
Abstract
Abstract
Background:
Arcanobacterium haemolyticum can cause severe systemic infections and sepsis. Thus, accurate and timely identification of the organism is essential.
Methods:
Case report and review of the pertinent English-language literature.
Case Report:
A 74-year-old male underwent repetitive surgical debridement and grafting for a full-thickness ulcer on the plantar surface of the left foot. One week after the last debridement, the patient presented to the emergency department with fever, hypotension, and severe left foot pain. A radiograph showed a soft-tissue defect of the plantar aspect of the left midfoot with gas along the lateral aspect of the fifth metatarsal. A below-knee amputation was performed. Blood culture and intraoperative tissue specimens grew colonies that exhibited β-hemolysis on sheep blood agar and agglutinated with streptococcal B group antiserum. However, gram staining revealed that the organism was a gram-positive bacillus, and a reverse Christie, Atkins, Munch-Peterson (CAMP) test showed that the organism inhibited the β-hemolysis of Staphylococcus aureus on sheep blood agar. Biochemical testing identified the organism as A. haemolyticum.
Conclusions:
It is important to investigate for A. haemolyticum when organisms with β-hemolytic activity react with group B streptococcal antiserum. Otherwise, A. haemolyticum can be mis-identified as group B Streptococcus or Listeria monocytogenes. This distinction is important clinically, because despite good in vitro activity of penicillin (a first-line antibiotic for group B Streptococcus infections), treatment failures have been reported when penicillin has been used for A. haemolyticum infections.
In this report, we describe a case of A. haemolyticum soft tissue infection and sepsis. We emphasize the importance of identifying the organism properly so that timely, appropriate treatment can be achieved.
Case Report
A 74-year-old male with a history of left-sided Charcot foot developed a 1×4-cm bullous lesion on the plantar surface of the left foot. Over the next three weeks, the lesion progressed to a full-thickness ulcer. A 10-day course of amoxicillin-clavulanic acid did not produce any improvement. Over the next two months, the ulcer was debrided repeatedly, and fibroblast mesh grafting material (Dermagraft; Advanced BioHealing, Inc., Westport, CT) was placed. One week after the last debridement, the patient presented to the emergency department with fever and severe left foot pain. His medical history was otherwise remarkable for hypertension and left-foot trauma sustained more than 50 years ago. He swam regularly at a fitness club for exercise.
On physical examination, the patient had a temperature of 38.5°C and a blood pressure of 80/40 mm Hg. His left foot was swollen and erythematous diffusely. A 2×4-cm ulcer with purulent drainage was present on the plantar surface. Laboratory data were notable for a white blood cell count of 18,600/mm3 with 89% neutrophils. A radiograph showed a soft tissue defect on the plantar aspect of the left midfoot with gas along the lateral aspect of the fifth metatarsal. Surgical exploration revealed extensive necrotic soft tissue and bone, and purulent material throughout the foot, ankle, and pre-tibial space. A left below-knee amputation was performed.
Cultures of tissue harvested intra-operatively grew bacteria that exhibited β-hemolysis on sheep blood agar. Streptococcal latex agglutination testing demonstrated that the organism agglutinated with streptococcal B group IgG-sensitized latex (PathoDx Strep Grouping Kit; Remel, Lenexa, KS). As a result, the organism was reported to be a group B β-hemolytic Streptococcus. The following day, a blood culture grew small gram-positive bacilli that also demonstrated β-hemolysis (Fig. 1). Re-examination of the tissue specimen revealed that it also contained a gram-positive bacillus. A reverse Christie, Atkins, Munch-Petersen (CAMP) test showed that the organism inhibited β-hemolysis of Staphylococcus aureus on sheep blood agar (Fig. 2). Biochemical testing (RapID CB Plus System, Oxoid Ltd., Basingstoke, United Kingdom) identified the organism as A. haemolyticum (99% probability). The patient was treated with a two-week course of piperacillin-tazobactam. More than one year later, he ambulates with a prosthesis and is otherwise well.
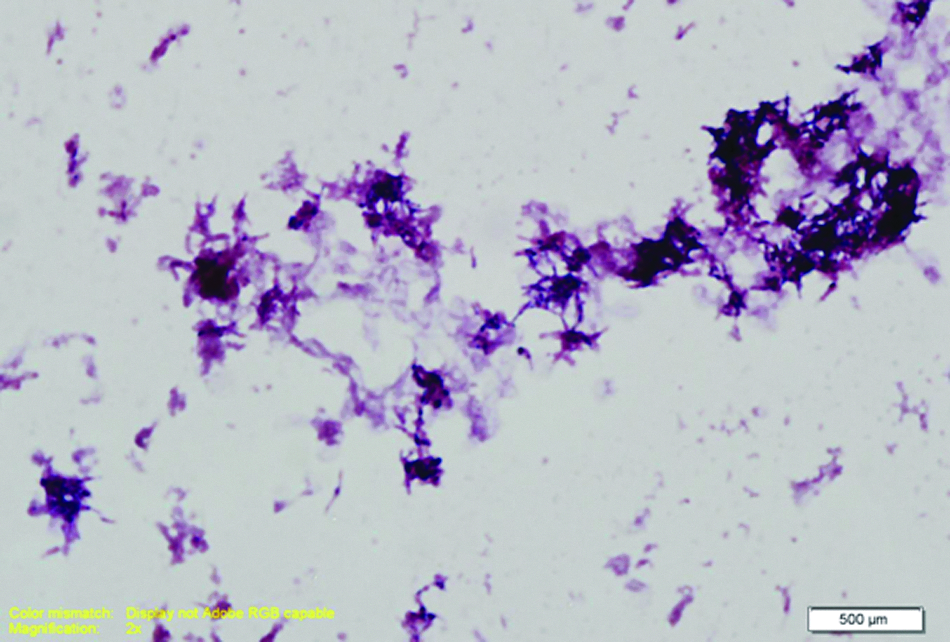
Gram stain of blood culture showing the gram-positive bacilli of Arcanobacterium haemolyticum. Color image is available online at www.liebertpub.com/sur

Reverse Christie, Atkins, Munch-Petersen test showing that Arcanobacterium haemolyticum inhibits the hemolytic zone of β-lysin-producing Staphylococcus aureus
Discussion
Arcanobacterium haemolyticum can cause severe morbidity and death. Hence, it is important to identify accurately and manage appropriately infections caused by this organism. The detection of A. haemolyticum by routine culture techniques can be challenging because of its slow growth, small colony size, and variable hemolytic activity on blood-based medium. It can take 24 h of growth before colonies become visible, and it may take 72 h before hemolysis is observed [1,11]. Growth of and β-hemolysis by A. haemolyticum are enhanced by the use of Trypticase soy agar with 5% sheep or horse blood and a 5% CO2 atmosphere [11–13]. Because of its phospholipase D activity, A. haemolyticum will inhibit the hemolytic zone of β-lysin-producing S. aureus, resulting in a positive reverse CAMP test [3,12].
With regard to the ability of A. haemolyticum to agglutinate with streptococcal antisera, the data are limited. It has been reported that A. haemolyticum does not cross-react with S. pyogenes or streptococcal G group antiserum [12]. To the best of our knowledge, it has not been reported that A. haemolyticum can cross-react with streptococcal B group antiserum. Because Listeria monocytogenes does demonstrate cross-reactivity with streptococcal B group antiserum, A. haemolyticum may be mis-identified as this organism as well. Moreover, because group B Streptococcus, L. monocytogenes, and A. haemolyticum all can exhibit β-hemolysis, it is essential to recognize that mis-identification may occur if a gram stain and biochemical testing are not performed.
Clinically, the distinctions among A. haemolyticum, group B Streptococcus, and L. monocytogenes are germane. Similar to A. haemolyticum, group B Streptococcus can cause severe infections, often stemming from skin or soft tissue [14]. However, proper differentiation among these organisms impacts treatment. β-Lactam antibiotics, macrolides, clindamycin, doxycycline, ciprofloxacin, and vancomycin have good activity in vitro against most strains of A. haemolyticum [15]. Nevertheless, treatment failures have been reported with therapeutic doses of penicillin [12,16]. This is important because penicillin, a first-line antibiotic for the treatment of group B streptococcal infections, may not be optimal for a patient with a severe, systemic infection caused by A. haemolyticum. Similarly, ampicillin, the first-line therapy for infections caused by L. monocytogenes, may not be appropriate for treating A. haemolyticum.
In conclusion, A. haemolyticum is capable of causing severe, systemic infections. This case illustrates that gram staining and biochemical evaluation for A. haemolyticum should be considered for throat, tissue, surgical specimens, or blood culture isolates that exhibit β-hemolysis and agglutinate with streptococcal B group antiserum. This is particularly important for severely ill patients or those who fail penicillin therapy for presumed streptococcal infections.
Footnotes
Author Disclosure Statement
The authors report no conflicts of interest.
No external funding was used.
This case report did not require ethical approval.