
Abstract
Abstract
Background:
Abscesses involving the inguinal region are uncommon as manifestations of complex soft-tissue infections or intra-abdominal pathology, and the routes by which they cause infection are usually unclear and may be overlooked.
Methods:
A comprehensive review of reports in the English language literature of the clinical presentations, outcomes, and causes of abscess in the inguinal/groin area requiring surgical intervention. The cases of 33 patients, including 30 patients in 27 reports in the literature and 3 patients in the Chang Gung Memorial Hospital at Chia-Yi, were reviewed to determine the ages, positions, gender, hypothesized causes, diagnostic modalities, and clinical outcomes of abscesses in the inguinal/groin area. Clinical data, laboratory examination findings, and culture results were analyzed.
Results:
Inguinal abscesses presented as tender inguinal masses that could extend from gastrointestinal, genitourinary, or retroperitoneal sites as well as being of miscellaneous origin. Most patients with such abscesses presented with fever and leukocytosis. Computed tomography provided a sensitive means for establishing the correct diagnosis and surgical plan of treatment for inguinal sbscesses. Gram-positive pathogens were associated with infections involving hip or thigh muscles and gram-negative pathogens were associated with infections involving the gastrointestinal (GI) and genitourinary (GU) tracts as well as with abscesses of the psoas muscle,
Discussion:
The inguinal region communicates through several routes with the peritoneal and retroperitoneal spaces as well as with the region of the thigh. The lymphatics drain from the external genitalia, inferior anal canal or perianal region, adjoining abdominal wall, and the lower extremities. Evaluation of a patient with inguinal abscess and with signs of infection should include computed tomography (CT) to elucidate the extent of infectious disease. Information obtained from CT is important in guiding the prescription of antibiotics and surgical planning for the treatment of inguinal abscesses.
Conclusions:
Computed tomography is helpful in diagnosing inguinal abscess and determining the extent of infection. In patients presenting with inguinal abscess. Early recognition of its origin can facilitate further surgical planning and possibly improve the outcome.
S
Inguinal abscesses resulting from pyomyositis in the thigh usually appear as well-defined cavities, whereas those resulting from intraperitoneal or retroperitoneal infections may be complicated by underlying bowel disease, abscesses of the seminal vesicles, or hip infections. Early recognition of the origin of inguinal abscesses would facilitate planning of their surgical treatment so as to avoid catastrophic consequences. The differential diagnosis of inguinal abscesses includes appendicitis, cecal adenocarcinoma, infections in the hip, abscesses of the seminal vesicles, abscesses related to intravenous (IV) drug abuse, aneurysms of the femoral or iliac arteries, and lymphoma, among other pathologies [8–24]. Although the need for a carefully recorded history and physical examination cannot be overemphasized in the diagnosis of inguinal abscesses, the use of advanced imaging as a diagnostic adjunct has been suggested [16] We conducted a comprehensive review of inguinal abscesses presenting as deep, complex soft-tissue infections or intra-abdominal pathology. It is hoped that such diseases will not be overlooked and can be treated on basis of their pathophysiology.
Patients and Methods
A comprehensive review in the PUBMED data base of the English language literature on inguinal/groin abscess treated surgically was conducted with use of the Mesh terms “groin,” “inguinal,” and “abscess.” One hundred seventy-nine reports were identified and reviewed carefully. The inclusion criteria were descriptions of patients who presented a groin mass or inguinal mass of varied pathogenesis and requiring surgical intervention. Twenty-seven reports from the PUBMED data base, describing 30 patients, were included. The investigation also included three patients treated at our hospital who met the inclusion criteria. The clinical parameters collected and analyzed in the review included age, gender, laterality of involvement, causal hypothesis, and diagnostic modality, as well as the bacterial species recovered from cultures. Three patients with abscesses of different origins and involving the inguinal region were also included to illustrate the important findings on imaging and the clinical course of inguinal abscesses of diverse origin.
Results
Review of the demographic and clinical parameters collected for the 33 patients included in the investigation (Table 1) revealed a bimodal distribution in their age, toward infants or adults >40 years of age, except in patients involving IV drug abuse–related abscesses. All patients (100%) with inguinal abscesses presented with a swollen, erythematous, and tender inguinal mass. Most patients (64%) experienced a gradual onset of disease marked by a limping gait, fever, and chills. Laboratory tests usually (70%) revealed leukocytosis. Inguinal abscess and the extent of infection were evaluated with computed tomography (CT) in 60% of patients (Table 2). Upon diagnosis, the treatment of an inguinal abscess included broad-spectrum antibiotic therapy, aggressive resuscitation, and adequate debridement guided by CT or another imaging modality. A diverse etiology of inguinal abscess was noted in the 33 patients included in the investigation, who were divided into five groups based on the origin of their infection as: gastrointestinal, retroperitoneal, genitourinary, IV drug–related, and miscellaneous.
IV=intravenous; LAR – low anterior resection; THA=total hip arthroplasty.
Report=patients in the present series.
CT=computed tomography; MRI=magnetic resonance imaging.
The inguinal masses occurred predominantly on right side in the group with a gastrointestinal origin of infection, which included eight patients with cecal and appendiceal pathologies. Fever and leukocytosis were present in all five of the groups established according to origin of infection. The CT findings in patients with inguinal abscesses included asymmetric enlargement of the underlying affected muscle, a “ring sign” or rim enhancement of the abscess wall with lower central attenuation, and gas bubbles. Computed tomography was sensitive in elucidating the extent of infection in all five of the groups in the investigation. Magnetic resonance imaging (MRI) was used in two patients in the group with a retroperitoneal origin of infection. Microbial culture demonstrated a predominance of gram-negative pathogens in abscesses of gastrointestinal and genitourinary origin, whereas gram-positive pathogens were prevalent in IV drug-related abscesses and infections involving the joints and foreign bodies. Monomicrobial infections were demonstrated in abscesses of gastrointentinal, genitourinary, and retroperitoneal origin, whereas polymicrobial infections occurred in IV drug-related abscesses (Table 3). All patients underwent surgical intervention that accorded with the pathology of their abscesses.
Abscesses related to intravenous drug abuse in four patients were polymicrobial.
Case Reports
Patient 1
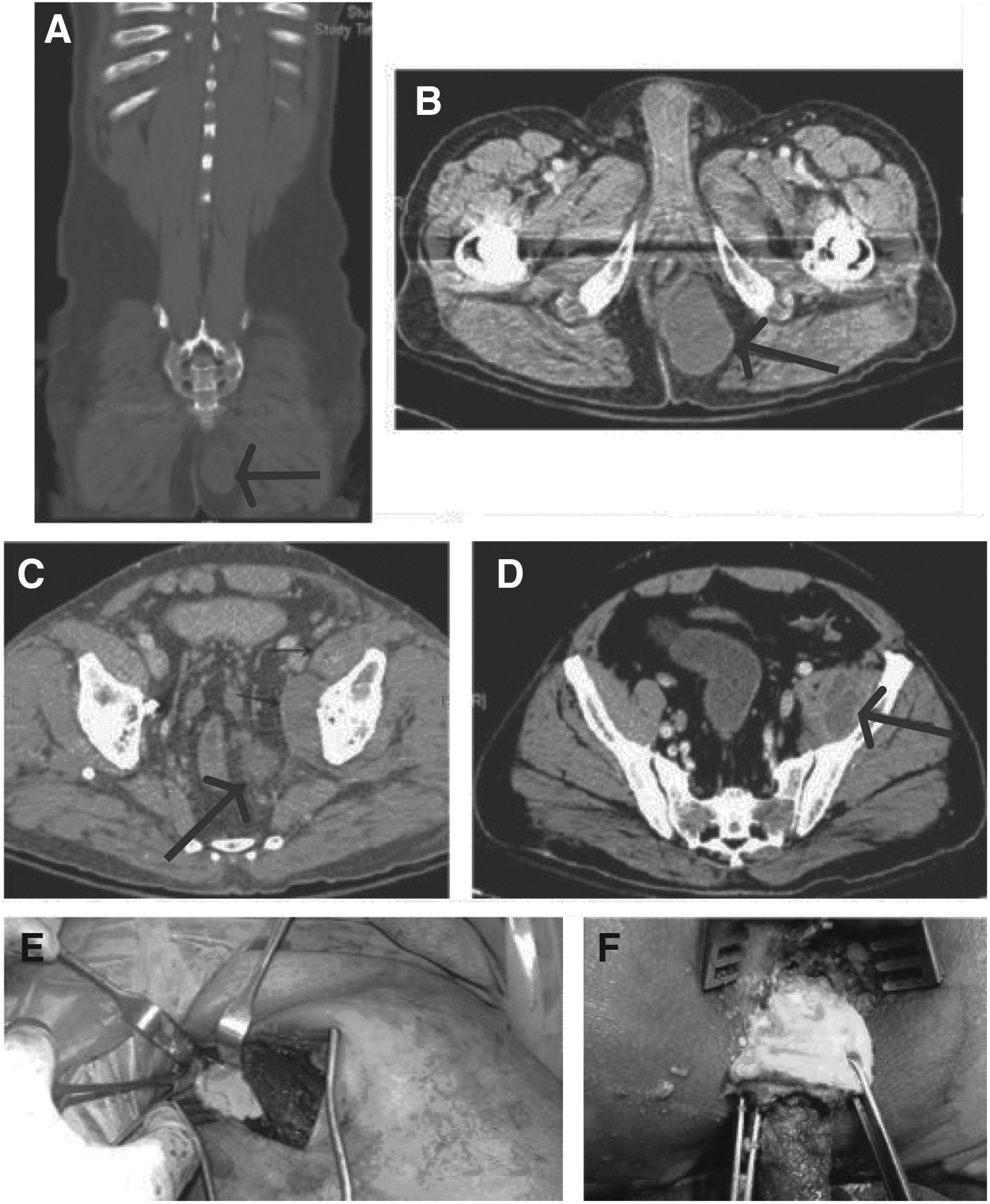
A 53-year-old female presented initially to our institution with pain in her right hip and a limping gait 1 mo before admission. A flexion–abduction–external rotation test of the patient's right hip elicited pain, but no fever, chills, or systemic symptoms were noted at that time. The patient was later sent to the emergency department (ED) with a swollen, erythematous, and tender inguinal mass of 3-d duration together with a spiking fever (Fig. 1A). She kept her right hip in slight flexion because forceful extension exacerbated her pain. She had no history of underlying bowel disease, immunodeficiency, diabetes mellitus, or IV drug abuse. Laboratory studies showed a white blood cell (WBC) count of 23.6×109/L, with 4.0% band forms, and an erythrocyte sedimentation rate (ESR) of 63 mm/h. The patient was immediately given oxacillin and gentamicin. Computed tomography of the pelvis showed an amorphous fluid collection with gas bubbles proximal to the right iliopsoas muscle and distal to the adductor muscle of the right inguinal region (Figs. 1B and C). The patient underwent surgical debridement with open drainage within 24 h of her admission because of rapidly developing sepsis. Debridement was done of the inguinal abscess together with curettage of the abscess overlying the iliopsoas fascia and deep into the retroperitoneal space (Figs. 1C and D). Frank pus and necrotizing tissue were collected for bacterial culture that yielded Bacteroides fragilis. The patient recovered after completing 14 d of IV metronidazole and was discharged uneventfully.

Patient 2
A 52-year-old male presented with a left inguinal mass associated with dull pain in the left buttock of 1-mo duration. On examination in the ED he was noted to have fever and chills. Examination revealed both an erythematous, swollen, and tender mass over the left inguinal region and diffuse swelling and tenderness in the left buttock. The patient had hepatitis C and alcoholism. He had undergone a bilateral total hip arthroplasty (THA) because of avascular necrosis of the heads of both of his femurs. Laboratory studies showed leukocytopenia (WBC count, 4.0×109/L), an elevated C-reactive protein (CRP) (76.3 mg/L), and an increased ESR (121 mm/h). Pelvic radiography showed no evidence of loosening or misalignment of the patient's implant. Magnetic resonance imaging of the pelvis demonstrated large, complex, multi-lobulated abscesses with lower central attenuation and peripheral enhancement, extending from the left ischiorectal fossa to the left iliacus muscle, iliopsoas muscle, and adductor muscle (Figs. 2A–D). Debridement was done of the multiple abscesses in the left iliacus muscle, left iliopsoas muscle, and adductor muscle, using a Smith-Petersen approach (Fig. 2E). Concurrently, a perineal incision was made for debridement and drainage of the left ischiorectal abscess (Fig. 2F). Intravenous antibiotic therapy with ceftriaxone plus metronidazole was given on the basis of the antibiotic susceptibilities of the bacteria isolated from the patient's abscesses (Escherichia coli and B. fragilis). The postoperative catheter drain for the patient's left ischiorectal abscess was removed after 14 d when its output was minimal and non-purulent. The patient recovered uneventfully and was discharged after 4 wks of parenteral antibiotic therapy.
Patient 3
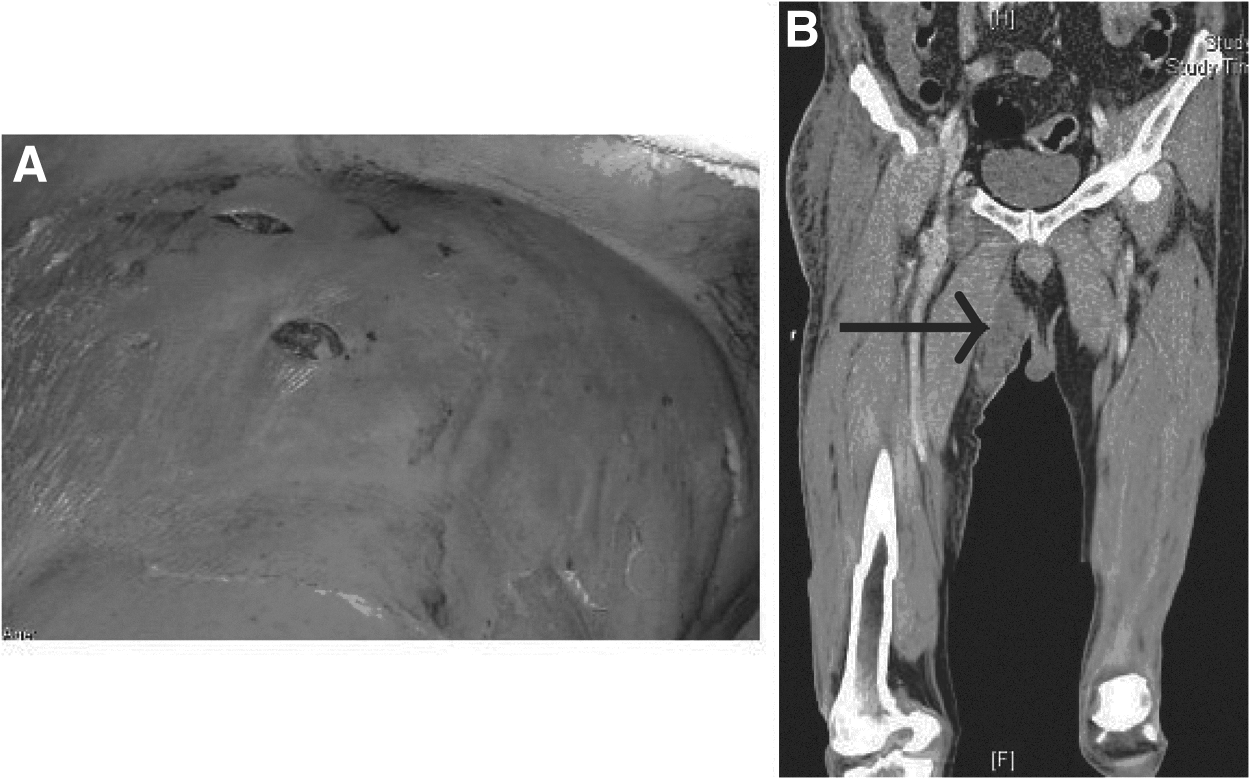
A 54-year-old male with an underlying hepatitis C infection and diabetes mellitus experienced a painful swollen inguinal mass forcing him to walk with a limping gait for 2 d before admission (Fig. 3A). He presented with fever, tachycardia, and lethargy. A bulging, erythematous, and painful mass was found in his right inguinal region. Laboratory examination revealed leukocytosis with a shift to the left (WBC count, 20.9×109/L, 5% band forms) and an elevated CRP concentration (274.0 mg/L). Radiographs of the patient's pelvic area and right hip were normal. Computed tomography of the pelvic area and right thigh showed formation of an abscess with gas bubbles in the medial region of the right thigh and involving the underlying adductor muscle groups (Fig. 3B). The patient was given oxacillin and subsequently underwent fasciotomy and extensive debridement because of profound sepsis. Drainage and debridement in the deep fascia and underlying adductor muscle group yielded about 300 mL of frank pus. Microbiologic examination of the wound culture revealed oxacillin-sensitive Staphylococcus aureus. The patient recovered uneventfully and was discharged after 4 wks of parenteral antibiotic treatment with vancomycin.
Discussion
The investigation described here found that patients with inguinal abscesses had diverse pathogenic findings, clinical presentations, and corresponding surgical interventions. Although two patients may have similar painful erythematous indurations in the inguinal region, the mechanisms of the two lesions may be quite different. The inguinal region communicates with the peritoneal and retroperitoneal spaces and the thigh through several routes, including the psoas sheath, femoral canal, sacrosciatic notch, pudendal canal, and obturator foramen [25,26] (Fig. 4). Indeed, retroperitoneal infections or the perforation of affected bowel may contribute to an inguinal abscess by way of the psoas sheath, which was also found to serve as a route of infection in adductor pyomyositis and infected THA.
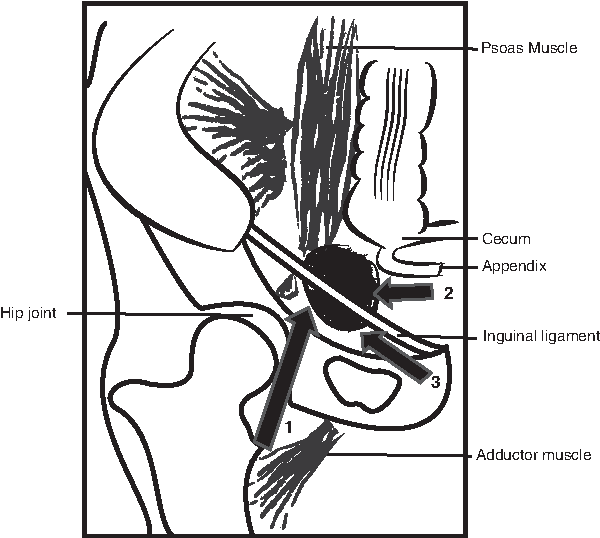
Routes leading to the formation of inguinal abscesses, including extension from the retroperitoneal region or hip joint along the psoas muscle (arrow 1); local extension from a gastrointestinal source (arrow 2); and extension from the genitourinary region along the inguinal canal (arrow 3). 195×171 mm (300×300 DPI)
Through this comprehensive review, it was found that inguinal abscesses may arise from intra-peritoneal or retroperitoneal abscesses, as well as by extension from pelvic bone or the thigh muscle compartment. Failure to identify the etiology of an inguinal abscess may result in its inadequate treatment. Computed tomography provided timely and accurate information that helped guide the empiric antibiotic treatment of and surgical planning for the management of inguinal abscesses. The treatment of deep soft-tissue abscesses in the inguinal area should be based on their pathology. Open drainage permits adequate debridement of the adjacent tissue in abscesses other than those of gastrointestinal origin [27–29]. In ruptured appendicitis and cecal adenocarcinoma, appendectomy and right hemicolectomy was suggested [10,11,14,15,18,20,22,24,30,31].
Computed tomography is helpful in diagnosing inguinal abscess and determining the extent of infection. In patients presenting with inguinal abscess, early recognition of its origin can facilitate surgical planning for its treatment and possibly improve the patient's outcome.
Footnotes
Author Disclosure Statement
No financial support was received for this study, and the authors have no conflicts of interest to declare.