
Abstract

To the Editor:
A 53-year-old man with no notable medical history presented to the emergency department with a one-week history of increasing right-sided abdominal and flank pain radiating to the right thigh, aggravated by walking and associated with limitation of right hip movement; a low-grade fever for the past two days also was reported. On physical examination, he was febrile (38.6°C), but hemodynamically stable, reporting right-sided pain during abdominal palpation, without guarding. Additionally, the patient was noted to have an antalgic groin and to maintain an antalgic posture, characterized by flexion of the right lower limb; no neurologic deficits were observed in the lower extremities. Laboratory studies revealed a white blood cell count of 14.6×109/L and C-reactive protein concentration of 3.5 mg/dL; the remaining blood studies were unremarkable.
A CT scan of abdomen and pelvis showed enlargement of the right iliopsoas muscle associated with a 16.0×3.0-cm low-attenuation lesion exhibiting an air-fluid interface and rim enhancement after intravenous administration of contrast (Fig. 1). In this clinical setting, imaging findings were consistent with a right-sided IPA. In the multiplanar reconstructions, a linear and well-delimited low-attenuation object was depicted, extending from the interior of the duodenum and reaching the right iliopsoas collection (Fig. 2). A hypothesis was made of duodenal perforation by a FB causing an IPA.
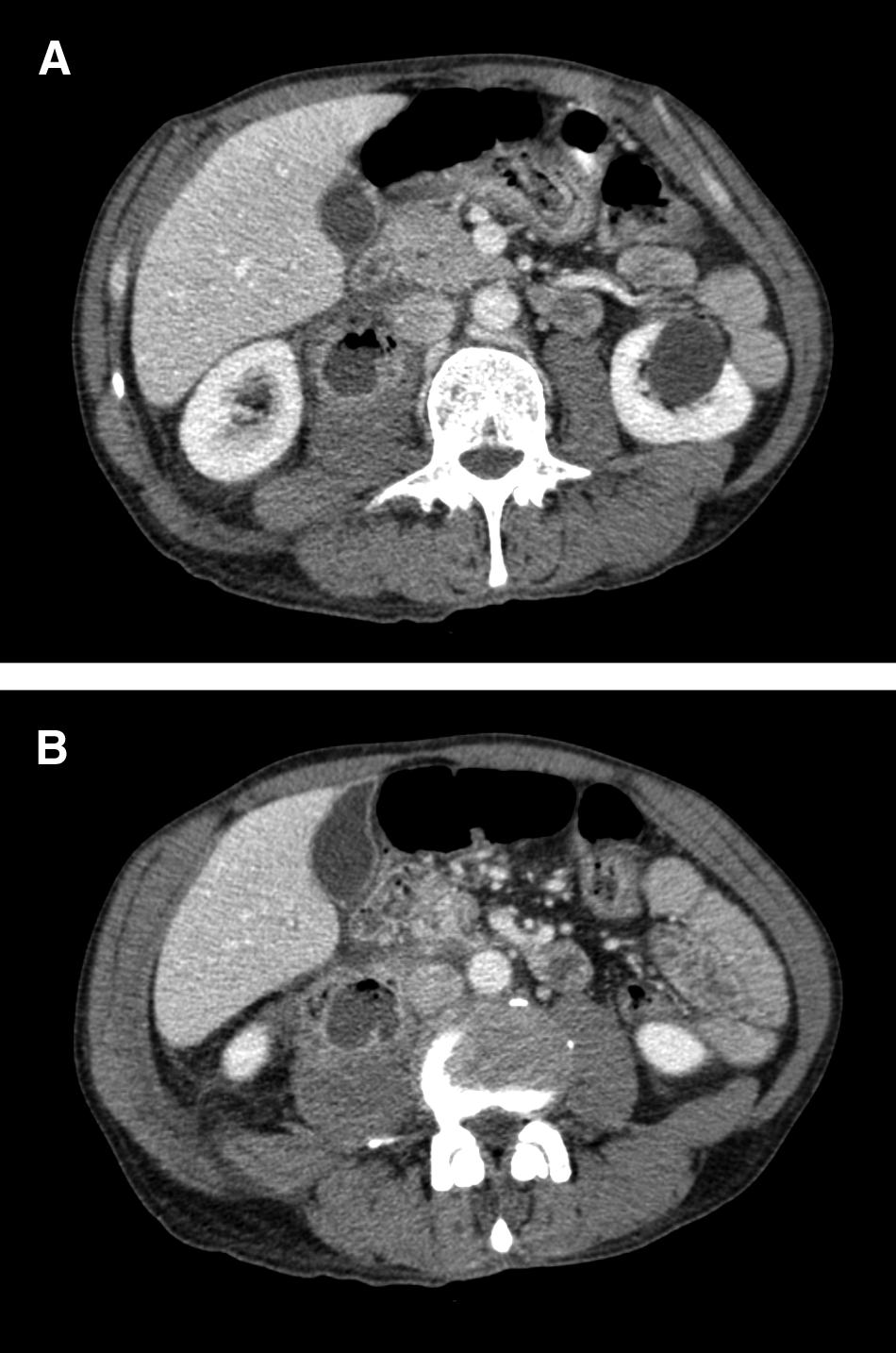
Axial contrast-enhanced computed tomography scan through abdomen at two levels (

Oblique sagittal contrast-enhanced reformatted images (
Empiric antibiotic therapy with metronidazole and ceftriaxone was initiated, and the patient underwent laparotomy the next day to drain the abscess and remove the FB. Intra-operative findings confirmed the pre-operative hypothesis and revealed a wooden toothpick perforating the duodenum and extending into the right iliopsoas muscle with purulent collection (Fig. 3). Cultures of this material yielded Enterococcus faecalis (sensitive to penicillin, ampicilin, streptomycin, gentamicin, teicoplanin, vancomycin, and linezolid; resistant to ciprofloxacin), after which the antimicrobial regimen was switched to ampicillin-sulbactam. Postoperative recovery was uneventful, and the patient was discharged asymptomatically, without any complaints on routine outpatient follow-up.
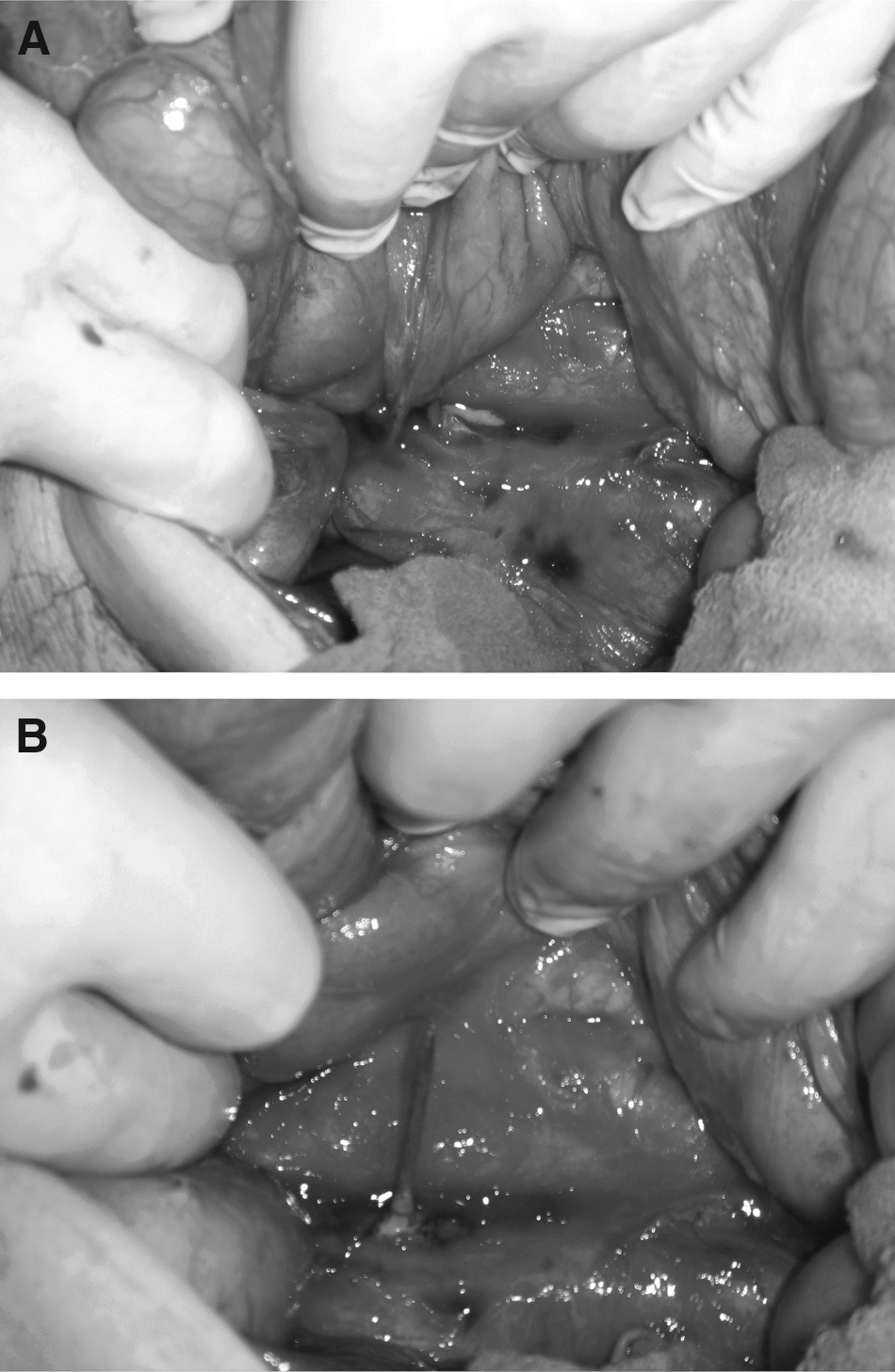
Intraoperative findings (
Iliopsoas abscesses can be classified as primary or secondary according to their etiology; whereas primary IPAs are rarer and usually idiopathic, affecting especially immunocompromised patients [1], secondary abscesses are more common and may be consequent to direct spread from infections of adjacent organs, such as the small and large bowel, kidneys and urinary tract, spine, and aorta [2]. An IPA secondary to a duodenal perforation by an FB is exceedingly rare, and, to the best of our knowledge, there is no report of imaging-based diagnosis in this setting.
Bowel perforations consequent to unintentional FB ingestion are difficult to diagnose pre-operatively [3] as a result of the low degree of clinical suspicion, the unavailability of a history of FB ingestion, and the lack of specificity of the clinical manifestations [4]. Therefore, the diagnosis is made commonly during laparotomy [3]. In our case, the IPA induced careful examination of the adjacent structures for an etiology that facilitated the diagnosis.
Multi-detector CT is an effective method for the evaluation of intestinal perforation caused by ingestion of a FB [5], as it enables high-quality multi-planar reconstructions with thin collimation and high resolution. Therefore, the gut can be assessed in all projections, and whatever the spatial orientation, a FB can be identified [5]. Although these affirmations generally are valid for calcified FBs [5], our case presented an additional difficulty, as the FB was a wooden toothpick and, therefore, appeared as a low-attenuation image on the MDCT scan.
Treatment of IPA consists of antibiotic therapy and open or percutaneous drainage, the latter having replaced surgical drainage as the method of choice. However, in patients such as ours, with suspicion of an underlying surgical gastrointestinal tract cause such as duodenal perforation, operative management is required. In addition, both the empiric and culture-driven antimicrobial therapy adopted in our case followed current international guidelines for the management of intra-abdominal infections of adults [6].
Footnotes
Author Disclosure Statement
The authors declare no conflicts of interest.