
Abstract

Case Report
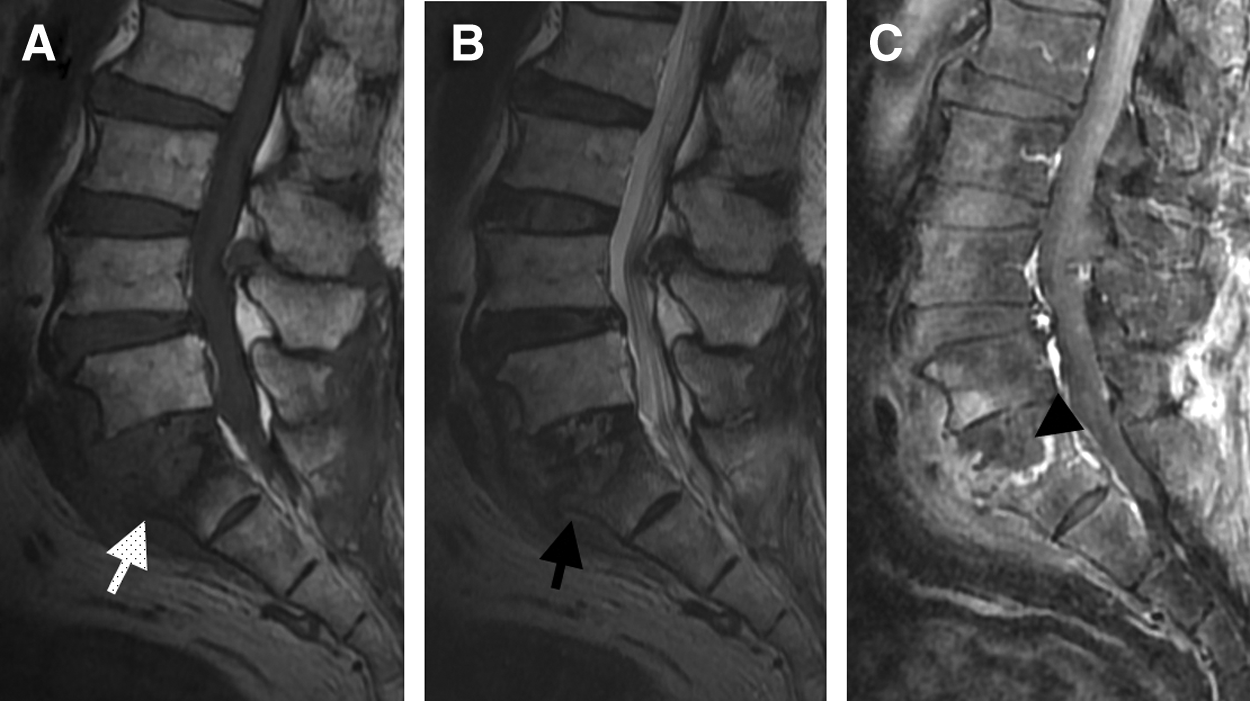
A 72-year-old male presented with a three-month history of back pain as well as radiating pain and weakness of both lower extremities. He complained of focal pain, but no motor dysfunction was noted on physical examination. The preoperative laboratory data were as follows: White blood cell (WBC) count 9,800/mm3 (normal range 4,000–9,000 cells/mm3); C-reactive protein concentration 129.2 mg/dL (<5 mg/dL); and erythrocyte sedimentation rate 76 mm/h (0–20 mm/h). Computed tomography (CT) of the spine showed sclerotic changes over the upper portion of the sacrum and destruction of the anterior endplate (Fig. 1). Magnetic resonance imaging (MRI) found hypointense regions on T1-weighted images and hyperintense regions of the sacrum, indicating bone marrow edema on T2-weighted images. Post-gadolinium T1-weighted imaging revealed enhancement of the pre-spinal soft tissue and the sacral vertebral body (Fig. 2). The patient denied any history of pulmonary tuberculosis, and the chest radiograph conducted on admission showed no abnormal findings.
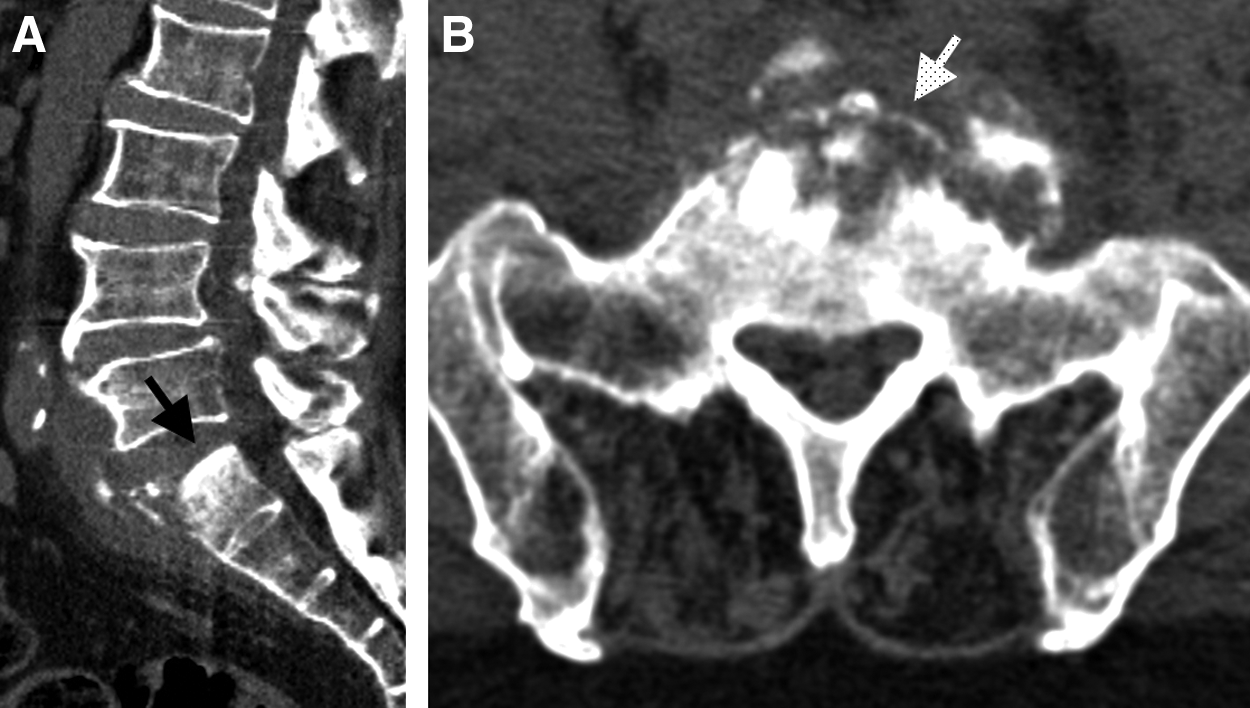
Computed tomography image in sagittal view (

Magnetic resonance images. (
A navigator-guided open biopsy of the affected rostro-ventral portion of the S1 vertebral body was conducted through a transpedicular approach. Histologic examination of the biopsy specimen revealed necrosis and granulation, but no granuloma (Fig. 3). The results of mycobacterial culture and acid-fast staining of the specimen were negative.
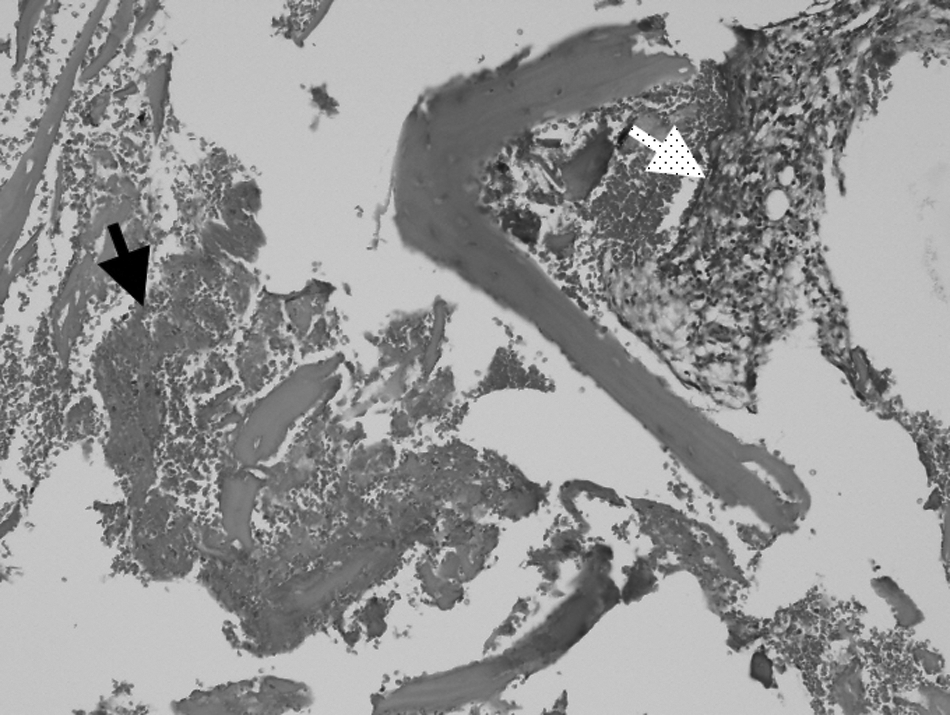
Histologic appearance of biopsy specimen showing necrosis (black arrow) and granulation (white arrow), but no granuloma. (Hematoxylin–eosin staining; original magnification×100).
As spinal tuberculosis is found sporadically in Taiwan, the specimen was examined further with PCR. This testing was conducted as follows. The surgical sample was ground and centrifuged at 300×g for 5 min. The supernatant liquid was discarded, and the cell pellet was resuspended in phosphate-buffered saline. The DNA was extracted using a QIAamp DNA minikit (Qiagen, Germantown, MD) following the manufacturer's protocol. The sequences of the primers used for amplification were 5′-CCTGCGAGCGTAGGCGTCGG-3′ and 5′-CTCGTCCAGCGCCGCTTCGG-3′. Nucleotides, primers, buffer, and enzymes were mixed and then dispensed in aliquots. Extracted DNA was added, and the reaction mixture was overlaid with mineral oil. A control tube containing no DNA was included with each set of reactions. The samples were denatured at 94°C for 5 min, and then 25 amplification cycles were performed with denaturation at 94°C for 2 min, annealing at 68°C for 2 min, and primer extension at 72°C for 2 min. The extension time was increased by 5 sec with each subsequent cycle [8,9]. The product was analyzed by electrophoresis on agarose gels. The presence of 123 base pair (bp) fragments was indicative of infection with Mycobacterium tuberculosis, and the 245-bp products represented β catenin as the internal control (Fig. 4). The results of the PCR test confirmed M. tuberculosis infection. On the basis of the PCR test report, the patient was started on a 6-mo antituberculosis regimen comprising rifampicin, ethambutol, and isoniazid.
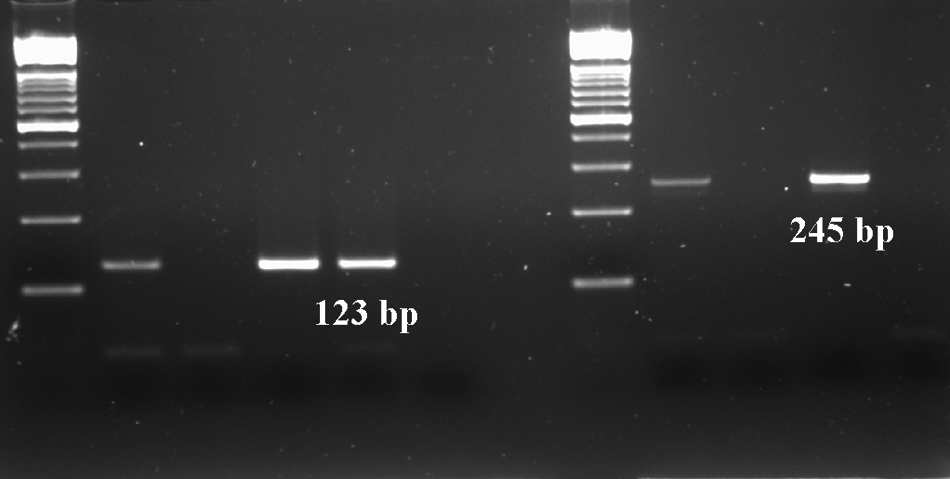
Electrophoresis identifying product of 123 base pairs indicative of infection with Mycobacterium tuberculosis and product of 245 bp as an internal control.
Six months later, the follow-up MRI scan of the spine revealed increased intensity over the upper portion of the sacrum on T1-weighted imaging and decreased intensity in the sacral vertebral body secondary to resolution of bone marrow edema on T2-weighted imaging. Post-contrast MRI scans demonstrated less enhancement at the previously infected area, which represented regression of the tuberculosis infection in the L5–S1 region (Fig. 5). The follow-up laboratory data also showed resolution of inflammation: WBC count 6,400 cells/mm3; C-reactive protein 5.8 mg/dL; and erythrocyte sedimentation rate 15 mm/h. At the end of treatment, the patient was symptom free with no functional impairment.
Magnetic resonance imaging scans. (
Discussion
The presence of granulomas in infected tissue is considered a hallmark of mycobacterial disease [10]. In a series of 15 patients with extrapulmonary tuberculosis, histologic examination of the tissue biopsy specimens from 14 patients revealed granulomatous inflammation [11]. However, histologic examination is an indirect method and is not always reliable for accurate diagnosis [6,12]. The PCR method, with its ability to amplify DNA fragments of interest selectively, is a powerful, accurate, rapid, and sensitive method for the detection of mycobacterial infections [13,14]. The samples from partially treated patients may give negative results in mycobacterial culture, but the infection still can be detected by PCR [13]. Therefore, PCR has played a major role in the study of the fastidious, tough-walled, and slow-growing mycobacteria [15]. In a recent study, the authors report that PCR is a rapid and effective method of diagnosing extrapulmonary tuberculosis, and its sensitivity is higher in spinal than in non-spinal samples [16]. Those investigators concluded that antituberculous treatment can be started if the PCR test is positive, as the false-positive rate is very low. In the current case, the histologic examination of the samples did not reveal any granulomatous inflammation. Early antituberculous therapy based on a positive PCR test for tuberculosis infection results in improvement in the clinical manifestations, imaging findings, and laboratory data. As a result, we highly recommend PCR as the first step in the diagnosis of bone and joint tuberculosis. This case report highlights the importance of creating awareness regarding tuberculous spondylitis and the significance of PCR testing in establishing a definite diagnosis of infection by M. tuberculosis.
Footnotes
Author Disclosure Statement
The authors report no conflicts of interest.