
Abstract
Abstract
Background:
The World Health Organization has identified the rapidly growing prevalence of obesity as one of today's serious health problems. Various surgical interventions categorized collectively as bariatric surgery now play an ever-increasing important role as the only known effective treatment for severe obesity. Laparoscopic gastric bypass is currently the most frequent bariatric surgical procedure performed. However, the laparoscopic adjustable gastric band (LAGB) is rapidly gaining in popularity as a minimally invasive surgical option with anticipated similarly efficacious outcomes. Gastric band erosion following LAGB is an uncommon yet potentially serious complication unique to this form of weight loss surgery.
Methods:
Case report and literature review.
Results:
We report a case of a pyogenic liver abscess related to a LAGB procedure. Apropos to this case, we review the presumed pathophysiologic mechanism of this particular infectious process, and discuss this and other complications associated with LAGB operations.
Conclusions:
As LAGB bariatric procedures become more popular, clinicians need to be aware of uncommon, but potentially serious complications unique to this form of weight loss surgery.
Lifestyle and behavioral modifications have not proved to provide long-term success in weight reduction or alterations in those chronic co-morbid conditions associated with obesity [5]. Bariatric surgery (also referred to as weight loss or obesity surgery) is the best-established and most successful method for weight loss in the morbidly obese patient population [6]. In addition to the weight loss, a substantial number of morbidly obese patients with associated conditions such as diabetes mellitus, hyperlipidemia, hypertension, and obstructive sleep apnea that underwent a surgical bariatric procedure experienced complete resolution or improvement of these conditions [6].
Bariatric procedures achieve weight loss via a combination of restrictive and malabsorptive (metabolic) elements, both aimed at reducing caloric intake by modifying the anatomy of the gastrointestinal tract. Restrictive procedures lead to early satiety and reduced portion size, where a malabsorptive procedures reduce the small bowel length available for mixing of food and biliopancreatic juices, thus reducing calorie absorption. Throughout the past four decades, several bariatric operations have been introduced, ranging from primarily restrictive (vertical banded gastroplasty, laparoscopic adjustable gastric banding (LAGB), and sleeve gastrectomy) to combined restrictive/malabsorptive (Roux-en-Y gastric bypass, biliopancreatic diversion with duodenal switch) to purely malabsorptive, or metabolic, operations (duodenal switch, which also entails the removal of a small portion of stomach). However, due to the lack of any large randomized studies, no one procedure has been shown to be superior in maintaining weight loss, although, both the duodenal switch and Roux-en-Y gastric bypass are accepted as more effective for weight reduction [6].
The Roux-en-Y gastric bypass is currently the most frequently performed operation for treating morbid obesity, accounting for about 70% to 75% of all bariatric operations [7]. Approved for clinical use in the United States in June 2001, LAGB now represents approximately 20%–25% of all bariatric operations in the United States and has become the weight loss operations with the fastest rate of growth in recent years [8]. By choosing either of the two U.S. Food and Durg Administration (FDA)-approved bands (Lap-Band® [Allergan, Irvine, California] and Realize® [Ethicon Endosurgery, Cincinnati, Ohio]), the patient is offered a minimally invasive surgical option that does not require gastric transection or gastrointestinal reconstruction. The LAGB consists of the creation of a small gastric pouch proximal to a band made of silicone and a narrow stomal, which results in a decreased amount of food being able to pass through the distal stomach and into the duodenum. Adjustments in the volume of the newly-created gastric pouch can be made by altering the amount of saline in the band using a subcutaneous access port placed during surgery that connects directly to the band. Studies have proved LAGB to be an effective procedure for weight loss when compared with other restrictive and malabsorptive bariatric surgical procedures [9]. In addition to requiring less operative time (80 to 105 min) than that necessary for laparoscopic gastric bypass, attempted LAGB also has a low incidence of conversion to open laparotomy (<1%), a low mortality rate (zero to 0.5%), and the added benefit of being able to remove the band in an outpatient setting under sedation but without the need for anesthesia. More importantly, LAGB has a lower overall and major complication rate than Roux-en-Y gastric bypass [10]. Nonetheless, despite these attractive features, patients undergoing a LAGB obesity operation may develop post-operative complications unique to this surgical weight loss modality.
Complications of LAGB have been divided into intra-operative, early, and late problems. Intra-operative events include digestive perforation, liver injury, failure to place the band, and conversion to an open operation [11]. Early complications are defined as those occurring 6 mo after the surgery and include dilatation and early band slippage, and respiratory disorders (atelectasis, acute respiratory distress syndrome, and pulmonary embolism). Late complications appear 6 mo and beyond surgery and include late band slippage, band migration, or erosion and esophageal dilatation. Late band slippage and erosion are reported as the two main complications in this category.
Other reported peri-operative complications following LAGB include port leakage (<1%), port displacement (2.5%–6%), port infection (<1.8%), and pouch enlargement (12%) [8]. Along with slippage and erosion, other complications of clinical importance following LAGB include gastric or esophageal perforation or bleeding, stoma obstruction, food intolerance, late port or band infection, and intra-abdominal abscess formation.
Abdominal pain in the epigastric region, gastrointestinal bleeding, cessation of weight loss, local port access infection, and abdominal abscess either localized to the peri-gastric area or presenting with diffuse peritonitis are the most common presenting signs and symptoms of band erosion. We report a case of a solitary pyogenic liver abscess occurring a few weeks after a LAGB procedure, and propose suspected pathophysiologic events responsible for this unusual complication secondary to erosion of the band at its site of placement.
Case Presentation
A 35-year-old obese male with a BMI of 44 elected to undergo a LAGB operation. His standard pre-operative medical evaluation was unremarkable. Other than suffering from morbid obesity, he had no other past medical or surgical history. He was taken to the operating room where he was prepped and draped in the standard fashion for a LAGB. A left subcostal incision was made. A Veress® needle (Genicon, Winter Park, FL) was used to insufflate to 50 mm Hg pressure. Using a 5 mm Optiview® trocar (Ethicon Endo-Surgery, Cincinnati, OH), access to the abdomen was gained under direct visualization. Bladeless trocars were inserted: A 5-mm trocar high in the left upper quadrant, a 5-mm trocar in the subxiphoid area with a Nathanson® liver retractor (Mediflex Surgical Products, Islandia, NY), a 5-mm trocar in the upper midline, and a 15-mm trocar rostral to the umbilicus. The angle of His was found and dissected, the gastro-hepatic ligaments were opened, and a tunnel was dissected into the pars flaccida position behind the gastro-esophageal junction. The angle of His was entered from a posterior approach utilizing a 5-mm slotted blunt tip dissector. A Lap-Band APL system® (Allergan Inc., Irvine, CA) was placed into the abdomen and locked in place followed by the placement of two #0 Surgidac™ braided polyester sutures (Covidien, Mansfield, MA) between the fundus and body of stomach and the pouch above the band. The band was rotated nicely in the usual fashion. The orogastric tube was removed while cycling suction. The tubing was brought out via the 15-mm trocar site. The liver retractor was removed under direct visualization. The tubing was attached to the port with ease. The port was then secured to the anterior abdominal wall fascia using the Z® (Allergan, Inc., Irvine, CA). Finally, the skin was closed with absorbable suture and Dermabond® (Ethicon, Inc., Somerville, NJ).
The immediate post-operative course was uneventful and he was discharged home the next day after tolerating a clear diet, as per our protocol. His first clinic visit on post-operative day seven was unremarkable. However, approximately two weeks later, he presented to his primary care physician complaining of fever, chills, night sweats, and generalized malaise. He received empiric antimicrobial medications for a presumed viral and respiratory infection with no symptom improvement. Subsequently, on post-operative day 22, he was re-admitted to the hospital for evaluation of his prolonged fever, whereupon a computerized tomographic (CT) scan demonstrated a multi-loculated 14.2×13.0 cm lesion in the right lobe of his liver suggestive of an abscess (Fig. 1). Pertinent physical examination findings included an elevated temperature to 100.8°F, mild tachycardia, and a normal blood pressure. His abdomen was soft, non-distended, and without tenderness. Laboratory studies revealed a leukocytosis (white blood cell count of 11,500/mm3 on admission and 18,000/mm3 on hospital day 2) and abnormalities in the hepatic profile with elevations of alkaline phosphatase (154 units/L; normal 20–130), aspartate transaminase (144 units/L; normal 10–40), and alanine transaminase (165 units/L; normal 7–55). A percutaneous drain was placed under CT guidance into the suspected abscess, and a large quantity of purulent fluid was removed. The drainage tube was left in situ connected externally to a gravity-fed collection bag. Microbiologic analysis of the recovered fluid revealed the presence of several polymorphonuclear white blood cells along with gram-positive cocci in pairs and chains. However, no bacterial isolates were recovered upon culture of the fluid. Antimicrobial therapy with intravenous (IV) ceftriaxone and metronidazole was administered empirically.

Non-contrast computed tomography of the abdomen demonstrating an approximate 13 cm×14 cm single hepatic abscess.
An esophagogastroduodenoscopy (EGD) was performed, whereupon entering the stomach the gastric band could be seen dislodged and eroding into the gastric lumen (Fig. 2). The patient was taken back into surgery for laparoscopic removal of the gastric band, which was accomplished without complication (Fig. 3). An intra-operative EGD demonstrated complete removal of the band from the gastric lumen, and insufflation failed to demonstrate any evidence of visceral defect. He was tolerating a regular diet by post-operative day three. A four-week course of intravenous antimicrobial therapy was administered with eventual removal of the hepatic drainage catheter after resolution of the abscess. He has remained well clinically.
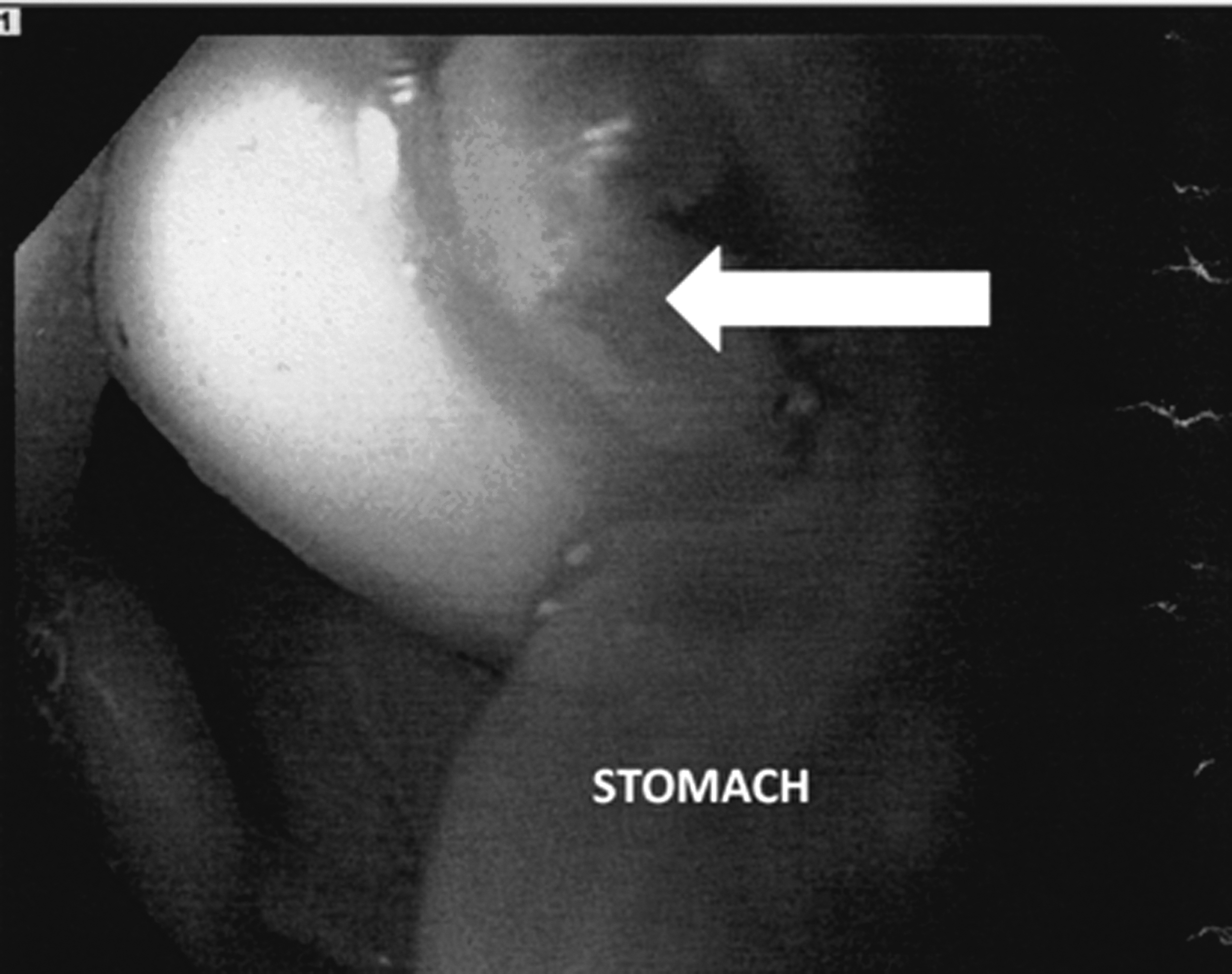
Esophagogastroduodenoscopic view of gastric band erosion into the stomach lumen.

Laparoscopic surgical removal of eroded gastric band from the stomach.
Discussion
The two major complications that can arise from bariatric operations that employ a banding procedure are gastric perforation and band migration [11]. Early perforations may result from a technical error during the operation or as a consequence of over-tightening of the band itself. Band erosion is defined as the gradual migration of the band through the stomach wall, and, on occasion, into the gastric lumen. Based on the time of diagnosis in relation to the surgery, band erosion complications are categorized as either early (within 1–6 mo post-operatively) or late [12]. In the vast majority of cases, band erosion occurs gradually and presents as a late complication of the bariatric procedure [8,13]. Overall, regardless of when the erosion takes place, the incidence of erosion following LAGB operations is reported to be less than 1%, with a prevalence varying from zero to 11% [11,13–14]. Interestingly, late erosions may not be due to the same mechanism as early erosions, and tend to be clinically silent and unrecognized [12]. It is postulated that erosion of the band begins with an inflammatory response provoked by placement of a foreign body (including silicone) around the stomach. Furthermore, the gastric wall insult induced by suturing the band to the stomach or imbricating the band with the stomach at the time of band placement alters the integrity of the gastric wall. Tight anterior fixation, especially around the band buckle, as well as increased pressure in the band, may result in necrosis of the gastric wall, thus facilitating erosion of the device [8,11]. Surgically provoked serosal damage that remains in contact with the silicone band has been proposed as a cause of intragastric migration of the band, as silicone itself is relatively inert to tissue [15].
Although the bacterial content in the upper gastrointestinal tract environment is generally sparse, infection around the foreign body nidus may result ultimately in rejection and extrusion of the foreign material [16]. Non-steroidal anti-inflammatory drug ingestion, alcohol consumption, and smoking also are predisposing factors contributing to disruption of the normal gastric mucosa [12,15].
In the majority of cases, patients with eroded bands are asymptomatic [8]. When symptomatic, the more common complaints related to band erosion are sudden cessation of weight loss, inability to fill the band properly, and acute or chronic infection at the port site [11]. Non-specific clinical manifestations also may include epigastric pain, gastrointestinal bleeding, intra-abdominal abscess, and systemic signs and symptoms of infection [8]. Peritonitis or the demonstration of pneumoperitoneum requires immediate attention [13]. Endoscopic evaluation is often used for definitive diagnosis [16]. Complete removal of the eroded gastric band endoscopically, laparoscopically, or via laparotomy is the recommended treatment for this LAGB complication [8,16]. In those patients exhibiting minimal symptoms, Chevallier et al. proposed delaying removal of the band until it has migrated completely through the gastric wall into the lumen, as this allows for removal of the device by an orogastric approach with cutting of the tube [11]. Although uncommon in the United States, this practice is the usual approach taken both in South America and Europe.
Liver abscesses are the most common form of visceral abscess, accounting for almost one-half of such infections [17]. The majority of cases occur in the fifth and six decades of life, corresponding to the increased incidence of biliary disease in middle age, which is the foremost cause of pyogenic liver abscess. There is a higher inclination for the abscess to form in the right lobe of the liver and solitary lesions are found in approximately 50% of cases. Historically, pyogenic liver abscesses have been classified according to the presumed route of hepatic bacterial invasion [18]. Infection of the biliary tree (cholangitis), usually as a result of obstruction, often leads to the formation of multiple lesions and is believed to be the etiologic event in 40%–50% of liver abscess diagnoses. Bacterial seeding of the liver parenchyma either through the hepatic artery (e.g., in endocarditis) or by direct drainage from the portal venous system (pylephlebitis associated with appendicitis, diverticulitis, omphalitis, pancreatitis, or post-operative infection) each account for roughly 5%–15% of these hepatic infections. Direct extension from a contiguous focus of infection (e.g., subphrenic abscess) and traumatic events (either penetrating or blunt) are presumed to be the source of infection in 5%–10% and 1%–5% of cases, respectively. In our case, direct seeding from trauma caused by surgical instruments, particularly a seeded liver retractor, is a possibility. However, a large percentage of liver abscesses (20%–40%) are deemed to be cryptogenic, postulated to be due to non-specific bacterial invasion of the liver in some individuals with underlying chronic medical conditions. Most pyogenic liver abscesses are polymicrobial, with the microbiology usually characterized by the route of infection. When infection is determined to be monomicrobial, arterial seeding or cryptogenic disease should be suspected. Successful isolation of the causative organism(s) occurs in 80%–90% of cases, with mixed enteric facultative and anaerobic species being the most common pathogens. Failure to cultivate the etiologic pathogen(s) can be attributed to infection with a fastidious organism, culture technique, or prior antimicrobial treatment.
Clinically, fever and abdominal pain (localized in the right upper quadrant) are the chief presenting complaints in patients with a liver abscess. More often than not, concurrent gastrointestinal symptoms such as vomiting, diarrhea, and abdominal cramps are absent. Abnormal laboratory studies, although not specific, characteristically include a moderate leukocytosis and an elevated alkaline phosphatase concentration. Radiographic imaging is essential to diagnose a pyogenic liver abscess. Contrast-enhanced CT scans and ultrasonography are the most useful. Although CT scanning provides a higher sensitivity (95% versus 70%–90%) than ultrasound [19–20], the latter modality is recommended in those patients with suspected biliary disease or if the use of intravenous contrast is contraindicated.
Treatment of pyogenic liver abscesses almost always requires a combination of drainage and antimicrobial therapy [17]. Percutaneous image-guided drainage procedures are preferred to surgery. Nonetheless, surgical intervention may be required if percutaneous drainage cannot be accomplished or management of coexistent intra-abdominal disease is necessary. In some patients, percutaneous aspiration without placement of an indwelling catheter may be adequate. Medical treatment of liver abscesses alone should only be reserved for very small lesions not amenable to drainage or if the circumstances are such that the risk of drainage is too high. Antimicrobial therapy is usually provided for four to six weeks, the first one-half of which preferably is given parenterally [17].
Conclusion
The original gastric bypass operation was conceived as a variation of gastric ulcer surgery more than four decades ago [21] after observing that patients who had undergone a partial gastrectomy for treatment of peptic ulcer disease experienced a substantial amount of weight loss.
As more patients continue to seek bariatric surgery as a means for weight reduction, LAGB procedures will continue to grow in number and popularity. In the only prospective randomized trial to compare the outcomes of LAGB surgery with laparoscopic gastric bypass [22], those patients who underwent the bypass operation had a higher percentage of excess body weight loss at the 5-y follow-up. However, one large meta-analysis concluded that LAGB had a lower operative mortality rate than gastric bypass (0.1% versus 0.5%, respectively), with the most frequent causes of death being pulmonary embolism and anastomotic leak [6].
Furthermore, gastric bypass is associated with a higher complication rate than LAGB [23]. However, for obvious reasons, the uncommonly encountered complication of band erosion is limited to the LAGB, and when symptomatic may be associated with the development of an adjacent intra-abdominal abscess.
To the best of our knowledge, pyogenic liver abscess formation resulting from band erosion has not been reported previously as a complication of LAGB weight loss surgery. We suspect that bacteria gained entry into the liver parenchyma from an unusual cause of pylephlebitis (infective suppurative thrombosis of the portal vein) as a consequence of an injury that occurred from the eroded band in proximity to the coronary vein (gastric vein). Among the various blood vessels that serve to drain blood from the abdominal part of the digestive tract, the coronary vein derives tributaries from both surfaces of the stomach, coursing from right to left along the lesser curvature of the stomach to the esophageal opening of the stomach, where it also receives some esophageal veins, eventually ending in the portal vein behind the omental bursa. At the level of the liver hilum, the portal vein divides into a right and left branch, with the right branch entering the right lobe of the liver directly. In general, under normal physiologic conditions, the micro flora of the human upper gastrointestinal tract is sparse, consisting of various streptococcal species, lactobacillus, and anaerobic gram-negative bacilli. Our microbiology laboratory's inability to identify a specific organism may have been influenced by the prior administration of antimicrobial agents, or related to the fastidious nature inherent to many intestinal bacterial inhabitants.
Footnotes
Author Disclosure Statement
No competing financial interests exist.