
Abstract

An 80-year-old man presented to our department with sepsis (hypotension, hypoxia, metabolic disorder, acidosis, leukocytosis, acute kidney injury, and congestive heart disease). No recent history of recurrent UTI was reported, although his history was suggestive of a single episode of left kidney stones at the age of 40, which resolved spontaneously. Severe prostate hyperplasia was present. The patient complained of lower abdominal pain, purulent urethral discharge, and hypogastric cutaneous ulceration with spontaneous serous–purulent discharge. Physical examination revealed hypogastric tenderness with diffuse subcutaneous emphysema. A hard hypogastric mass was palpable, causing acute pain and urethral passage of purulent material. A computed tomography (CT) scan showed multiple GBC, free air in the bladder, and a vesicocutaneous fistula with multiple abdominal wall abscesses (Fig. 1).
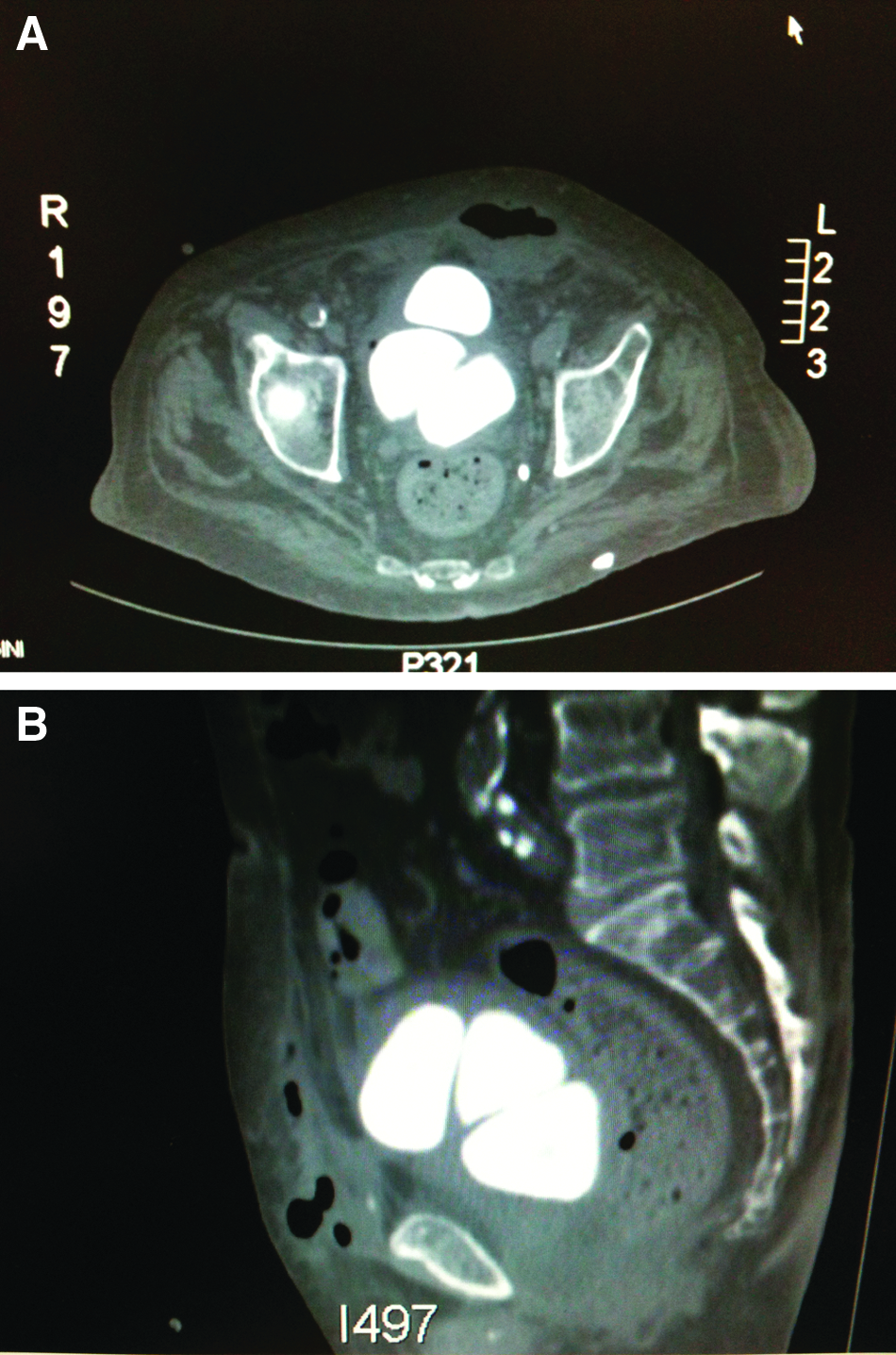
Computed tomography scans showing multiple giant vesical stones causing a spontaneous vesicocutaneous fistula, confirmed by the presence of air and liquid in the abdominal wall and soft tissues (
Antibiotic therapy (ciprofloxacin 400 mg bid) was given, and a cystolithotomy was performed with drainage of multiple abdominal-wall abscesses. Surgery allowed the removal of three giant stones with a maximum dimension of 11×8×7 cm and a total weight of 1,580 g. A double-lumen catheter was left in the bladder through the suprapubic incision to perform continuous transcurrent bladder lavage during the post-operative course, favoring the resolution of local infection and avoiding the development of blood clots in the vesical lumen. The abscesses were drained with closed suction drains.
The post-operative period was uneventful. The sepsis abated rapidly with no residual purulent discharge after post-operative day 2. An intra-operative vesical swab yielded Escherichia coli and Proteus mirabilis, both susceptible to ciprofloxacin, which was continued until 10 days after surgery, whereas lavage was stopped on day 6. The double-lumen catheter was removed, leading to complete healing of the cutaneous incision. Similarly, the abdominal wall abscesses resolved in two weeks.
Only two cases of vesicocutaneous fistula secondary to giant vesical stones have been reported before [5]. In both of those cases, the fistula developed in surgical abdominal-wall scars. In this situation, the formation of a fistula within the soft tissues and the rectal muscles is facilitated by the weakening of the abdominal wall, whereas in our case, a fistula and abscesses developed in an intact abdominal wall, making the event rarer still. Vesical diverticula, recurrent bladder infections, intravesical foreign bodies, neurogenic bladder, indavir antiretroviral therapy, and permanent catheters are risk factors for the development of calculi. In such cases, urine acidification with
Vesicocutaneous fistula is rare, but can originate even in the absence of previous abdominal scars and can lead to potentially fatal sepsis, especially if it remains undiagnosed in older patients with co-morbidities. Many risk factors are to be considered for the development of GBC, including the loss of bladder clearance mechanisms associated with permanent nephrostomy or long-term dialysis. In patients with reduced urine output or obstructive disease, the presence of vesical calculi should be monitored to avoid serious complications such as sepsis or organ perforation. Furthermore, in subjects with permanent catheters, continuous urine acidification is advocated to reduce the risk of catheter encrustation and consequent stone formation.