
Abstract

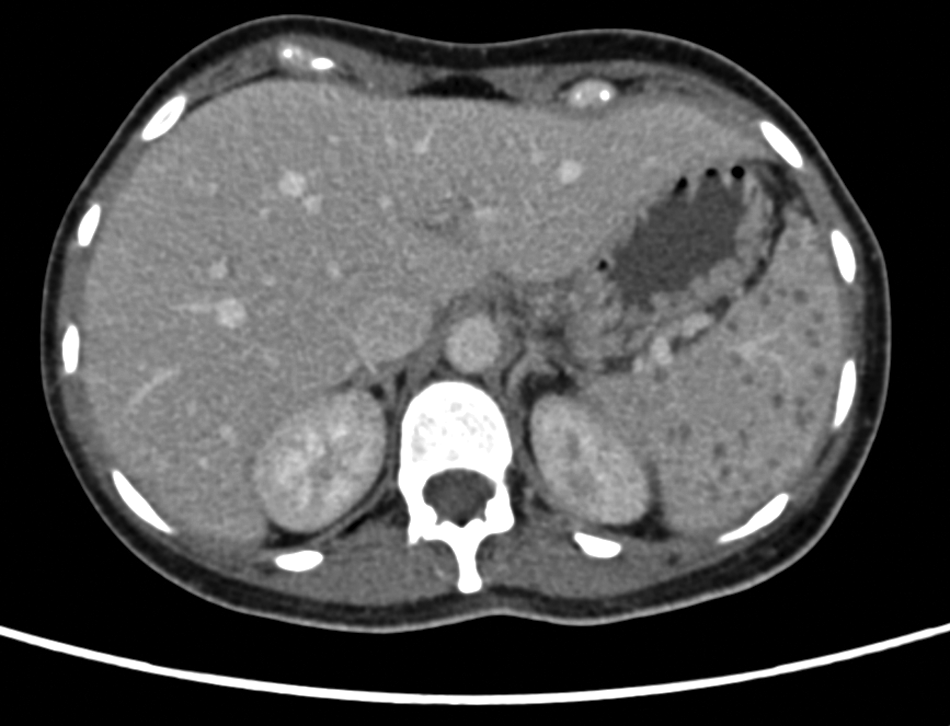
Multiple hypodense splenic nodules on abdominal computed tomography scan.
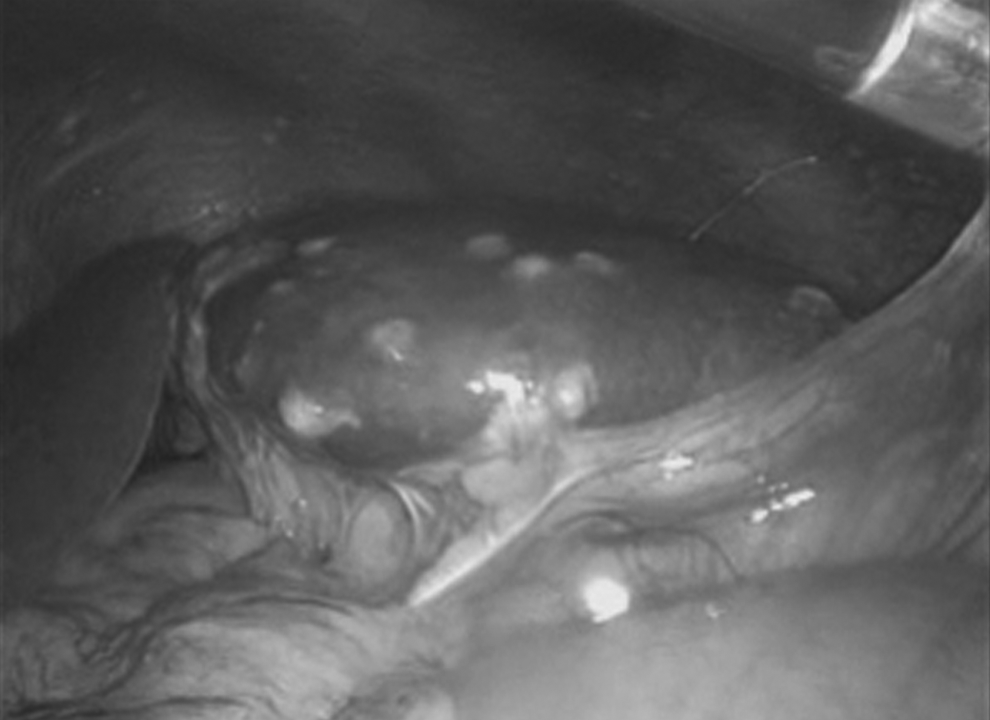
Laparoscopic view of spleen.
Except in trauma, splenic pathology is rare and is represented mainly by benign or malignant lesions, infectious causes, and hematologic disorders. Splenic abscesses have been associated with different microorganisms, including aerobic bacteria (Streptococcus spp., Staphylococcus spp., Salmonella spp., Pseudomonas, Escherichia coli, Enterococcus spp., Klebsiella, and Proteus), anaerobic bacteria (M. tuberculosis and M. avium complex), and fungi [1]. Splenic tuberculosis represents an extremely rare entity; there are just small series and a few isolated case reports in the literature. Splenic infection by M. tuberculosis may occur as primary involvement of the spleen or during miliary tuberculosis [2]. Presenting symptoms may be related to systemic tuberculosis infection or to direct splenic involvement, which may produce left upper-quadrant pain, ascites, and splenomegaly [3]. The radiologic features are splenomegaly, a solitary mass, or multifocal hypodense nodular lesions [3].
In some scenarios, splenectomy represents both a diagnostic and a therapeutic intervention. There are case reports in which the diagnosis was made with a percutaneous biopsy, and patients were treated successfully with antituberculous drugs [4]. Laparoscopy is a minimally invasive approach for diagnosis or treatment for this rare condition [5].