
Abstract
Abstract
Background:
Septic shock causing or complicating critical surgical illness results in high mortality. Drotrecogin alfa (activated), known also as recombinant human activated protein C (rhAPC) has become controversial as therapy, owing to persisting questions of efficacy and safety. We hypothesized rhAPC to be effective therapy for critically ill surgical patients with septic shock.
Methods:
Open-label therapy with rhAPC (by predefined criteria) of 108 critically ill surgical patients. Treated patients were matched individually in prospect for age, gender, Acute Physiology and Chronic Health Evaluation (APACHE)-II and –III scores, site of infection, and organism (0–2 points each, maximum 12 points) with 108 patients from our 15,000-patient surgical intensive care unit database who did not receive rhAPC. No match was accepted if <6 points. Multiple organ dysfunction (MOD) scores and data regarding cortisol concentrations, bleeding complications, and transfusion requirements were collected. The primary endpoint was 28-day mortality, with mortality for hospitalization and resolution of organ dysfunction as secondary endpoints. Statistical analyses included ANOVA, c statistic, binary logistic regression, and Kaplan-Meier time-to-event and Cox proportional hazards analyses; α=0.05.
Results:
The mean match score was 9.2±0.1 points (range, 6–12 points). Patients were well matched by all criteria, including baseline MOD score (9.5±0.7 vs. 9.8±0.3 points, p=0.66). Mean age was 68.1±1.1 years (p=0.49), Mean APACHE-III score was 99.6±1.5 points (p=0.87). Mean time to rhAPC administration was 25±3 h. Survival at 28 days after rhAPC was 71.3% vs. 49.1% (p=0.001); hospital survival was 57.4% vs. 40.7% (p=0.02). By logistic regression, rhAPC therapy resulted in improved 28-day survival (OR 2.57, 95% CI 1.46–4.52, p=0.001) (model χ2 11.244, p=0.001); and hospital survival (OR 1.96, 95% CI 1.14–3.36, p=0.015) (model χ2 6.03, p=0.014). The MOD score decreased significantly (p=0.012) during rhAPC therapy.
Conclusion:
Therapy with rhAPC appeared to improve survival in surgical ICU patients with life-threatening infection characterized by septic shock and organ dysfunction.
The mortality of intra-abdominal infection complicated by critical illness is approximately 22–30% [14]. Although contemporary critical care and improved source control may be reducing mortality [14], there is always the potential for improvement. Whether improved antibiotic therapy can yield incremental benefit is unknown, because critically ill patients are usually excluded from clinical trials. Thus, the optimal pharmacotherapy of serious infections of surgical patients is still being defined.
Drotrecogin alfa (activated) (Xigris®, Eli Lilly and Co., Inc., Indianapolis, IN), or recombinant human activated protein C (rhAPC), was approved in 2001 for the treatment of severe sepsis in patients with a high risk of death (i.e., Acute Physiology and Chronic Health Evaluation (APACHE)-II score ≥25 points, dysfunction of ≥2 organs). In a phase III trial (PROWESS), the risk of 30-day, all-cause mortality with severe sepsis was reduced by 6.1% [1], but apparently only among patients with an enrollment Acute Physiology and Chronic Health Evaluation (APACHE)-II score ≥25 points. Moreover, among the 532 “surgical” patients enrolled in PROWESS, mortality decreased only by 3.1% (p=NS), raising the question of efficacy for surgical sepsis, a concern compounded by questions of safety because of a perceived higher risk of bleeding after surgery.
A blinded post-hoc adjudication of the PROWESS database assessed the adequacy of surgical source control among 474 confirmed surgical patients [15]. The 28-day, all-cause reduction of mortality in high-risk (APACHE-II ≥25 points) intra-abdominal surgery patients treated with rhAPC (absolute risk reduction 18.2%; relative risk of death [RR] 0.60, 95% confidence interval [CI] 0.36-1.00) was consistent with the overall PROWESS study sample. Increased risk of bleeding in surgical patients was not detected.
Hypothesizing that rhAPC is efficacious for therapy of critically ill patients with intra-abdominal infection, a pilot prospective, matched-control, inception-cohort study was conducted (35 patients with intra-abdominal infection and septic shock, 35 control patients selected from our ICU database who were matched prospectively based on six criteria) [16]. Treated patients were extremely ill (mean APACHE III score, 102±2 points) and had substantial MODS. Mortality at 30 days was 30% for patients treated with rhAPC compared with 70% for the control patients (odds ratio (OR) for survival 5.29, 95% CI 1.85–15.10, p<0.0001). Patients who survived rhAPC therapy showed objective resolution of organ dysfunction before the 96-h infusion period was completed.
This study was undertaken to test further the hypothesis that treatment with rhAPC reduces mortality among critically ill surgical patients with infection, septic shock, and MODS. Although patients with non-abdominal infections were eligible for inclusion, the enrollment and case-matching criteria were essentially similar to the pilot study.
Patients and Methods
This study was a prospective, open-label, single-blind, comparative trial of rhAPC administration to critically ill surgical patients with infection and septic shock, as defined by consensus [17]. Informed consent was waived by the Committee on Human Rights and Research of Weill Cornell Medical College, because all patients received approved, indicated therapy.
Hospital and study inclusion and exclusion criteria were established to mimic as closely as possible the inclusion and exclusion criteria from PROWESS [1] (Table 1), excepting the requirement of septic shock. Consecutive patients were enrolled if they required surgical critical care for a surgically treated or post-operative infection, had MODS ≥ 2 organs, and required vasopressor therapy. Absolute contraindications included a high risk of bleeding after surgery, active hemorrhage, and expected survival of less than 24 h (Table 1).
Treated patients were compared with a cohort of patients who were treated previously in the surgical ICU, matched individually from a prospective database of more than 15,000 patients dating from January 1991, configured in prospect to de-identify patients and outcomes. After a patient began treatment with rhAPC, he or she was matched within 12 h by one of us (LJH), who had no clinical responsibilities and did not enter the ICU. Allocation and outcome of all matched patients were concealed until data lock.
Matching was performed with validated methodology [18], according to six criteria defined prospectively (Table 2): Age, gender, APACHE II and -III scores, infection-related diagnosis, and microbiology. Use of both APACHE II and -III scores ensured the closest possible match for severity of illness [19]. The closeness of the match for each parameter was awarded 0–2 points, thus a perfect match received 12 points. A patient was considered unmatched (and therefore excluded) if a minimum six-point match could not be achieved. All matching cases were selected from a time period as close to contemporaneous management as possible. When multiple candidate matches were identified for a treated case, the matching case treated most recently was chosen.
Patients were matched on six criteria; a perfect score was 12 points; whereas patients were considered unmatchable if a match of >6 points could not be found. Patients were matched by both APACHE II and APACHE III scores, so as to describe severity of illness with utmost precision (see text). “Same gram stain” refers to both patients having “gram-positive cocci,” “gram-negative bacilli,” or the like.
Demographic data collected included age, gender, admission diagnosis, site of perforation, APACHE II and –III scores, MOD scores (criteria of Marshall et al.; six organs, 0–4 point scale, maximum score 24 points) [5] on days 1–7, and the cumulative MOD score. In the cumulative score paradigm, points are awarded for worsening organ dysfunction, but not rescinded if organ function improved subsequently. Serial activated partial thromboplastin time (aPTT), serum glucose concentrations, and basal and stimulated (60 min after cosyntropin 1 mcg) cortisol concentrations were monitored. Transfusion of blood and blood products was recorded. Mortality was noted at 28 days and for the hospitalization.
The surgical ICU is “semi-closed,” with care coordinated with the surgical team but provided by surgical intensivists [20]. Sepsis care was provided according to Surviving Sepsis Campaign guidelines [21]. Empiric antibiotic therapy of complicated intra-abdominal infection and nosocomial pneumonia was administered according to guidelines of the Surgical Infection Society [22] and the American Thoracic Society [23], respectively, but administered by a “rotation” schedule (monthly rotation of cefepime, levofloxacin, imipenem-cilastatin, piperacillin-tazobactam; quarterly rotation of vancomycin and linezolid) [24]. Double-coverage (e.g., an aminoglycoside) of gram-negative sepsis was unusual. Empiric antifungal therapy was not administered unless the patient had a hospital-acquired perforated viscus (e.g., colon anastomotic dehiscence). Antibiotic therapy was de-escalated as appropriate based on the antibiotic susceptibility of isolated organisms.
Statistical analysis
Statistical analysis was performed using commercial software (SPSS 11.0 for Macintosh, SPSS, Inc., Chicago, IL). The study was designed to have 80% power to detect a 13% absolute decrease in mortality from therapy with drotrecogin alfa (activated) with 95% confidence. The primary endpoint was 28-day mortality. Secondary endpoints were mortality for the hospitalization and the resolution of organ dysfunction. Univariate analysis of coordinate variables was performed by chi-square contingency table analysis with the Fisher exact test, and univariate analysis of continuous variables was performed using the Mann-Whitney U-test. The Kolmogorov-Smirnov non-parameteric test was used to test differences in data that were not distributed normally. Changes in continuous variables with respect to time were analyzed by repeated measures analysis of variance (ANOVA) with the Tukey post-hoc test, and analyzed by the c statistic. Differences in mortality to 28 days were analyzed by Kaplan-Meier time-to-event analysis and compared by Cox proportional hazard ratio. Statistical significance was defined at α=0.05. Binary logistic regression was used to assess the independence of a single independent variable (therapy with rhAPC) upon mortality, considering that several “independent” variables of relevance to outcome were controlled for by the case-matching schema. The OR and 95% CI were determined, and the sensitivity, specificity, and goodness of fit (model χ2, Hosmer-Lemeshow test) were determined for the logistic regression model. Data are expressed as mean values±standard error.
Results
One hundred eight treated patients were compared with 108 individually matched control patients. Comparative demographics for the matched patients are listed in Table 3. The mean age of the 216 patients was 68.1±1.1 years, and the mean APACHE II and APACHE III scores were 28.6±0.4 and 99.6±1.5 points, respectively. The mean MOD score was 9.6±1.5 points at study entry. None of these values differed between groups. The results of the matching process are shown in Table 4 and Figure 1. All treated patients were matched without exception. The mean matching score was 9.2±0.1 points, with comparable degrees of matching for all six components. Ninety-five percent of matched patients received at least an eight-point match.
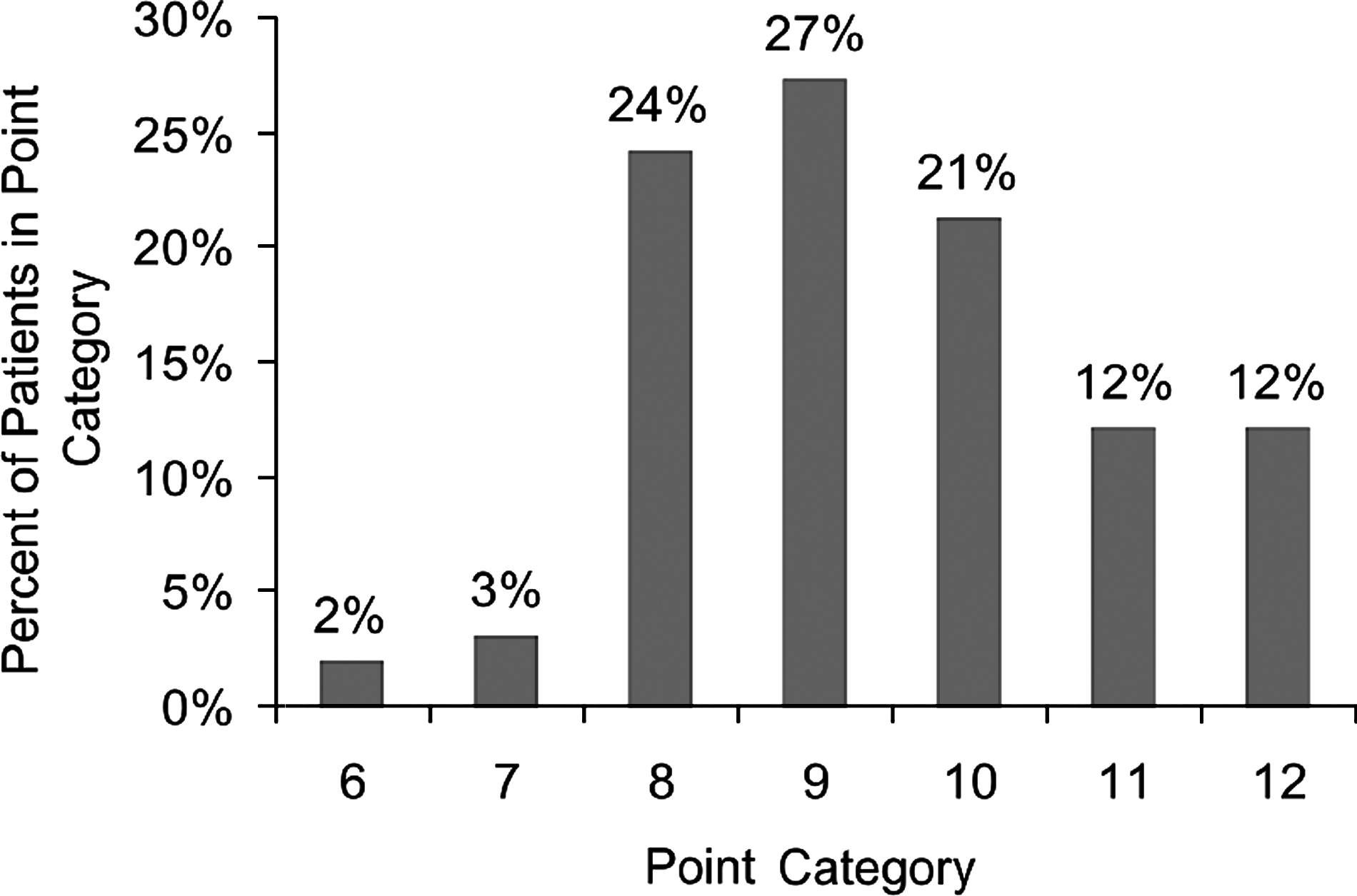
Frequency distribution of the matching scores.
APACHE=Acute Physiology and Chronic Health Evaluation; MOD=multiple organ dysfunction.
APACHE=Acute Physiology and Chronic Health Evaluation; MOD=multiple organ dysfunction; SEM=standard error of the mean.
Among patients operated on for source control of intra-abdominal infection (72/108, 66.6%), rhAPC was initiated 25±3 h after surgery (29/72, 40.2% within 24 h). The infusion was stopped for 10/108 patients (9.3%) to manage bleeding (n=4) or anemia (n=6) with transfusions of blood and blood products (Table 5). The infusion was resumed and completed for all 10 patients who were transfused, for 100% completion of the intended 96-h infusion. Patients treated with rhAPC were likely to develop an increased aPTT. The aPTT was prolonged throughout the infusion period compared with matched controls (Fig. 2). Mean aPTT increased from 38.7±1.2 seconds to 64.6±3.1 seconds by 12.8±1.3 h after the initiation of therapy, and increased above the upper limit of normal for the assay in 64.8% of patients. Fresh frozen plasma was administered if the aPTT increased above 60 seconds, regardless of the status of hemostasis. The incidence of FFP transfusion was 38.5% among rhAPC-treated patients, totaling 1.6±0.3 units. Mean basal and 60-min stimulated serum cortisol concentrations did not change in either the rhAPC–treated patients or matched controls (34.9±8.1 vs. 29.7±2.3 mcg/dL, p=0.494, zero vs. 60 min, matched cohort; 33.0±6.5 vs. 35.8±2.8 mcg/dL, p=0.776, zero vs. 60 min, rhAPC).

Mean activated partial thromboplastin times (in seconds), recombinant human activated protein C (rhAPC)-treated patients and matched control patients, during infusion.
Non-specific decrease of hematocrit to transfusion trigger (n=6, 4.8%)-all transfused
rhAPC therapy was contraindicated in this trauma patient with traumatic brain injury
rhAPC=recombinant human activated protein C.
Patients treated with rhAPC were significantly more likely to survive to the 28-day primary endpoint and the hospital discharge secondary endpoint. Survival at 28 days was 71.3% vs. 49.1% (p<0.001) for an absolute reduction of the risk of death of 22.2% and a relative risk reduction of 44.0%. Survival to hospital discharge was 57.7% vs. 40.7% (p=0.02), for an absolute reduction of the risk of death of 17.0% and a relative risk reduction of 29.0%. The Kaplan-Meier analysis of mortality is shown in Figure 3; the survival benefit of rhAPC therapy was significant out to more than 90 days. (p<0.01). By binary logistic regression, rhAPC-treated patients were more than twice as likely to survive to 28 days (OR 2.58, 95% CI 1.47-4.52), and nearly twice as likely to survive to hospital discharge (OR 1.96, 95% CI 1.14–3.36, with good model calibration and discrimination for both (Table 6). Among the 72 rhAPC-treated patients with complicated intra-abdominal infections, 71.6% were alive at 28 days vs. 48.5% of patients in the matched cohort (p=0.004). Among the 36 rhAPC-treated patients with all other types of infections (ventilator-associated pneumonia, most commonly), 70.6% were alive at 28 days vs. 50% of patients in the matched cohort (p=0.059). Binary logistic regression of 28-day mortality in the infection type subsets confirmed these observations, including the trend toward efficacy for “other” infections.
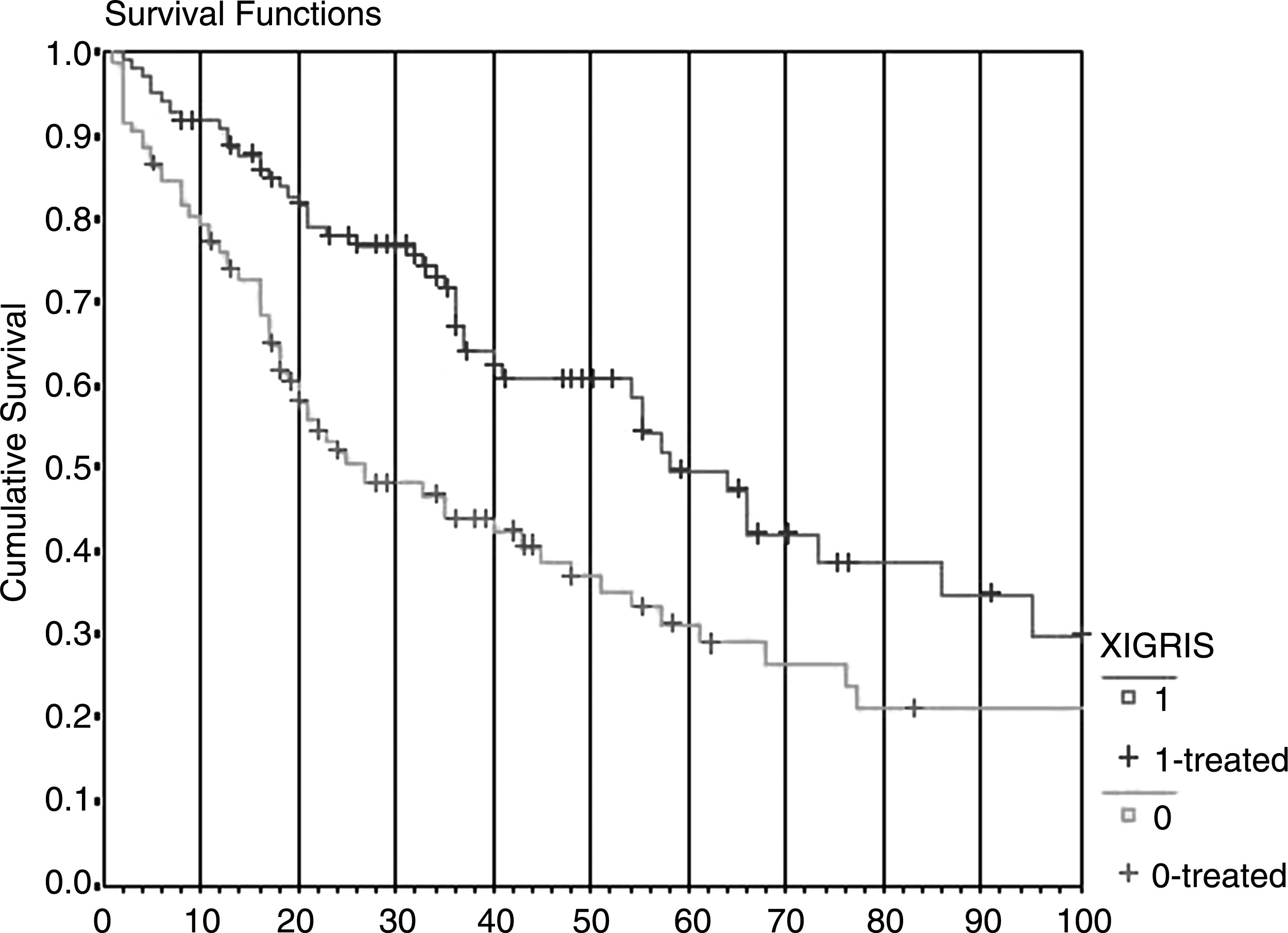
Therapy with recombinant human activated protein C (Xigris) increased survival significantly (p<0.01) at both 28 days and at hospital discharge, compared with untreated matched controls. The survival curves are also statistically distinct at 100 days post-therapy (p<0.05).
OR=odds ratio; CI=confidence interval.
Although the initial magnitude of organ dysfunction was comparable between treated and matched patients (9.8±0.4 vs. 9.5±0.7 points, respectively, p=0.66), statistically significant improvement of organ function (p<0.05) was observed during rhAPC therapy before the 96-hour infusion was completed, compared with matched controls (Fig. 4). The improvement in MOD scores was a significant predictor of outcome as analyzed by the c statistic and displayed by receiver-operator characteristic curves (Fig. 5). Length of stay in the ICU (ULOS) and hospital (HLOS) were longer after rhAPC therapy despite comparable severity of illness. For ULOS, there was a trend toward longer duration (28±3 vs. 18±2 days, p=0.068), whereas HLOS was prolonged unequivocally (47±6 vs. 34±4 days, p=0.006), likely a direct reflection of increased survival.
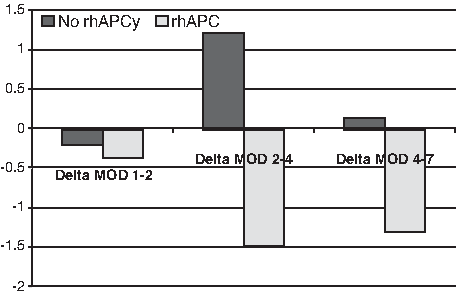
Daily changes of multiple organ dysfunction score among recombinant human activated protein C (rhAPC)-treated patients stratified by hospital survival. The differences at days 2–4 and 4–7 are statistically significant.
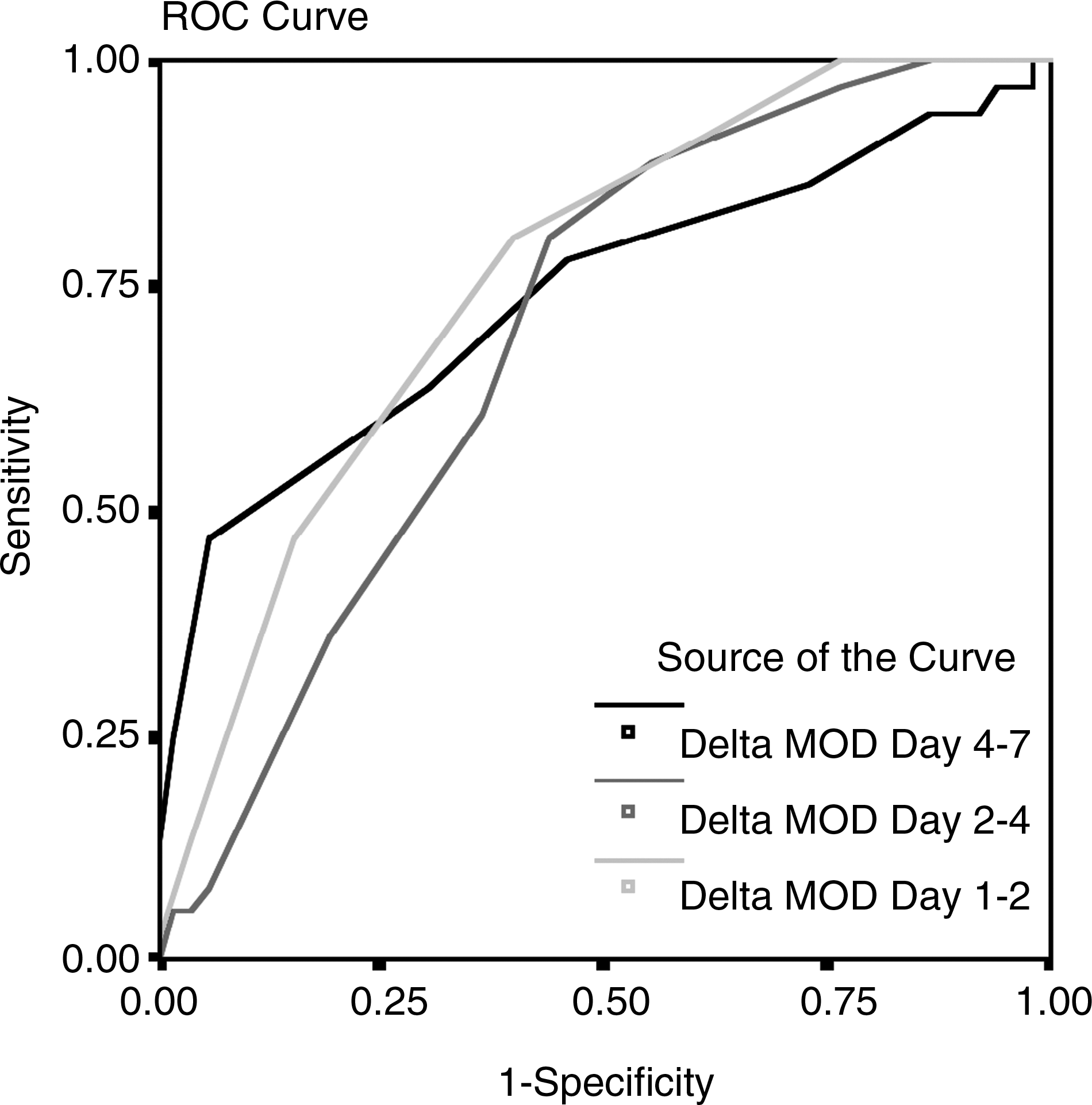
Influence of change in daily multiple organ dysfunction (MOD) scores during recombinant human activated protein C (rhAPC) infusion on mortality from septic shock in surgical patients. The areas under the receiver-operator characteristic curves are 0.759 (day 1 to 2), 0.696 (day 2 to 4), and 0.737 (day 4 to 7) (all p<0.05).
Discussion
Compared with matched controls, critically ill surgical patients treated with rhAPC for septic shock had significantly improved survival with an associated resolution of organ dysfunction. The observed reduction of risk was greater than that observed by PROWESS [1], from analysis of the sickest 50% of patients from PROWESS (APACHE II ≥25 points), and from analysis of the cohort of surgical patients from PROWESS [17]. These results may have been due to the focus on high severity of illness, or to the emphasis on administration of drug within 24 h, which has been associated with improved outcomes [2]. Therapy of intra-abdominal infection was particularly effective.
Our cohort-matching strategy creating equivalent groups for comparison. Potential assignment bias was minimized by assigning the process to an individual who had no clinical responsibilities, before the outcomes of the rhAPC-treated patients were known. Using the 12-point scale, comparators were selected based on the closest match; a “perfect” (12-point) match was achieved for 13 patients, and a majority had a match of eight points or better. Examples of temporal bias include the reduced mortality that may have resulted from faster resolution of organ dysfunction, which may also be attributable to improved glycemic control; a protocol for glycemic control was followed during the rhAPC therapy period [25], but not for some of the matched controls. It is also possible that the observed effects are attributable to some imperceptible effect other than therapy with rhAPC, such as improved surgical source control, or changes in the way antimicrobial agents were administered. The latter is unlikely, given that antibiotics are administered by protocol and that initial antimicrobial therapy was appropriate in more than 90% of cases [24].
The open-label cohort-matching design was chosen because, at the time the study was designed, a randomized, placebo-controlled trial of approved therapy raised ethical questions regarding the withholding of therapy for the purpose of the study. However, controversy developed subsequently because of the publication of non-confirmatory trials [26], and equipoise supported the conduct of a randomized, double-blind, placebo-controlled trial of rhAPC for therapy of septic shock (PROWESS-SHOCK) [27–30]. The patient population studied herein fell clearly within the population indicated in the product literature, but given that media reports indicate that PROWESS-SHOCK was a negative study and that rhAPC was withdrawn from the market worldwide on October 25, 2011 [31,32], questions of efficacy and safety have been rendered moot, and now will center on why PROWESS-SHOCK failed.
The limitations of the study are several. Foremost, this was not a randomized controlled trial, and some other aspects of critical care therapeutics did change during the study period, but the rigor of the cohort matching process should have mitigated that effect. An alternative to matching individual patients by specific criteria would have been to calculate a propensity score for therapy with rhAPC based on measured variables, and match based on the propensity score [33]. Propensity scores have been validated for comparisons of groups treated and not treated, but rhAPC was not available clinically during some of the time period when the matching patients were treated, hence there was no propensity whatsoever for their treatment with rhAPC, and therefore no treatment selection bias. Propensity score methods do reduce bias by 2–13% in the estimation of marginal ORs compared with logistic regression [34,35], but not to the degree that this study would have produced different results.
Footnotes
Author Disclosure Statement
Doctor Barie is a consultant to and has received honoraria from Eli Lilly and Co., Inc., and is a member of the Academic Steering Committee for the PROWESS-SHOCK trial. None of the other authors have a conflicting financial interest.