
Abstract
Abstract
Background:
Appropriate utilization of antibiotics for critically ill patients involves tailoring the drug to culture results; however, the culture results must be reliable. We hypothesized that antimicrobial agents reduce significantly the reliability of cultures obtained between 1 and 24 h after antibiotic administration.
Methods:
Patients were eligible for the study if they were ventilated mechanically and were suspected to have pneumonia. After enrollment, sputum cultures were obtained, and broad-spectrum antibiotics were started. Sputum cultures were repeated at 1, 6, 12, and 24 h after delivery of the first dose of antibiotic. Twenty-one patients whose initial culture was positive were included in the analysis. Their average age was 49.4 years, and the average Injury Severity Score was 27.7 points.
Results:
The average intensive care unit and hospital lengths of stay were 20.2 days and 24.7 days, respectively. All of the organisms grown from the pre-antibiotic cultures also grew in the cultures obtained 1 h after antibiotics were given. However, a significant number of these organisms were unable to be grown in subsequent cultures. The rate of negative cultures increased to 21%, 32%, and 42% in the 6-, 12-, and 24-h groups (p<0.01), respectively. Gram-positive organisms accounted for 42.9% of infections, with Staphylococcus aureus being the most common. All patients positive for S. aureus prior to antibiotic administration remained positive at each subsequent time. By 6 h, 21.5% of the gram-negative organisms could no longer be cultured. At 12 h, among the gram-positive organisms, 11 of 12 cultures were still positive, whereas only 50% of gram-negative organisms were still recoverable.
Conclusion:
Antibiotics have a substantial effect on culture results that is most pronounced in gram-negative organisms and is observed in cultures obtained beginning 1 h after antibiotics are given. As a result, cultures obtained more than 1 h after antibiotics are started cannot be used to tailor antibiotic choice in injured patients with suspected infections.
The optimal approach to the treatment of infections in the ICU must consider two competing principles [4]. Inadequate antibiotic therapy, defined by post-hoc sensitivity profiles, is associated with increases in the mortality rate [5]. Similarly, delayed introduction of antimicrobial therapy is associated with a higher risk of death [6]. These principles have led physicians to prescribe broad-spectrum antibiotics empirically when severe infections are suspected. However, there are undesirable consequences to this approach. First, broad-spectrum antibiotics may increase the incidence of certain super-infections, such as pseudomembranous colitis [7]. Additionally, “antibiotic pressure” is the primary driving force behind antibiotic resistance, both in individual patients and within ICUs [8].
In order to reconcile these competing principles, de-escalation therapy was developed. With this approach, broad-spectrum antibiotics are initiated empirically and tailored within three days to the organism(s) found in the culture. In order for de-escalation therapy to be implemented, however, physicians must feel confident about the culture results. For this reason, multiple guidelines have recommended obtaining cultures prior to the administration of antibiotics [3,4]. In the event patients receive antibiotics prior to cultures being obtained, there is little literature to guide physicians about the appropriate approach. It is intuitive that pre-culture antibiotics would inhibit the growth of bacteria in the microbiology laboratory provided they are sensitive to those drugs; however, the specific details of this effect are unknown. For example, it is not known how quickly pre-culture antibiotics invalidate culture results and how antibiotics affect cultures obtained from trauma patients. Injured patients tend to be younger and also to have a metabolic profile different from medical patients because of their multi-system injuries. This characteristic also could affect the results of cultures obtained after antibiotic administration. We designed a study with the following objectives: (1) To evaluate the effect of pre-culture antibiotic administration on culture results at various time points thereafter; and (2) to evaluate the differential effects of pre-culture antibiotic administration on the organism recovered.
Patients and Methods
Permission to perform the study was granted by our Institutional Review Board. Informed consent was obtained from each patient's surrogate decision maker, as the patients were not able to provide consent for themselves.
North Memorial Medical Center is an American College of Surgeons-verified Level I trauma center. The study was conducted over a 15-month period from 2009 to 2010. Patients admitted to the trauma service who were intubated endotracheally and who were suspected of having pneumonia were approached for enrollment. The trauma service is staffed primarily by four surgeons. To diagnose VAP, cultures are obtained when fever or leukocytosis is noted in combination with purulent secretions or chest radiograph infiltrates. It is our practice always to start empiric antibiotics, although the specific regimen is left to the discretion of the attending trauma surgeon. We de-escalate when final culture results become available. We typically treat VAP for 7 days (or 14 days for Pseudomonas infections).
Patients were considered appropriate for the study if the attending physician planned to obtain sputum cultures and start broad-spectrum antibiotics. Patients who were under 18 years of age or who received antibiotics in the preceding 24 h were excluded. Twenty-one patients were enrolled. Baseline cultures were obtained, and sputum cultures were repeated 1, 6, 12, and 24 h after antibiotic administration began.
Empiric antibiotic regimens generally consisted of broad-spectrum coverage with piperacillin-tazobactam or meropenem with or without vancomycin. Six of the patients were treated with meropenem, and 12 were treated with piperacillin-tazobactam. The remaining three patients received ciprofloxacin, ceftriaxone, and tigecycline. Thirteen of these patients also received vancomycin for empiric methicillin-resistant Staphylococcus aureus (MRSA) coverage. None of the cultures was positive for MRSA. Among the patients with methicillin-sensitive S. aureus (MSSA), four received vancomycin. All but two of the patients with MSSA also received meropenem or piperacillin-tazobactam. The remaining two patients received ceftriaxone or tigecycline.
Sputum cultures
Sputum cultures were obtained via tracheal aspiration by the ICU nursing staff, as is our standard practice. Both semi-quantitative and quantitative tests were conducted on each specimen. Semi-quantitative results were reported as no, scant, light, moderate, or heavy growth. Quantitative cultures were reported as the number of colony-forming units (CFU)/mL. Laboratory testing was conducted according to Clinical Laboratory Improvement Amendments (CLIA) standards. Only patients with a positive sputum culture were enrolled.
Data analysis
Statistical analysis was conducted with Analyse-It (Analyse-it Software, Leeds, United Kingdom). Semi-quantitative cultures were treated as categorical data and analyzed with chi-square tests for multiple-group companions. Quantitative cultures were treated as both categorical and continuous variables. The average quantitative result at each time point was compared with the baseline using paired t-tests. This analysis was used instead of analysis of variance, as the only data of interest were the numbers of organisms at each time compared with the number at baseline. The quantitative culture results were then stratified as being above or below a threshold of 104 CFU/mL. The number of “positive” samples using this threshold at each time point was then calculated, and the number at each time was compared with the baseline number using chi-square tests. The log10 reduction was calculated by taking the logarithm of the quotient:individual time point CFU/mL divided by the baseline CFU/mL. Because a quotient cannot be created when dividing by zero, a value of 1 was substituted when “no growth” was reported.
Results
Two organisms were cultured from seven patients, so the total number of bacterial isolates evaluated was 28. Demographic information of the 21 patients is listed in Table 1. The average patient age was 49.4 years. Most of the patients were male. The patients were severely injured, as indicated by an average Injury Severity Score of 27.7 points. One patient died. The average ventilator time was 17 days. The average time after admission that cultures were obtained was 8.9 days. All of the bacterial isolates grown in culture were sensitive to one of the antibiotics given empirically. Certain bacteria, such as Moraxella catarrhalis and Haemophilus influenzae, were tested only for beta-lactamase positivity rather than for specific antibiotics. Sensitivity profiles were extrapolated based on this testing and by assuming that MSSA was sensitive to piperacillin-tazobactam, meropenem, and vancomycin despite lack of formal testing against these agents.
Overall, 57% of the isolates were gram negative (Table 2). The most common was H. influenzae, which accounted for 18% of isolates. The remaining gram-negative organisms were split between H. parainfluenzae (n=3), M. catarrhalis (n=2), Escherichia coli (n=2), and six species that were isolated only once. The most common bacterial species isolated was S. aureus, which accounted for 36% of all isolates and 83% of the gram-positive isolates.
Organisms recovered once. These were Pseudomonas aeruginosa, Streptococcus pneumoniae, Acinetobacter baumannii, Citrobacter koseri, Streptococcus group C, and Enterobacter cloacae.
There was a significant effect of antibiotics on culture results (Fig. 1). All of the organisms that were cultured at baseline had some element of growth after 1 h of antibiotics. By the 6-h time point, however, 21.5% of the organisms could no longer be cultured. This was exclusively among the gram-negative bacteria. At 12 h, 32.1% of the these cultures were negative. Among the gram-positive organisms, 11 of 12 were still positive at 12 h, whereas only 50% of gram-negative organisms were still recoverable. By 24 h after the start of administration of antibiotics, 42.9% of the cultures were negative: 10 of 12 gram-positive organism cultures remained positive but only 37.5% of gram-negative organism cultures were still able to be cultured. Streptococci accounted for the gram-positive cultures with no growth at this time. All of the S. aureus cultured at baseline also were cultured at each subsequent time point.
Culture results at each time. Each cell represents percentage of cultures that were positive (i.e., not “no growth”) at that time. The p values are listed above each bar that is not 100% (where p=1) and represent the results of the chi-square tests that compared each time with the baseline.
The semi-quantitative culture results are shown in Figure 2. At baseline, the majority of cultures had either moderate or heavy growth. Over the next 24 h, there was a trend toward an increasing percentages of cultures with no or scant growth and a reduction in moderate and heavy growth. Seventy-five percent of the baseline cultures demonstrated either moderate or heavy growth. This trended down to 42% at 1 h (p=0.11). Only 4% of the cultures obtained at baseline showed scant growth. At 6 h, 42% of cultures showed no or scant growth (p=0.0035), at 12 h, 43% of cultures showed no or scant growth (p=0.0007), and by 24 h after the start of administration of antibiotics, 64% of the cultures showed no or scant growth (p<0.0001).

Percentage of cultures reported as having no, scant, light, moderate, or heavy growth at each time point. The p values represent the chi-square results that compared each followup culture with the baseline.
Quantitative cultures also were evaluated (Fig. 3). The baseline average bacterial count was 61.66×103. This decreased steadily over the next 24 h. The average quantitative culture at 1 h was 49.20×103 (p=0.0186 compared with baseline), which decreased to 10.41×103 by 24 h after the start of antibiotic administration (p<0.0001). The average log reduction at 1 h was 0.286. This increased to 0.577 at 6 h, 0.614 at 12 h, and 1.04 at 24 h. However, the average log reduction must be interpreted with caution, as there was a wide range. In one instance, there was a negative log reduction (increase in growth), and among the other cultures, the range of log reductions was 0 to 4.17. When stratifying for just the gram-negative organisms, the log reduction was more dramatic: 0.48 at 1 h, 2.1 at 6 h, 2.5 at 12 h, and 3.04 at 24 h.

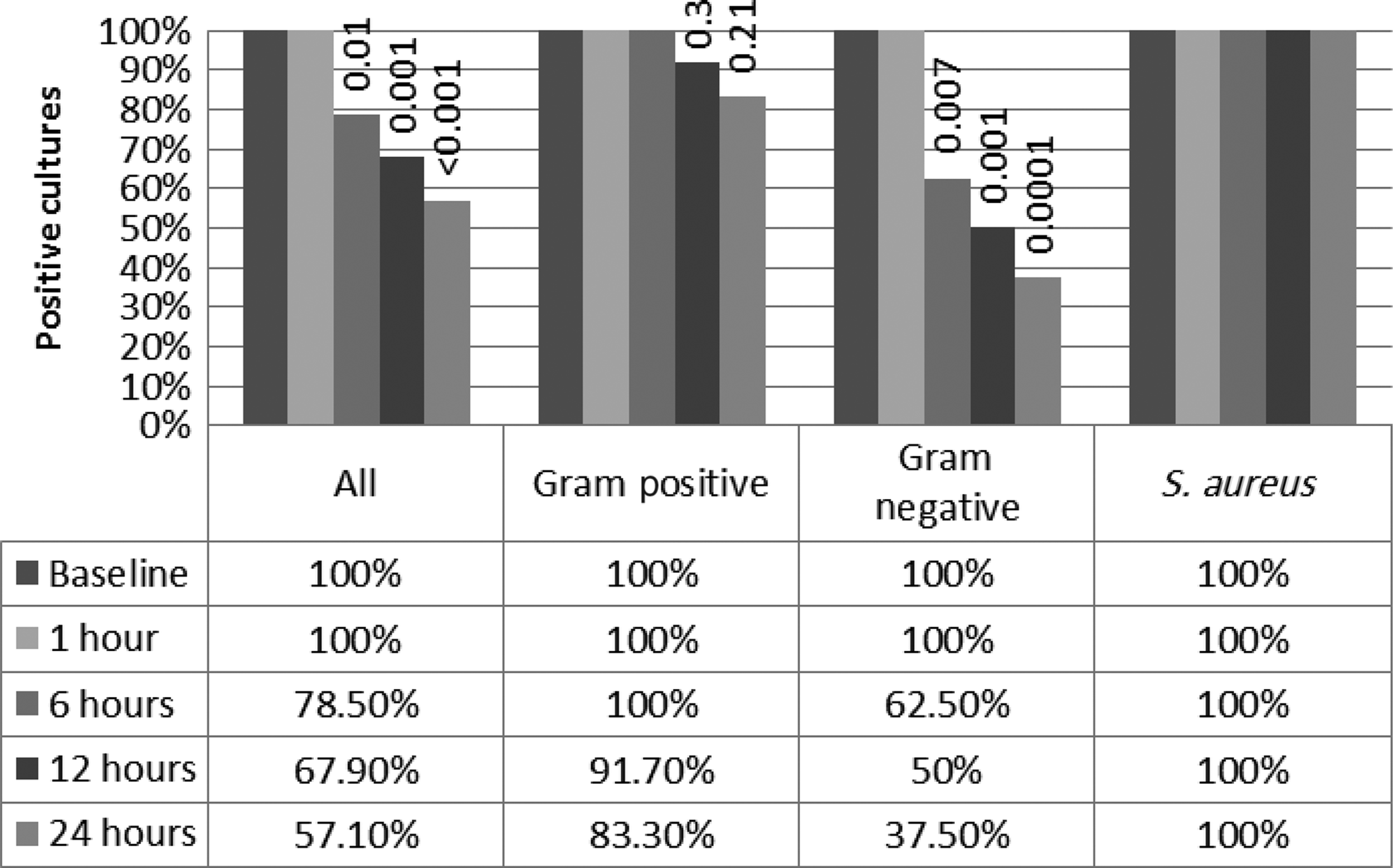
Percentage of quantitative cultures positive at each time point (>104 colony-forming units/mL). The p values (inside bars) represent each time compared with the baseline.
Quantitative cultures also were evaluated according to a threshold commonly used to diagnose VAP. Among the baseline cultures, 23 had growth that was at least 104. Gram-positive organisms accounted for 12 of these positive cultures. The percentage of cultures at subsequent time periods that met the threshold value of 104 was evaluated (Fig. 4). Of all the organisms, S. aureus was the most robust. All of the cultures of this organism met the threshold at 1 h, and only one sample at the 6 and 12 h did not reach the threshold. By 24 h, however, only 60% of the S. aureus cultures met the 104 threshold (p=0.02). About three-quarters of gram-negative organisms could still be cultured at 1 h, but only 18.2% were cultured at each subsequent time point (p<0.0001).
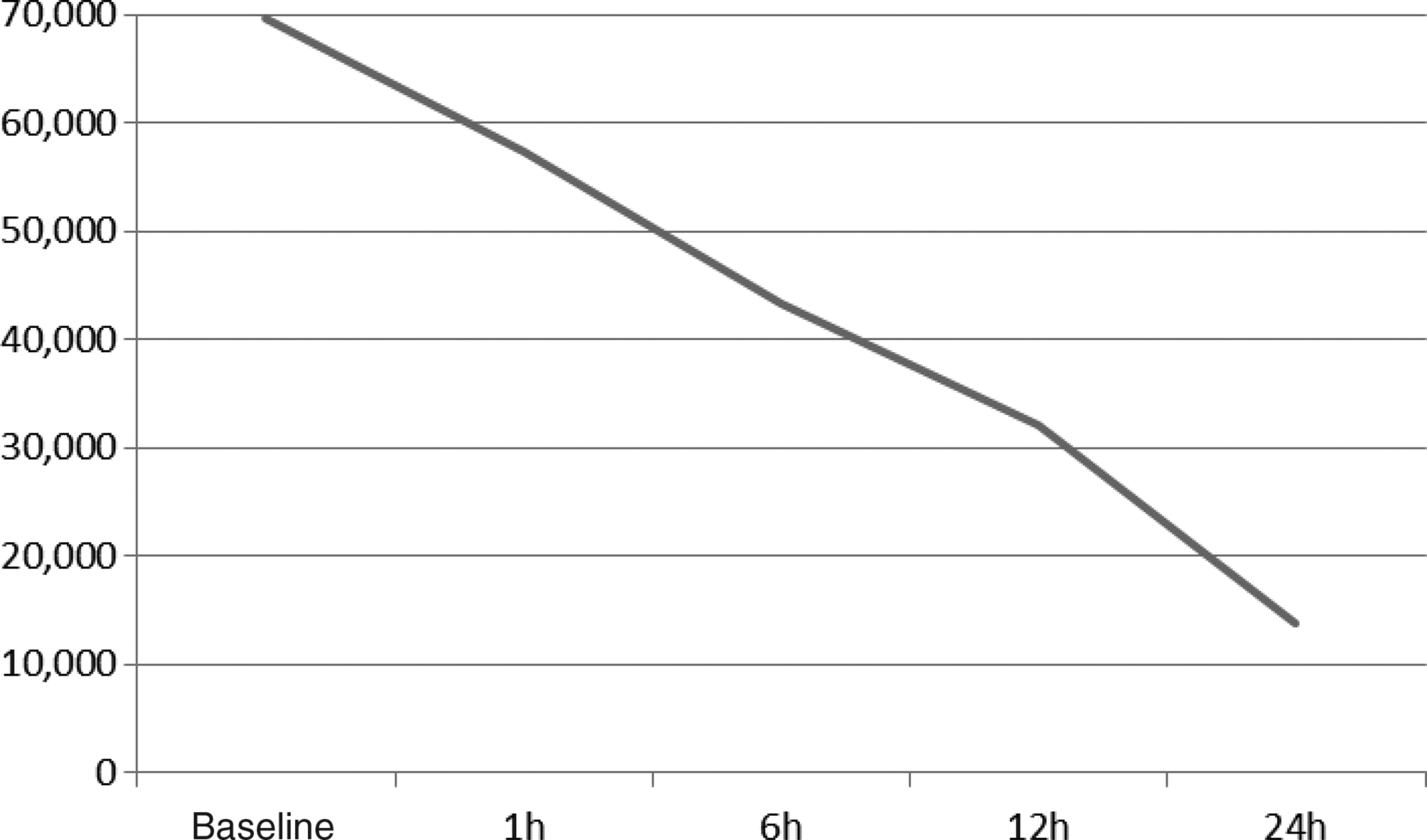
Average quantitative culture results at each time point. The y-axis represents the number of colony-forming units; the x-axis represents time after first antibiotic dose. The p values compared with baseline were 1 h, 0.019; 6 h, 0.0023; 12 h, <0.0001; 24 h, 0.0001.
Discussion
The traditional school of thought teaches that culture results obtained during antibiotic therapy are unreliable. As a result, clinicians may provide an entire course of broad-spectrum antibiotics without tailoring treatment to sensitivity analyses. This approach is problematic, in that it exposes patients to antibiotics that may not be necessary. Moreover, exposure to antibiotics is a factor in antibiotic resistance and the development of certain infections, such as fungal superinfections and pseudomembranous colitis. Accordingly, the specific effect of antibiotics on culture results is important for clinicians to know.
The effect of antibiotics on quantitative cultures from protected brush specimens was evaluated by Prats et al. [9]. This study was conducted in a general ICU, but 10% of the patients had multisystem trauma, allowing comparison with our population. Cultures from brush specimens were obtained 12, 24, 48, and 72 h after the baseline culture. The investigators defined a positive culture as at least 103 CFU/mL. They noted that the rate of positive cultures decreased to 50% by 12 h and 4% by 72 h. Our study adds to this report in a number of ways. We also evaluated beginning soon after the administration of antibiotics. We found that gram-negative organisms are affected by antibiotic administration within 1 h of the first dose. The primary antibiotic used in the earlier study was amoxicillin-clavulanic acid, which is seldom used today for VAP. Also, although a protected brush specimen is a proved method of diagnosing VAP, tracheal aspirates from endotracheal tubes or bronchoalveolar lavages are more common in current practice. Our study has the advantage of using a diagnostic technique more popular in ICUs today.
A variety of other studies have suggested that antibiotics reduce the reliability of sputum culture results. Montravers et al. noted that most bacteria are eliminated with three days of the start of antibiotics [10]. Postmortem examinations also have suggested this result [11]. Dotson et al. demonstrated reduced ability to recover intracellular organisms among patients with recent antibiotic exposure [12].
Our study adds several important points to the research currently available. We focused exclusively on a trauma population, which increases the generalizability of our results to injured patients. We did not have enough samples to evaluate all organisms, but a clear trend was seen in S. aureus. This species was the most resistant to suppression by antibiotics. In fact, every patient who yielded S. aureus at baseline was positive for S. aureus at 24 h. The effect of antibiotics on gram-negative organisms was much more profound. A small minority of gram-negative organisms was still able to be cultured at 24 h, but a significant effect was seen already at 1 h. We did not have a large enough sample to determine if gram-negative bacteria traditionally considered to be more robust, such as Pseudomonas aeruginosa, would follow a trend similar to that seen with S. aureus.
The second item that our study adds to the current literature is the focus on shorter time frames. Although previous studies suggested that antibiotics affect culture results, these studies focused on times of at least 24 h. Our study has demonstrated that there is an early effect of antibiotics on culture results, within 1 h of antibiotic administration. This is an important point, in that physicians should not tailor antibiotics to culture results even if the cultures were obtained a short time after antibiotics were administered. The possible exception to that recommendation is S. aureus. If clinicians are simply looking at positive versus negative cultures, then the results of S. aureus sputum cultures appear to be reliable as late as 24 h after the start of antibiotic administration.
A third important point to our study was the presentation of results from both semi-quantitative and quantitative cultures. Guidelines on the diagnosis of VAP suggest that either type of culture is acceptable [3]; however, the interpretation of semi-quantitative cultures can be difficult. We included these data, as this is the primary type of culture obtained in many hospitals. Our data suggest that moderate or heavy growth is unlikely to be seen by 24 h after the beginning of antibiotic administration. We also demonstrated a clear reduction in quantitative cultures over the course of 24 h. The log10 reduction appears to be linear over time. Unfortunately, a specific change in the threshold for the diagnosis of VAP cannot be recommended from our results, as a number of cultures had no growth within 6 h of antibiotic dosing.
We cannot comment on the possibility of the development of a new bacterial steady state at some point after antibiotics are started. It is possible that after a few days of antibiotic administration, new cultures will be positive for organisms resistant to the antibiotic regimen being used. Our study was limited to 24 h, so we can comment only on this period.
There are limitations to our study. We included patients who did not meet the quantitative culture threshold for VAP (104 CFU/mL). We made this decision, as many hospitals do not perform quantitative cultures, and elimination of these samples would have reduced our sample size of semi-quantitative cultures. We used a tracheal aspirate as the primary method of culture. Therefore, it is not clear how our results apply to the practice of bronchoalveolar lavage. Previous literature has demonstrated that the ICU mortality rate is unchanged with either diagnostic approach [13]. We focused exclusively on trauma patients, which increases the generalizability of our results to this population but may reduce their applicability to other populations. We are limited in our ability to comment on specific bacteria, as the numbers of bacteria other than S. aureus were small. This study was designed as an observational study without a control group. As such, we cannot rule out the possibility that the same changes in culture results would have been observed in patients not given antibiotics. In our practice setting, however, this study design would have been impossible. It is our practice to start antibiotics while awaiting culture results, so we could not have justified a true control group ethically. Qualitatively, we noted that many patients were not eligible because they had received antibiotics in the previous 24 h, but we do not have data on their number. At our institution, many patients receive therapeutic courses of antibiotics for facial and open extremity fractures, although there is no formal policy on antibiotic use for these conditions. Additionally, many patients receive a single dose of antibiotics for procedures and operations. As a result, many patients (although the number is unspecified) were excluded from the study.
It is unlikely that the persistent growth of S. aureus in the face of empiric antibiotics was attributable to inadequate antibiotic coverage. Vancomycin achieves poor pulmonary penetration and is a suboptimal choice for MSSA; however, each patient with MSSA in the sputum also received a second agent that provides MSSA coverage for this organism. Our laboratory performs standard testing on S. aureus with cefazolin, clindamycin, erythromycin, levofloxacin, oxacillin, and penicillin according to CLIA standards. Organisms resistant to oxacillin are reported to be MRSA. All of the MSSA in this study were sensitive to all the antibiotics tested except penicillin. Because our laboratory does not perform formal testing on vancomycin, piperacillin-tazobactam, or meropenem, we extrapolated sensitivity to these drugs on the basis of the results with other antibiotics. It is possible (although unlikely) that the MSSA actually was resistant to these agents and that that is the explanation for the different response of S. aureus to empiric antibiotics. In order for our results to be incorrect, however, all 10 of the MSSA cultures would have had to have been resistant to meropenem, piperacillin-tazobactam, and tigecyline, which is unlikely.
Conclusion
Our results demonstrate clearly that there is a significant effect of antibiotics on culture results. This effect can be seen within 1 h of the start of antibiotic administration. Staphylococcus aureus appears to be robust, such that cultures of this organism appear reliable as long as 6–12 h after antibiotic administration, whereas other organisms begin to respond sooner. Thus, post-antibiotic culture results for bacteria other than S. aureus must be interpreted with caution.
Footnotes
Author Disclosure Statement
The authors have no commercial interests regarding any facet of this study.