
Abstract
Abstract
Background:
Thoracoabdominal actinomycosis is rare, especially in the context of readily available medical facilities.
Methods:
Case report and review of the literature.
Case Report:
A 54-year-old male patient was admitted because of hemoptysis and a pulmonary infiltrate in the left lower lobe. His history was unremarkable except for chronic gastritis and an elective laparoscopic cholecystectomy performed 10 years earlier. Following persistent hemoptysis, elevated inflammatory markers, and a non-revealing bronchoscopy, a computed tomography scan of the thorax and upper abdomen revealed a tumor in the upper part of the left kidney spreading directly to the adjacent diaphragm and left lower lobe. Laparotomy revealed a granulomatous mass containing a gallstone, as well as orange granular content. The treatment involved surgical removal of the mass, splenectomy, excision of the infiltrated part of the left hemidiaphragm, and decortication of the left lower lobe. Because of a prolonged post-operative low-grade fever and radiologically confirmed encapsulation in the lingula, the patient was given ceftriaxone. Repeat bronchoscopy revealed Actinomyces meyeri. The initial antibiotic therapy was replaced with amoxicillin-clavulanic acid, after which the patient's health improved.
Conclusion:
Actinomycosis is still a highly intriguing disease, as initial symptoms often mislead clinicians. It is important to consider the disease whenever we are challenged diagnostically or when risk factors are present.
If bowel trauma occurs, resulting in a disrupted mucosal barrier, commensal bacteria might act as pathogens, invading deeper tissues. Actinomyces normally is part of the oropharyngeal and gastrointestinal flora and that of the female genital tract. In case of a disrupted mucosal barrier, Actinomyces causes disease with clinical features divided into three subtypes: Cervicofacial, thoracic, and abdominal, the most prevalent of which is the cervicofacial, occurring in as many as 55% of affected patients [6]. Thoracic and abdominal actinomycosis are less common forms, 15%–20% and 10%–20%, respectively. The infection can also spread via the blood stream to other organs, causing generalized actinomycosis. Current recommendations for treating actinomycosis include intravenous penicillin at a dose of 18–24 million U daily for 2–6 wks followed by oral penicillin or amoxicillin for 6–12 mos [1,2].
Case Report
A 54-year-old male patient was admitted to the hospital with a two-month history of intermittent high-grade fever and coughing. His medical history was unremarkable except for chronic gastritis and an elective laparoscopic cholecystectomy performed 10 years earlier because of chronic cholecystitis. He was a smoker (30 pack-years). During his professional life, he was not exposed to chemicals or other irritants.
The present disease started with high-grade fever during the evening hours, cough, and general malaise. A respiratory tract infection was suspected, and the patient received a seven-day oral cefuroxime regimen, 250 mg twice daily. The fever recurred when the antibiotic was discontinued. Chest radiography revealed an infiltrate in the basilar part of the left lower lobe. Amoxicillin-clavulanic acid was administered, 1 g twice daily. The infiltrate resolved, but six weeks later, the high-grade fever returned, followed by hemoptysis. His general practitioner administered clindamycin, 300 mg twice daily. Because of persistent hemoptysis, he was sent to the hospital.
On admission to the Clinic for Lung Diseases, the patient was afebrile. On physical examination, there was no breath sound heard in the basal part of the left lung lobe. Laboratory tests revealed a leukocyte count of 13,200/mm3 (neutrophils 13.2%, lymphocytes 11.1%, and monocytes 7.7%), hemoglobin 12.0 g/dL, platelet count 430,000/mm3, C-reactive protein 18.5 mg/dL, aspartate aminotransaminase 30 U/L, alanine aminotransaminase 75 U/dL, gamma glutamyl transpeptidase 149 U/L, and alkaline phosphatase 154 U/L. The serum sodium concentration was 135 mmol/L. There were no other serum abnormalities. Tumor marker tests (CYFRA 21-1, neuron-specific enolase, and carcinoembryonic antigen) were all negative. Sarcoidosis and tuberculosis were excluded.
Repeat chest radiography revealed a dense infiltrate in the posterobasilar segment of the left lower lobe. Bronchoscopy did not show signs of an endobronchial lesion, only scant bleeding visible in the medial basilar segment of the left lower lobe. Samples taken during bronchoscopy showed inflammatory cells (mostly neutrophils), whereas malignant cells were not found.
Because of the continued hemoptysis, computed tomography (CT) of the thorax and upper abdomen was obtained that showed an abdominal tumor, 12 cm in diameter, involving the upper part of the left kidney and spreading in continuity through the diaphragm to the left lower lobe (Fig. 1).
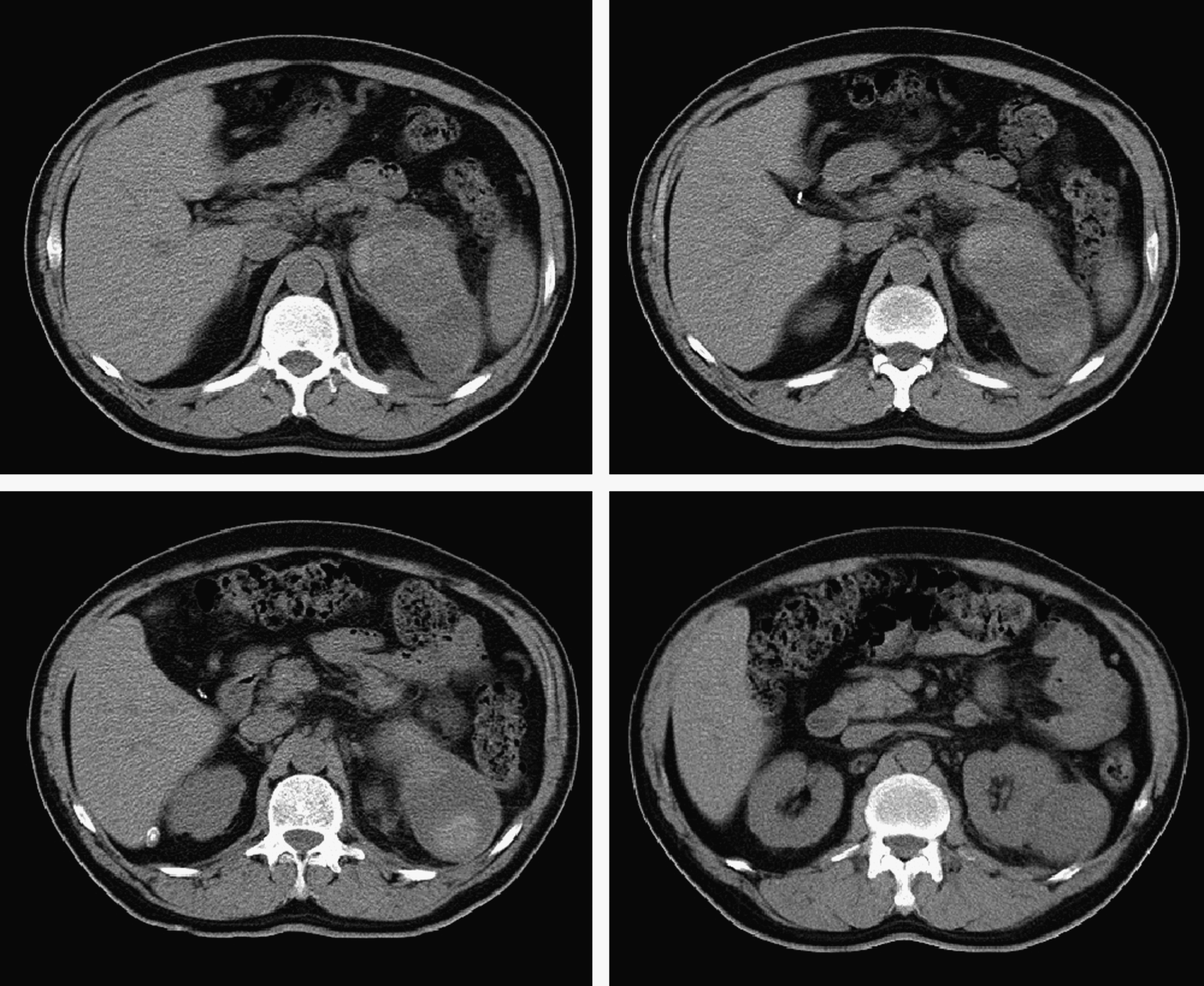
Abdominal computed tomography scan demonstrates a 12-cm mass at the upper pole of left kidney.
The patient was sent to a tertiary-care hospital for a multislice CT scan with intravenous contrast medium, which demonstrated a complex mass comprised of the area adjacent to the pancreatic tail, the lateral aspect of the left kidney, and the left subphrenic space with spread into the left lower lobe. A left thoraco-abdominal exploration revealed a huge tumor infiltrating the left hemidiaphragm, the visceral pleura of the left lower lobe, and the pancreas. Surgical excision was performed of the central part of the left hemidiaphragm splenectomy, and decortication of the part of the pleura involved in this inflammatory process. The pancreas and the left kidney were left intact. Within the tumor was a gallstone, later confirmed by pathology. Intra-operative cultures of the left subphrenic space did not yield any organisms. No malignant cells were found.
Post-operatively, the patient received ciprofloxacin, 500 mg twice daily for five days. Because of the persistent low-grade fever, ertapenem was added, 1 g daily. Cultures from the repeat bronchoscopy revealed Actinomyces meyeri (Fig. 2). The therapy was replaced with intravenous amoxicillin-clavulanic acid for 14 days, 1.2 g three times a day. The early post-operative course was complicated by retroperitoneal hemorrhage, mandating re-laparotomy for hemostasis. The further post-operative course was uneventful, without any signs of recurrence of Actinomycosis one year after surgery (Fig. 3).

Gram stain of bronchial aspirate demonstrating branching, gram-positive organisms characteristic of actinomycosis. (By courtesy of Esmina Prahin, Eng'r; Department of Microbiology, University of Zagreb School of Medicine.) Color image is available online at www.liebertpub.com/sur

Follow-up abdominal computed tomography scans one year after operation.
Discussion
Laparoscopic surgery has become the gold standard for the treatment of symptomatic choleolithiasis. Although the initial reports described a higher complication rate [7], the present data confirm that laparoscopic cholecystectomy has lower morbidity and mortality rates than open operation [8]. Specific complications that follow laparoscopic cholecystectomy are leakage from the cystic duct, injury to the main bile duct, retained gallstones, and perforation of the gallbladder [7]. However, complications may arise long after the operation, imposing a diagnostic challenge for clinicians.
Literature is abundant on intra-abdominal infections relating to Actinomyces spp., retained gallstones, or a combination of the two. Intra-abdominal abscess is the most frequent complication of laparoscopic cholecystectomies with retained gallstones [2]. Gallbladder perforation and intraperitoneal spillage of gallstones are common, occurring in as many as 40% of all laparoscopic cholecystectomies [5]. The average time from the operation until the onset of symptoms is 5.5 months [9,10].
In the early era of laparoscopy, retained gallstones were considered harmless, as confirmed in animal models [11]. With a growing body of literature on the complications of this technique, however, awareness of deleterious effects has increased. Spilled stones should be removed laparoscopically, with the peritoneal cavity washed extensively; therapy may be antibiotic administered post-operatively [12]. Brockmann et al. identified several risk factors for complications in patients with intraperitoneal gallstones: Acute cholecystitis, perihepatic location of retained gallstones, more than 15 gallstones, average size of gallstone >1.5 cm, male gender, and advanced age [5].
To our knowledge, there is only one report of thoracoabdominal actinomycosis associated with retained gallstones [13]. This is the first report of A. meyeri causing thoracoabdominal actinomycosis on a gallstone nidus.
Actinomyces is a saprophyte in the oral cavity, gastrointestinal tract, and female genital tract. If the mucosal barrier is disrupted by mechanical trauma, surgical intervention, placement of intra-uterine device, or periodontal disease, Actinomyces penetrates tissues and organs easily. The most common infection in humans is with A. israelii [14]. Actinomyces meyeri is isolated rarely in cases of actinomycosis. It often causes pulmonary infection and has a tendency for hematogenous dissemination. Infections caused by A. meyeri are more prevalent among males (the male-to-female ratio is 20:6) with a mean age of 42.5 years [15].
The major risk factor for an infection caused by A. meyeri is periodontal disease, which our patient was determined to have had previously, in retrospect.
Because of the fastidious nature and slow growth of Actinomyces, the organism may be missed, especially if antibiotics are administered. Furthermore, prompt transport of either resected specimens or deep needle aspirate to the microbiology laboratory is necessary for optimal isolation of actinomycetes, preferably in an anaerobic transport device.
Actinomycosis, as a granulomatous inflammation/mass, may be mistaken for malignant disease, inflammatory bowel disease, or intestinal tuberculosis [16]. Therefore, diagnosis usually is established postoperatively, especially in emergency settings. Because of the non-characteristic signs and symptoms, a proper diagnosis is made in only 10% of cases [17], as in our patient. Because of the long time between laparoscopic cholecystectomy and the presenting disease—in our patient, 10 years—the proper diagnosis of retained gallstone was delayed, especially considering that the presenting symptoms appeared in the respiratory tract only (even though the abdominal mass was large, he experienced no abdominal symptoms). Our hypothesis is that the retained stones served as a nidus for chronic inflammation with the slowly growing Actinomyces. Finally, the invasive granulomatous inflammation spread through adjacent tissues, causing predominantly respiratory symptoms.
There are no recommendations for the duration of treatment of such infections. Our patient received a short course of antibiotic therapy, in addition to complete en-bloc excision. Long-lasting (6 mo–1 yr) penicillin treatment is recommended if used as a single modality [18], as the intense desmoplastic reaction associated with actinomycosis limits drug penetration [19]. In patients allergic to penicillin, tetracyclines and clindamycin are used. If patients remain symptomatic after a month of penicillin therapy, additional antibiotics should be considered because of the likelihood of a polymicrobial superinfection. Resection of the infected tissue is recommended to reduce the chance of recurrence, along with a short antibiotic course [19]. There is a need to evaluate the patient regularly with radiologic and clinical follow-up.
Footnotes
Author Disclosure Statement
No competing financial interests exist.