cisplatin, and doxorubicin was initiated per the Italian Sarcoma Group (ISG) OS1 protocol and was followed by the development of multiple ulcerated skin lesions. No antibiotic was administered. Therapy was continued by the oncologist despite the exacerbations of the skin condition with each course of chemotherapy, and the patient underwent surgery at our center.
Clinical inspection of the eruption disclosed ulcerated plaques in aggregates, involving the left deltoid area and the left inguinal fossa. The lesions generally were uniform, with an average diameter of 0.8 cm, and were red/pink with atrophic centers. Their borders were raised but ill-defined (Fig. 1). On biopsy, a granulomatous reaction compatible with tuberculous disease was observed (Fig. 2).

Clinical view of skin lesions. (
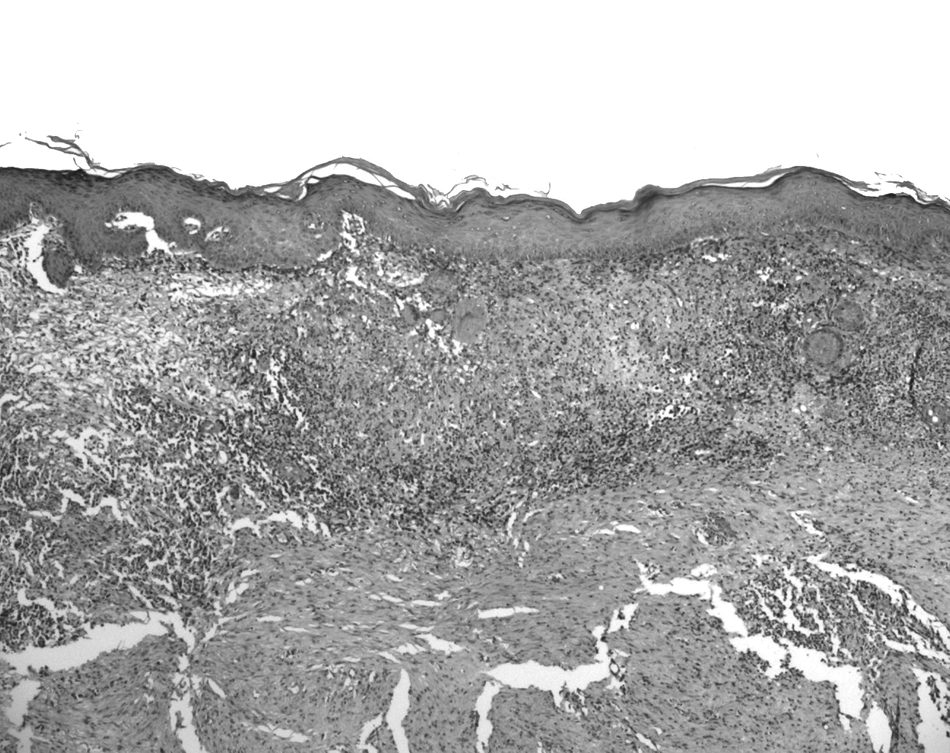
Cutaneous biopsy showed poorly formed non-caseating granulomas with multinucleated giant cells in the upper dermis just below the epidermis. Ziehl-Neelsen stain revealed no bacilli. In deep dermis, cicatricial fibrosis was present. (Original magnification×10.)
Four weeks after cessation of chemotherapy, the patient was hospitalized for surgery. Treatment with rifampicin, ethambutol, and isoniazid was started after a presumptive diagnosis of CTB and given as prophylaxis at the start of anesthesia. The patient then underwent hemipelvic resection with provisional cement and screw reconstruction to reduce the risk of introducing infection. Definitive reconstruction was deferred to be done at one-year follow-up, provided the preliminary surgical results were not compromised by TB. Post-operative chemotherapy was still feasible, and no metastases were evident. A left inguinal lymph node sampled during surgery was positive for tuberculous lymphadenitis, showing the beginnings of scrofuloderma on histologic examination.
Discussion
Cutaneous TB is caused by Mycobacterium tuberculosis and Mycobacterium bovis and presents most commonly as scrofuloderma, with tuberculous lymphadenitis and cutaneous ulcerations as the main epiphenomena [1,6]. The BCG product is a live attenuated strain of M. bovis used to provide protective immunity against tuberculosis, but infectious complications do occur, at a rate of 0.4 per 1,000 vaccinations [6,7].
Because of its ability to activate the immune system, the first attempt to use BCG as an immunostimulator in cancer patients was described in 1975 [8]. Currently, intravesical BCG typically is instilled for in situ and superficial carcinoma of the urinary bladder, for residual bladder cancer after surgical resection, and as prophylaxis for multicentric or potentially recurrent bladder cancer [4]. Immunotherapy with BCG also has been described as a treatment for malignant melanoma [9]. Although several trials are ongoing to verify the value of BCG in other advanced tumors [10–12], its utility in osteogenic sarcoma is questionable. The few reports available in this setting are old and inconclusive, and no extended follow-up data (per recommendations) have been published [13–16].
It is our opinion that BCG injection should be avoided in all patients requiring surgery, especially in oncologic patients, in whom the immunodeficiency brought on by chemotherapy predisposes to active opportunistic infection. The surgical manipulations can easily introduce organisms into deeper tissue layers. In the event that BCG is used in an immunocompromised host, anti-tuberculous prophylaxis is indicated, given that this is a live (albeit attenuated) bacterial strain [17].
For our patient, surgery was performed prior to disappearance of cutaneous lesions as a matter of urgency, mandating meticulous surgical dissection to avoid tuberculous contamination. A phased (two-step) surgical reconstruction also was necessary in view of the infectious risk. More experimental study clearly is needed to gauge the efficacy of BCG in bone neoplasms. Although BCG injection has benefit for small or superficial tumors, we feel it should be avoided when major surgery is anticipated or indicated as first-line treatment.
Footnotes
Funding Sources and Author Disclosure Statement
No external funds were used for this work. The authors declare that they have no conflicts of interest related to this manuscript.