
Abstract
Abstract
Background:
Guidelines advise that patients with ventilator-associated pneumonia (VAP) should respond clinically by Day 3 of antibiotics. White blood cell (WBC) count, maximum temperature (Tmax), and PaO2:FIO2 ratio are all said to respond significantly by Day 6. Resolution of abnormalities has not been evaluated in trauma patients.
Methods:
Retrospective review of trauma patients with VAP. The WBC count, Tmax, and PaO2:FIO2 were evaluated for 16 days after diagnosis. Patients were grouped into uncomplicated VAP, complicated VAP (those with inadequate empirical therapy [IEAT], VAP relapse/superinfection, or acute respiratory distress syndrome), and concurrent infection+VAP (those also infected at another site).
Results:
There were 126 patients (uncomplicated VAP=29, complicated VAP=69, and concurrent infection+VAP=28). The mean Tmax in patients with uncomplicated VAP decreased significantly from diagnosis to Day 4 (Day 1: 39±0.5°C vs. Day 4: 38.6±0.7°C; p=0.028) but never normalized. Their WBC counts and PaO2:FIO2 did not change significantly over the 16-day follow-up and never normalized. When comparing the three groups, the probability of resolving all three abnormalities was not different (p=0.5).
Conclusions:
Clinical and laboratory abnormalities in critically injured patients with VAP do not resolve as quickly as suggested in the guidelines. Future studies should evaluate new methods to determine the response to antibiotic therapy in critically injured patients with VAP.
However, trauma patients are a unique population that may respond to VAP treatment differently than do general medical/surgical intensive care unit (ICU) patients. Traumatic injury can induce the systemic inflammatory response syndrome (SIRS), contributing to derangements of clinical measures used to determine the response to VAP therapy. As many as 91% of trauma patients exhibit signs of SIRS during the first week in the ICU [4]. In addition, a composite score of clinical measures (Clinical Pulmonary Infection Score [CPIS]) used for VAP diagnosis in some medical ICUs does not perform well in critically injured patients, making it a poor choice for evaluating the response to therapy [5].
We hypothesized that clinical and laboratory abnormalities in patients with no confounders would decline significantly after VAP, whereas those in patients with confounders would stay elevated throughout follow-up. Additionally, because there are insufficient data to characterize the clinical and laboratory response to VAP in critically injured patients, we evaluated the resolution of clinical and laboratory abnormalities retrospectively in these patients after diagnosis and appropriate treatment of VAP.
Patients and Methods
Following approval by the University of Tennessee Institutional Review Board (IRB number 09-00277-XM), this retrospective review was conducted at the Presley Memorial Trauma Center, Memphis, TN. Patients admitted from December 1, 2006, through July 31, 2008, were eligible if they were ≥18 years of age and had VAP diagnosed. Patients who died during treatment were excluded, as their elevated values prior to death could mask overall resolution in the group. Patients receiving steroids also were excluded in order to avoid misinterpretation of Tmax and WBC count.
Diagnosis and treatment of VAP
Ventilator-associated pneumonia was suspected if patients had a new or changing infiltrate on chest radiograph and experienced two of the following clinical signs: fever or hypothermia (>38°C or <36°C), leukocytosis or leukopenia (>10×103 cells/mm3 or <4×103 cells/mm3), or macroscopically purulent sputum. The VAP diagnosis was confirmed using bronchoscopic bronchoalveolar lavage (BAL) with quantitative culture demonstrating bacterial growth ≥100,000 colony-forming units (CFU)/mL. Empirical antibiotic therapy was initiated in all patients immediately after the BAL. All patients were treated for suspected VAP using a unit-specific protocol [5,6–8]. Thus, patients admitted to the trauma intensive care unit (TICU) for ≤7 days received ampicillin/sulbactam 3 g intravenously (IV) every 6 h, or moxifloxacin 400 mg IV every 24 h in those with penicillin allergy. Patients mechanically ventilated for ≥7 days received vancomycin 20 mg/kg IV q 12 h plus cefepime 2 g IV q 8 h, or ciprofloxacin 400 mg IV q 8 h for those with penicillin allergy. On identification of the causative pathogen, antibiotic therapy was narrowed appropriately. Based on previous data, the treatment protocol dictates that patients with early VAP (<7 days) be treated for seven days [7]. For late VAP, the protocol recommends a follow-up BAL to determine microbiologic response to antibiotic therapy, if possible. A follow-up BAL demonstrating growth of the original pathogen of <10,000 CFU/mL is deemed a microbiologic response. If growth is 10,000–99,999 CFU/mL, antibiotics are continued for the maximum duration to ensure appropriate treatment. If culture of an organism yields ≥100,000 CFU/mL, the BAL finding is deemed a relapse or superinfection (depending on the original pathogen). The protocol recommends a maximum duration of therapy of 14 days for late pathogens such as methicillin-resistant Staphylococcus aureus (MRSA), Pseudomonas aeruginosa, or Acinetobacter baumannii [9]. If patients' signs and symptoms are not resolving while the patient is being treated, the protocol recommends continuing to search for new or recurrent infections as indicated (subsequent BALs, blood cultures, urine cultures, etc.). If the signs of VAP are not resolved at the end of antibiotic therapy, antibiotics are stopped, and the search for occult infections continues. Extreme cases such as hemodynamic instability could warrant continuation of antibiotics, but this is not common. This approach is supported by repeat microbiologic culture data from our institution [7,9].
Study groups
All patients experienced VAP, were treated with appropriate definitive antibiotics, and survived the VAP episode. Patients were categorized into one of three groups based on complicating factors that could affect the resolution of clinical evidence of disease. Patients with VAP who were treated appropriately, did not acquire any other infections, and did not have any of the complicating factors listed below were placed in the uncomplicated VAP group. Patients with complications that could relate to VAP, such as inadequate empiric antibiotic therapy (IEAT), VAP relapse, VAP superinfection, or acute respiratory distress syndrome (ARDS), were placed in the complicated VAP group. Patients with concurrent infection(s) at another site were placed in the concurrent infection+VAP group.
Definitions
The adequacy of empiric therapy was determined for each VAP episode. IEAT was defined as VAP caused by at least one bacterial species reported to have either intermediate or full in vitro resistance to all empirical antibiotics. Empiric antibiotic therapy was considered adequate if at least one antibiotic in the regimen demonstrated in vitro activity against all identified pathogens. The treating physician diagnosed ARDS using standard criteria that included acute onset, bilateral infiltrates on chest radiograph, exclusion of cardiogenic pulmonary edema, and a PaO2:FIO2 <200 . Additional infections were defined as follows: VAP relapse, a subsequent BAL demonstrating growth of the original pathogen ≥100,000 CFU/mL; VAP superinfection, a subsequent BAL demonstrating growth of a different pathogen ≥100,000 CFU/mL, bacteremia/fungemia, growth from at least two bottles for S. epidermidis or from one bottle for all other bacteria or fungi; urinary tract infection (UTI), urine culture demonstrating bacterial or fungal growth ≥100,000 CFU/mL; surgical site infection, or any wound deemed infected by the treating surgeon and requiring antibiotic therapy.
Data collection
Demographic data, Injury Severity Score (ISS), duration of mechanical ventilation, and length of stay in the TICU and hospital were recorded. Patients were followed from the day the BAL was conducted (Day 1) through Day 16. Patients who were discharged from the ICU during the follow-up period were included in the final analysis. Patients discharged from the hospital are clinically stable. Therefore, unresolved clinical abnormalities were considered resolved on the day of discharge and were categorized as such through Day 16. The following clinical and laboratory data were recorded daily: Tmax, WBC count, and PaO2:FIO2. Resolution was defined as follows: Tmax≥36°C or ≤38°C, WBC count ≥4×103 cells/mm3 or ≤10×103 cells/mm3, and a PaO2:FIO2 ratio ≥250 [2,10]. The diagnosis of VAP does not require all disease features be abnormal; thus, resolution for individual measures was evaluated only in those patients with abnormal variables on the day of diagnosis.
Statistical analysis
Continuous variables were compared using the Student t-test for normally distributed variables or the Wilcoxon rank-sum test for non-normally distributed variables. Proportions were compared using the χ2 test. Repeated-measures analysis of variance was used to compare changes in clinical features over the 16-day follow-up period for the three groups. Multiple pairwise comparisons were made using the Holm-Sidak method. The Kaplan-Meier method was used to depict the probability of resolution of clinical and laboratory abnormalities. The log-rank test was used to compare two Kaplan-Meier curves. All statistics were calculated using SigmaPlot 11.1 software (Systat Software, Inc., San Jose, CA). Data are presented as mean±standard deviation (SD), mean±95% confidence interval (95% CI), median (interquartile range), or proportions, as indicated.
Results
A total of 142 patients with VAP were identified. Fifteen patients were excluded because of death during antibiotic therapy for VAP, and one was excluded because insufficient information was available. Therefore, 126 patients were analyzed. Twenty-nine patients (23%) had no complications during their VAP episode (uncomplicated VAP), whereas 69 patients (54.8%) experienced IEAT, a VAP relapse, superinfection, or ARDS during their VAP episode (complicated VAP). Twenty-eight patients (22.2%) had a concurrent UTI, bacteremia, or surgical site infection during their VAP episode (concurrent infection+VAP). Patient demographics were similar in all three groups (Table 1). It was not surprising that patients with complicated VAP had a significantly lower rate of early VAP (p=0.006) and a statistical trend toward a higher ISS (p=0.057).
Comparison between VAP only and VAP+confounders.
ARDS=acute respiratory distress syndrome; BAL=bronchoalveolar lavage; ICU=intensive care unit; IQR=interquartile range; SCI=spinal cord injury; SD=standard deviation; TBI=traumatic brain injury; VAP=ventilator-associated pneumonia.
The VAP pathogens are listed in Table 2. Of note, Haemophilus influenzae was the most common. Methicillin-resistant S. aureus accounted for 7.4% of organisms overall, 7.4% in the uncomplicated VAP group, 6.7% in the complicated VAP group, and 9.5% in the concurrent infection+VAP group.
Overall, 90 patients (71%) underwent one surgical procedure during the 16-day follow-up. This first operation was performed on average 5.4±4.5 days (range 1–15 days) after the diagnosis of VAP. Thirty-nine patients (31%) underwent a second operation 7.4±4.1 days after VAP diagnosis, and smaller numbers of patients underwent three, four, and five surgical procedures (14, 7, and 3 patients, respectively). Operation 1 occurred in 20 patients (69%) with uncomplicated VAP, 51 (74%) with complicated VAP, and 19 (68%) with concurrent infections+VAP. Operation 2 occurred in 10 patients (35%) with uncomplicated VAP, 23 (33%) of those with complicated VAP, and six patients (21%) with concurrent infections+VAP.
Changes in clinical and laboratory measures for all three groups are depicted in Figure 1. In patients with uncomplicated VAP and an elevated temperature at baseline, the earliest statistically significant decrease in Tmax occurred on Day 4 (Day 1: 39±0.5°C vs. Day 4: 38.6±0.7°C, p=0.028). However, the group's mean Tmax never dropped below 38°C (Day 16 mean Tmax 38.1±0.6°C). Patients with complicated VAP with an elevated baseline temperature demonstrated a statistically significant decrease in Tmax at Day 2 (Day 1: 39.1±0.5°C vs. Day 2: 38.7±0.8°C; p=0.047). Interestingly, the mean Tmax normalized on Day 16 in this group (mean 38±0.8°C). In the concurrent infection+VAP group, Tmax decreased significantly on Day 7 (Day 1: 39.2±0.5°C vs. Day 7: 38.5±0.7°C; p=0.005). The mean Tmax normalized on Day 13 (mean 38±0.8°C), but then increased again and normalized on Day 16 (mean 37.9±0.8°C).
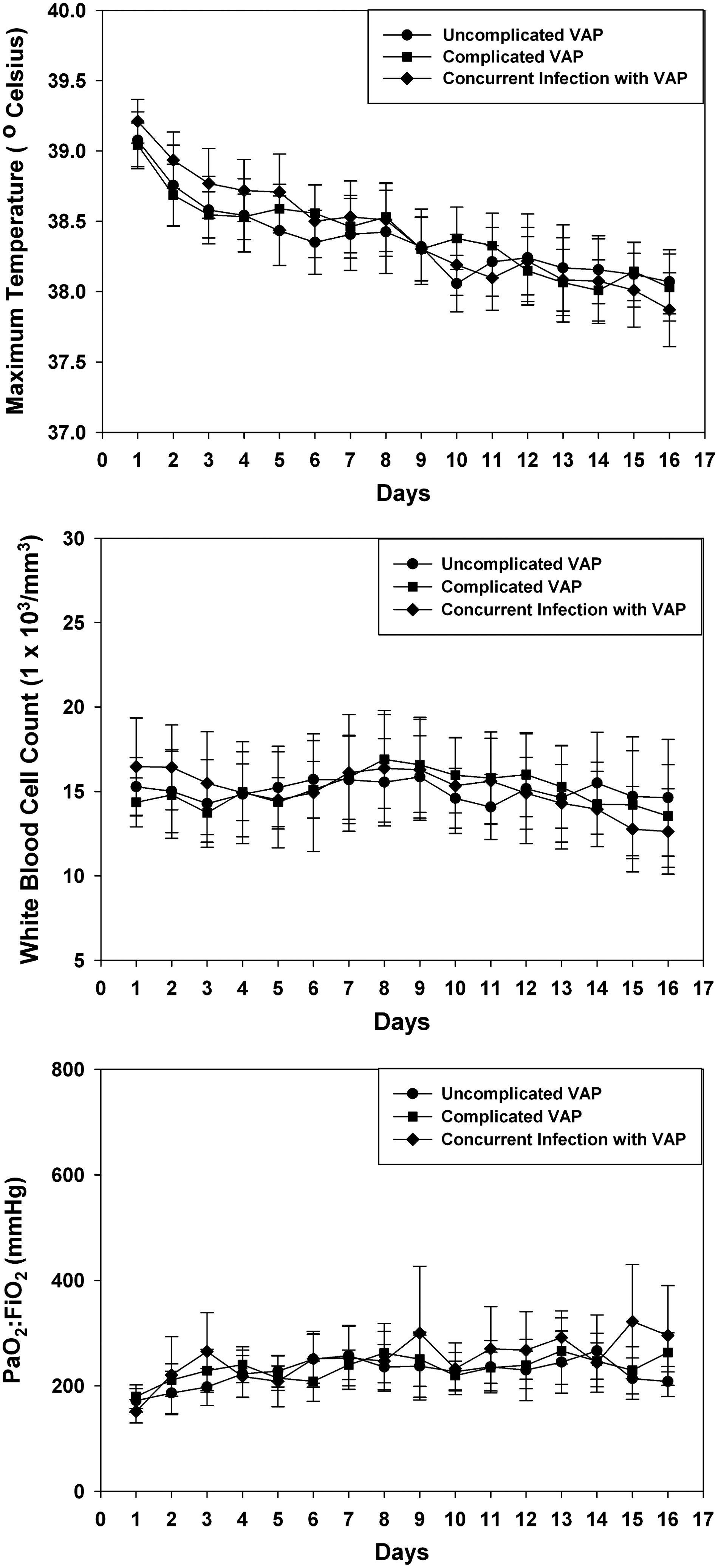
Mean values for clinical and laboratory measures after diagnosis of ventilator-associated pneumonia. Day 1 is the day bronchoalveolar lavage was conducted to verify the pneumonia.
In patients with an elevated baseline WBC count, there was no statistically significant change over the 16-day follow-up (uncomplicated VAP p=0.26; Complicated VAP p=0.097; concurrent infection+VAP p=0.09), and the mean WBC count never normalized in any of the three groups. The PaO2:FIO2 in the uncomplicated VAP and concurrent infection+VAP groups did not change significantly (p=0.058 and 0.197, respectively), whereas the complicated VAP group demonstrated a significant decrease at Day 3 (Day 1: 170±67 vs. Day 3: 246±158; p=0.033). The PaO2:FIO2 fluctuated by worsening on Days 4–6, but improving significantly on Days 8, 9, 13, and 16.
The proportions of patients whose clinical and laboratory abnormalities resolved on Days 3, 6, 9, 12, and 16 are presented in Table 3. The majority of patients in all three groups did not achieve resolution by Day 6. Even by Day 16, resolution was less common than had been expected. The probability of resolving all three abnormalities is displayed in Figure 2. Kaplan-Meier log-rank analysis demonstrated no significant difference between patients with uncomplicated VAP, complicated VAP, and concurrent infection+VAP. In addition, similar results were seen when patients were categorized according to the timing of VAP (early or late) or whether the VAP was caused by non-fermenting gram-negative bacilli (data not shown).

Kaplan-Meier graph depicting the probability that all three abnormalities (maximum temperature, white blood cell count, and PaO2:FIO2) will not resolve over the 16-day follow-up period. There was no difference in the probability of non-resolution (p=0.5).
Discussion
This retrospective study raises serious concerns about the value of the traditional measures used to assess VAP treatment in trauma patients. According to the current American Thoracic Society/Infectious Diseases Society of America (ATS/IDSA) guidelines [1], the uncomplicated VAP group should have demonstrated a clear response to therapy by Day 3 and a substantive response by Day 6. However, in this group, the Tmax was the only measure to decline significantly during the 16-day follow-up. Although the decline was statistically significant, it was likely not clinically significant, being approximately 0.4°C by Day 4. Indeed, the group mean never normalized. The WBC count and PaO2:FIO2 never declined significantly and never normalized. These findings seem valid because the uncomplicated VAP group had no concomitant infections or complicating factors related to VAP that may have kept the clinical and laboratory abnormalities from resolving. Also, all patients in this group were confirmed to have had a positive microbiologic response to treatment according to a follow-up BAL. Furthermore, the clinical response did not differentiate patients with uncomplicated VAP, complicated VAP, or concurrent infection+VAP. Traditional medical belief dictates that there probably would have been a clear difference in the resolution of the clinical and laboratory abnormalities in these groups. Unfortunately, in these critically injured patients, resolution of all disease measures was poor in each of the three groups (less than 35% by Day 16) despite successful treatment of their VAP. Additionally, the probability of resolution of all three measures did not differ between groups. Overall, these results suggest that the current guidelines do not apply well to trauma patients.
There are only a few studies that have evaluated this issue. The study most similar in design to the current one was performed by Dennesen et al. [2], but their results were different from ours. They noted Tmax and WBC count declined and the PaO2:FIO2 increased after VAP. However, it is important to note that they enrolled medical, surgical, trauma, and neurologic patients, whereas the current study included only trauma patients. In addition, in the current study, the WBC count and Tmax were higher, and the PaO2:FIO2 was lower, on the day of VAP diagnosis than in the study by Dennesen et al. (WBC 15.1±3.8×103 cells/mm3 vs. 14.2±5.4×103 cells/mm3, Tmax 39±0.6°C vs. 38.8±0.5°C, PaO2:FIO2 176±55 vs. 197±79). Perhaps the patients in the current study were more seriously ill at the onset of infection. Moreover, Dennesen et al. used a resolution cutoff for the PaO2:FIO2 of 188, which is lower than that used in the current study and by others [10,11]. Another difference is that the diagnostic criteria for VAP in the current study were more rigorous. Dennesen et al. did not define their diagnostic threshold, whereas the current study used ≥100,000 CFU/mL, which is recommended in the ATS/IDSA guidelines but is not accepted universally. Finally, the paper by Dennesen et al. is somewhat confusing because they report a mean duration until resolution of six days for all three signs, whereas their graph indicates that the mean WBC count never normalized.
Other studies were similar to the current study in showing that clinical and laboratory abnormalities do not resolve quickly or cleanly during VAP. A large randomized trial [12] noted only a small decline in mean temperature after treatment of VAP (Day 1 ∼38.6°C, Day 2 ∼38.1°C). Although the temperature responded to antibiotic therapy within three days, the mean PaO2:FIO2 did not increase above 250 until after Day 7, and the mean WBC count remained above 10×103 cells/mcL through Day 28.
A related issue is the possibility that IEAT or specific pathogens can affect resolution of disease. Vidaur et al. reported the clinical resolution of 60 patients with adequate empiric therapy and 30 with inadequate therapy [10]. Inadequate EAT delayed the median time to resolution of fever, hypoxemia, and WBC count by 5–7 days, 6–8 days, and 3–5 days, respectively. Infection with MRSA increased the time to resolution of disease regardless of IEAT status. These data highlight additional factors that must be considered when evaluating the treatment response. In the current study, patients experiencing IEAT were separated from those receiving appropriate therapy. Patients with MRSA VAP were not grouped separately because the incidence of MRSA was similar in the three groups (uncomplicated VAP 7.4%, complicated VAP 6.7%, and concurrent infection+VAP 9.5%). Thus, these factors are unlikely to explain the delayed response seen in the current study.
The lack of resolution in the current study likely is multifactorial. Surgery has been associated with elevations in temperature and WBC count even if the patient does not have an infection [13]. Thus, the multiple surgical procedures performed in the study patients may have masked a clinical response to antibiotics by altering temperature and WBC count. Additionally, more than one-half of the patients had early VAP (<7 days), suggesting the presence of SIRS as a result of their original trauma [4].
New methods must be identified for evaluating the response of trauma patients to VAP therapy. Repeat BAL cultures can be used [7,14] and were the standard of practice in the current study. Unlike clinical measures, repeat cultures are not affected by non-infectious variables and thus are a more objective marker. Mueller et al. noted shorter durations of antibiotic therapy when repeat BAL cultures were used [7]. Microbiologic data could reduce clinicians' reliance on other laboratory data, especially in trauma patients. However, repeat cultures are invasive and can be expensive, depending on the techniques used. Alternatively, biomarkers such as procalcitonin may be able to signal response to therapy [15], and in one study this protein was not affected by surgery [16]. A recent meta-analysis of seven studies showed that procalcitonin monitoring decreased the duration of antibiotics in patients with respiratory tract infections [15].
The current study has several limitations. The data were collected retrospectively, which is inherently less specific than a prospective study. However, the variables were recorded accurately and would not have been different if collected prospectively. Second, a diagnostic threshold for VAP of ≥100,000 CFU/mL is higher than the ≥10,000 CFU/mL used by many institutions. The larger bacterial load may result in a longer time to resolution of clinical and laboratory abnormalities. Finally, the study enrolled only 29 patients in the uncomplicated VAP group, which is the ideal study group for this problem. Although this number is relatively small, it is not substantially different from the enrollment in other published studies evaluating resolution of disease [2,3]. Indeed, the total number of patients across the three groups is good in relation to this body of literature. The strengths of the study include a relatively homogeneous population, the use of the highest-quality VAP diagnostic criteria, and a high percentage of patients with follow-up cultures that confirmed a positive response to treatment. The study enrolled only critically injured patients, a population that is inherently different from other critically ill patients. Use of bronchoscopic BAL with quantitative cultures ensured that the patients actually had VAP and thus eliminates bias from including patients without pneumonia.
Conclusion
Signs, symptoms, and laboratory abnormalities in critically injured trauma patients with VAP do not resolve as quickly as suggested by the guidelines. The probability of resolving all three clinical measures does not differ in patients with uncomplicated VAP and those with complications or concurrent infections. Future studies should evaluate new methods to determine the response to antibiotic therapy in critically injured patients with VAP.
Footnotes
Author Disclosure Statement
No competing financial interests exist for any of the authors.