
Abstract
Abstract
Background:
We conducted a study with the primary objective of assessing whether a difference existed in the frequency and type of surgical interventions (SIs) implemented in patients treated with linezolid versus vancomycin for the management of complicated skin and skin structure infections (cSSSIs) caused by methicillin-resistant Staphylococcus aureus (MRSA).
Methods:
We analyzed data from a phase IV clinical trial evaluating the safety and efficacy of linezolid and vancomycin, given for 7–14 d, to treat cSSSIs other than cellulitis that were caused by MRSA. The study included patients who received ≥1 dose of drug, had a cSSSI caused by culture-proved MRSA, and underwent ≥1 SI after commencement of the study. The types and frequencies of SIs were assessed on a per-patient basis during the following three time periods: (1) study days 0–3: the estimated time to reach steady-state serum drug concentrations; (2) study days 4–14: the drug-treatment period (days 4–14) during which steady state drug concentrations are likely reached; and (3) study days 15–28: the post-treatment period through end of the study (EOS). Independent predictors of ≥2 SIs during the drug-treatment period were identified by logistic regression. Clinical and microbiologic outcomes were assessed at the end of treatment (EOT), and at EOS for the SI population.
Results:
The data analysis included 323 patients (linezolid, n=167; vancomycin, n=156). The majority of patients (81% in the linezolid group and 83% in the vancomycin group) underwent an initial SI or source control procedure within 72 h of study initiation. The most common cSSSIs among patients having SIs were abscesses (59%) and infected ulcers (20%). Independent predictors of ≥2 SIs during study days 4–14 included treatment with vancomycin (OR 5.97; 95% CI 1.97-18.03), polymicrobial infection (OR 2.84; 95% CI 1.13-7.12), and degree of wound induration (OR 1.06; 95% CI 1.02–1.10). Clinical success rates in the SI population were 88% in the linezolid group and 80% in the vancomycin group (p=0.14) at EOT and 80% in the linezolid group and 68% in the vancomycin group (p=0.04) at EOS. Microbiologic success rates were 83% in the linezolid group and 68% in the vancomycin group (p=0.004) at EOT and 71% in the linezolid group and 60% in the vancomycin group (p=0.05) at EOS.
Conclusion:
Patients who received linezolid had a lower probability of undergoing ≥2 SIs during drug treatment. Type of antibiotic received was the only modifiable predictor of a greater rate of SI during the drug-treatment period. In the patient population of the study, with cSSSIs other than cellulitis that were caused by MRSA, and in which at least one SI per patient was done within 72 h of the commencement of drug treatment, linezolid was associated with a higher rate of clinical success at EOS than was vancomycin, as well as with a higher rate of microbiologic success at both EOT and EOS.
The tenets of treatment for cSSSIs include the use of two therapies, such as aggressive surgical drainage and debridement to ensure source control, together with the simultaneous selection of an appropriate antimicrobial agent to cover expected pathogens [4]. To provide empiric treatment successfully, it is necessary to understand the factors that put the patient at risk for infections with methicillin-resistant Staphylococcus aureus (MRSA) and other multi-drug–resistant pathogens [5]. Furthermore, despite the dependence of a successful outcome on both of the two treatment techniques named above, little is understood about how they might affect each other.
A paucity of data exist about the extent to which an antimicrobial drug may influence surgical interventions (SIs) in the management of cSSSIs. Given the increased resource utilization for and potential morbidity and mortality among patient with multiple SIs, identifying an antimicrobial drug that decreased the extent of the surgery required for treating cSSSIs would be beneficial. We conducted a study to determine whether such an effect exists.
We hypothesized that patients treated with linezolid for cSSSIs caused by MRSA may require fewer and less extensive SIs than those treated with vancomycin. The primary objective of our study was to determine whether a difference exists in the frequencies and types of SIs implemented for patients treated with linezolid and those treated with vancomycin for cSSSIs caused by MRSA. Secondary objectives of our study included the identification of independent predictors of the need for multiple SIs and assessment of the clinical and microbiologic outcomes of patients who underwent SIs.
Patients and Methods
We analyzed data generated in a phase IV, randomized, open-label, clinical trial comparing linezolid with vancomycin for the management of documented MRSA-induced cSSSIs [6]. In this trial, eligible adults (age ≥18 years) were randomized (1:1) to receive either linezolid 600 mg intravenously (IV) or orally (PO) q12h, or vancomycin 15 mg/kg IV q12h (with dosages adjusted by an unblinded pharmacist on the basis of renal function and serum drug concentration) for 7–14 days to treat a documented MRSA-induced cSSSI. Patients included in the trial had at least two symptoms associated with a cSSSI that involved deep tissue (purulent drainage, erythema, swelling or induration, tenderness or pain, and local warmth) and at least one sign of systemic infection (fever, hypotension, or a white blood cell [WBC] count ≥10,000/mm3 or >15% immature neutrophils regardless of the total WBC count). Patients with diabetic foot infections were considered eligible on the basis of evidence of a deep infection of the foot, ankle, or lower leg that required a surgical procedure; through an identifiable wound with evidence of purulence or erythema over more than 50% of the surface area of the foot, ankle, or lower leg; or streaking in the medial arch of the foot. Exclusion criteria at the time of enrollment in the trial were cellulitis, necrotizing fasciitis, septic arthritis, osteomyelitis, and receipt of an MRSA-active antibiotic for more than 24 h within 72 h of enrollment. Aztreonam (or another antibiotic known to be inactive against gram-positive organisms) and metronidazole were permitted for treating infections caused by gram-negative and anaerobic pathogens, respectively.
Clinical and microbiologic responses were evaluated at the end of treatment (EOT) as cure, improvement, failure, or an unknown response. Clinical response was categorized at the end of study (EOS) visit, at 6–28 d after EOT, as cure, failure, or unknown on the basis of the primary outcome in the original clinical trial. A classification of clinical cure required the receipt of four or more full days of study medication, and a classification of failure required two or more full days of study medication. Clinical success was defined as the resolution of clinical signs and symptoms of infection that were identified at baseline. Microbiologic success was defined as a negative MRSA culture from the original site of infection, or as presumed eradication of MRSA when no culture data were available and the patient's clinical outcome was a success. Microbiologic failure was defined as a positive MRSA culture and categorized as a persistent or recurrent infection or presumed persistence of infection when no culture data were available and the clinical outcome was defined as failure. The Wilson score was used to assess and compare the severity of cSSSI in the two treatment groups [7].
Our analysis included the population of the original clinical trial that underwent SI (the SI population), which included patients who received at least one dose of study medication, had a positive culture at baseline screening (designated as the modified intent-to-treat [mITT] population), and underwent at least one SI after the beginning of the trial. Surgical interventions were captured in text fields in procedural data, without any capture of data on the adequacy of surgical treatment, need for further intervention, or location of surgery. Thus, the need for, type, and/or adequacy of surgical treatment were not dictated as parts of the methods included in the clinical trial on which our study was based, but were instead determined by the patient's surgeon as components of the standard of care.
Assessment of surgical interventions
Data on SIs (number and type) were collected in the procedures section of the case report form for each patient in the original clinical trial. Three independent reviewers (B.C., L.A.P., and M.J.) coded the surgical procedure data and collected data from the original clinical trial to assess and categorize an SI in the mITT population as incision/drainage (I/D), excision/debridement (E/D), surgical closure, or amputation. Data were entered and reviewed for inter-rater reliability. Any discrepancies were resolved by an independent fourth reviewer (T.M.D.) and final categorization was unanimous among all reviewers. The types and frequencies of SIs per patient were collected, categorized, and quantified during each of the three distinct study periods as (1) SIs occurring from study day 0 (time of initiation of drug treatment) through study day 3, the estimated period during which steady-state serum drug concentrations would be reached; (2) SIs occurring from day 4 through day 14, constituting the drug-treatment period during which steady-state serum drug concentrations had likely been reached; and (3) SIs occurring from day 15 through day 28, the period following EOT and extending to EOS. A performance of ≥2 SIs was chosen as a threshold for comparison of the groups of patients, and in logistic regression analysis as reflecting patients who underwent additional SIs after an initial source control procedure as a standard of care.
Statistical analyses
Descriptive analyses were done to evaluate the distribution of covariates among the treatment regimens in the study. Statistical comparisons of groups were done with the χ2 test for categorical variables and two-sample t-test for continuous variables, with significance set at p≤0.05. Frequencies of SIs were also tabulated for the two antibiotic treatment groups by time and type of intervention. Clinical and microbiologic success rates at EOT and EOS were compared for treatments through use of the absolute difference and the 95% confidence intervals (CIs) for the differences in rates. P values were used for the Fisher exact test. Multivariate logistic regression was used to identify factors predictive of at least 2 SIs during study days 4 to 14. Covariates with a value of p≤0.25 met the screening criteria and were considered for inclusion in the model-building process. These covariates were study treatment, baseline diastolic blood pressure, baseline respiratory rate, baseline pulse rate, baseline hemoglobin, baseline platelet count, skin-injury severity score [7], presence of pain at baseline (yes/no), width of induration, width of erythema, infection in a lower extremity (yes/no), polymicrobial infection (yes/no), region of study (United States/outside the United States), and body weight under 75 kg (yes/no). The final model was selected through a backward elimination process. This process involves first estimating parameters for the complete model, followed by examination of the results for individual parameters. Any effect that does not meet the p=0.05 threshold for maintenance in the model is removed. Once an effect is removed from the model, it remains excluded. This process is repeated until no effect in the model meets the specified level for removal. Goodness of fit was assessed with the Hosmer–Lemeshow test [8].
Results
A total of 323 (linezolid, n=167, and vancomycin, n=156) patients in the mITT group underwent at least one SI after initiation of the original trial, and constituted the SI population for the current analysis. Baseline demographic characteristics (Table 1) were similar in the two groups among the SI population, with the exception that more males received vancomycin than linezolid (107 [69%] vancomycin, 96 [58%] linezolid; p=0.05]. Most of the patients in both treatment groups underwent an initial SI within the first 72 h (days 0–3) of the beginning of the study and commencement of drug treatment (136/167 [81%] in the linezolid and 129/156 [83%] in the vancomycin group; p=0.88). No difference was identified in the baseline clinical characteristics of the two groups (Table 2), whether in underlying co-morbidities, skin infection; type, size, and location of lower-extremity wounds; or presence of polymicrobial infection. The most common co-morbidity among the SI population in both groups was vascular disease (48% linezolid, 47% vancomycin), which was followed by diabetes mellitus (36% linezolid, 37% vancomycin). Abscess was the most prevalent diagnosis for skin infection (59% linezolid, 60% vancomycin) in both groups. The proportion of patients in whom treatment began as oral therapy was 73/167 (43%) in the linezolid treatment group.
LZD=linezolid; VAN=vancomycin; SD=standard deviation.
p=0.050.
Percentages were rounded and may not add up to 100.
Other category was not qualified on the case-report form.
LZD=linezolid; VAN=vancomycin; MRSA=methicillin-resistant Staphylococcus aureus; SD=standard deviation; NA=not applicable.
Other included blister, bursitis, cellulitis, diabetic foot infection, erysipelas, hematoma, infected insect bite, and soft tissue infection.
The Wilson severity score is based on a validated scoring system in which baseline variables predict outcome. Points are assigned based on age, findings on physical examination, laboratory tests, size and degree of wound involvement, presence of surgical site infection, bacteremia, and comorbid conditions [7].
Mean (±SD) trough serum concentrations of vancomycin of 9.8 (±7) mcg/mL and 11.8 (±7) mcg/mL were attained on day 3 and day 7, respectively, among vancomycin-treated patients (Table 2). The average minimum inhibitory concentration (MIC) of vancomycin among MRSA isolates, as determined by micro-broth–dilution susceptibility testing, was 1.0 mcg/mL. The proportions of patients who underwent specific types of SI during the study period are shown in Figure 1; it should be noted that patients may have undergone multiple types of interventions during a single surgical procedure. No difference was found in the number of patients in the two groups who underwent I/D, E/D, amputation, or surgical closure. The most common types of intervention were I/D (in 116 [70%] of the linezolid-treated patients and 106 [68%] of the vancomycin-treated patients) and E/D (in 55 [33%] of the linezolid-treated patients and 57 [37%] of the vancomycin-treated patients). There were no differences between the groups in the types of SIs that patients had undergone as their first, second, or third interventions.
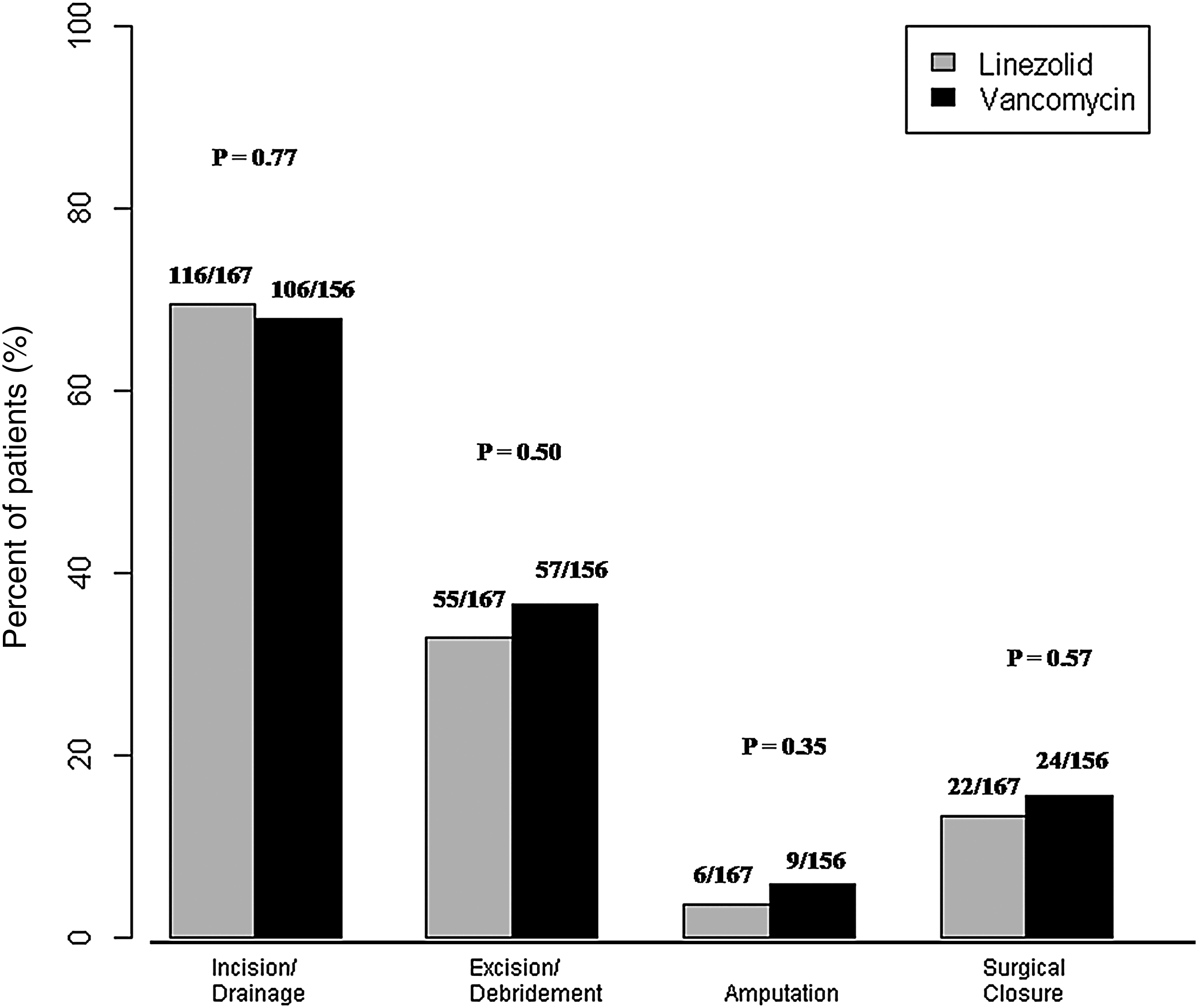
Percent of patients with surgical interventions by intervention type.
Figure 2 illustrates the percentage of patients who underwent two or more SIs during one of the three time periods in the study. A significantly higher proportion of patients treated with vancomycin than with linezolid underwent ≥2 SIs during the drug treatment period (3% in the linezolid and 12% in the vancomycin group; p=0.002). Additionally, treatment with vancomycin was predictive of ≥2 SIs during the drug-treatment period as determined by logistic regression (Table 3). Other factors predictive of multiple SIs during the drug-treatment period included polymicrobial infection and the extent of wound induration.

Percent of subjects who underwent ≥2 surgical interventions.
In addition to these predictors, the backward elimination procedure also identified infection in a lower extremity as a predictor of ≥2 SIs, but is not shown here because its effect was not significant at p=0.05.
An additional comparative and regression analysis was done in the cSSSI patient subgroup with abscesses. Abscess was diagnosed in a total of 192 patients in the SI population, of whom 98 received linezolid and 94 received vancomycin. In accord with the analysis in the overall SI patient population, a higher proportion of patients in the abscess subgroup who were treated with vancomycin than with linezolid underwent ≥2 SIs during the drug treatment period (11% vancomycin and 2% in the linezolid treatment groups; p=0.01). Furthermore, treatment with vancomycin, induration width, and infection in a lower extremity were identified as statistically significant predictors of ≥2 SIs during the drug-treatment period. Polymicrobial infection was not identified as an independent predictor of ≥2 SIs in the abscess-only group, in contrast to the overall SI patient population.
The clinical success rates in the two treatment groups were similar at EOT (88% linezolid, 80% vancomycin; difference [95% CI] 7.1%; –1.5%-15.6%; p=0.14), but clinical success at EOS was achieved in a greater proportion of the SI population treated with linezolid than with vancomycin (80% linezolid, 68% vancomycin; difference [95% CI] 11.5%; [0.6%-22.3%]; p=0.04). Additionally, microbiologic success was achieved at EOT in a greater proportion of the SI group that was treated with linezolid than with vancomycin (83% linezolid, 68% vancomycin; difference [95% CI] 15%; [5.2%-25.1%]; p=0.004), and the same was true at EOS (71% linezolid, 60% vancomycin; difference [95% CI] 11.5%; [0.04%-22.9%]; p=0.05).
Discussion
During the past two decades there has been an increase in the number of patients with diagnoses of skin and soft tissue infections [1]. This is probably the consequence of an increase in the number of patients with risk factors associated with these disease processes, as well as of an increasing incidence in the human community of more invasive organisms, such as community-acquired MRSA. In the present study, patients having SI had a high prevalence of vascular disease (47%), diabetes mellitus (36%), cardiac disease (28%), and chronic kidney disease (13%), most of which are co-morbidities of importance in patients with MRSA infections [9]. As more patients develop co-morbidities requiring hospital care, an understanding of appropriate therapy for these patients is paramount to optimizing their outcome.
It is often challenging to determine the best therapy for a cSSSI because of the range in severity and type of these conditions. For example, cellulitis confined to the inflammation of soft tissue is treated ideally with antimicrobial drugs alone [4], whereas uncomplicated surgical infections, without systemic signs of infection, require drainage alone, without the use of antimicrobial drugs. Complicated infections in which there is bacterial invasion of soft tissue together with abscess formation require a balance of surgical and medical interventions [10].
The surgical approach to cSSSIs is focused on the removal of all necrotic tissue and purulence, because the penetration of antimicrobial drugs into these areas is poor if not non-existent. Most interventions should include early I/D as well as excision of tissue according to the depth and degree of necrosis [11]. In the present study the large majority of patients underwent I/D, which is consistent with complicated abscess having been the most common diagnosis in this group. Excision and debridement was the second most common operative intervention, suggesting that some of the infections required additional debridement of tissue beyond simple evacuation of pus. It is important to keep in mind that the type of surgery required and the need for re-operation was determined by each individual surgeon in the original trial and was not standardized for the trial. Because our analyses were based on data generated from a large, multi-center, multi-national clinical trial, we assumed that the types and frequencies of SIs implemented reflected the standard of care for patients with cSSSI. Planned re-operation is a key component of the surgical care of cSSSIs because it is often difficult to determine tissue viability or to predict progression of disease at the time of initial operation. However, the effect of choice of an antimicrobial drug on the need for further surgery has not previously been considered. The choice of antimicrobial drug has typically been based on the prevalence of various pathogens.
The guidelines of the Surgical Infection Society discuss in detail the pathogens that need to be covered when dealing with cSSSIs [4]. The more common gram-negative organisms include Pseudomonas aeruginosa and Escherichia coli, yet these are far less common than S. aureus [5,12]. Staphylococcus aureus is found much more often than are the other two organisms, constituting almost 50% of all isolates in North America from 1998 to 2004 [13]. Because of this and the increase in MRSA as a pathogen, these guidelines include coverage of community-acquired MRSA in most settings.
Vancomycin has long been considered the gold standard in the treatment of cSSSIs caused by MRSA. However, a number of studies have demonstrated the efficacy of linezolid in the treatment of these disease processes, including both cSSSI and diabetic foot infections without osteomyelitis [14,15,16,23]. Moreover, linezolid is approved by the U.S. Food and Drug Administration for cSSSIs caused by MRSA because of its demonstrated non-inferiority to vancomycin [6]. Additionally, because of its 100% bioavailability [17], linezolid is the only oral agent approved by the FDA for treating cSSSIs caused by MRSA. A major difference between linezolid and vancomycin is the need to monitor serum concentrations of vancomycin to adjust its dosing, which is not required with linezolid [18]. As demonstrated in the present study, reaching and maintaining the “target” vancomycin serum trough concentration threshold of 15 mcg/mL, as recommended for serious MRSA infections, is challenging even under closely regulated study conditions [19].
To our knowledge, our study is the first to have evaluated the role of antimicrobial drug choice in the necessity for re-operation in cSSSIs. This is an important consideration in view of the close linkage of repeated SI with the choice of antimicrobial therapy in the treatment of cSSSIs. With the increase in resource utilization and risk to the patient with multiple operations, it is valuable to determine whether drug selection affects the need for repeat surgery. The findings in our study indicated that the use of vancomycin was an independent predictor of the need for ≥2 SIs. This was found despite the similar baseline characteristics of the patients in the vancomycin- and linezolid- treatment groups in the study.
An explanation for this difference may be related to the tissue penetration of linezolid [20]. Patients requiring repeated SI may have tenuous blood flow to the tissue surrounding necrotic tissue debrided previously and into the cavity of an abscess, limiting antibiotic delivery to these areas [21]. Although we did not study this directly in a comparative fashion, linezolid may be more successful in penetrating into such areas and reaching higher tissue concentrations because of its chemical properties. An adequate antimicrobial drug concentration would result in more effective elimination of the offending organisms and prevent further tissue necrosis and liquefaction, thereby maintaining tissue viability and eliminating the need for further debridement. A possible second explanation could be that over recent decades, the susceptibility to vancomycin of some strains of MRSA has decreased [22]. It has been demonstrated that in clinical sites of infection, hetero-resistant strains of both vancomycin-susceptible and vancomycin-resistant S.aureus could coexist [23–25]. Routine clinical laboratory testing of samples from an infected site may not be sensitive enough to detect a small percentage of vancomycin-resistant strains, and these strains may be reported as susceptible [26]. The primary study on which this analysis was based, conducted by Itani et al. [6], also used routine cultures and may therefore not have detected heteroresistant strains of S. aureus. In such mixed infections, linezolid may be preferred as an antimicrobial agent.
This study has some limitations. It is a post hoc analysis of a prospective, randomized trial and therefore was not designed to assess for differences in frequency and type of surgical interventions between treatment groups. In addition, the data on SIs collected for the study were limited in the original trial to number, date, and type of SI. Therefore, data on the decision to perform surgery, on the adequacy of surgical treatment, and on the need for repeat operative interventions were not available for our analysis. However, these types of data are based on clinical decision making as part of the standard of care, and allowed the assessment of frequency and type of SI used for a particular patient independent of the study intervention. Hence, we were unable to control for the reasoning behind the initial operation, or which patients underwent re-operation and when re-operation occurred. A prospective study with specific questions for the surgeon at time of SI would be beneficial for elucidating our findings further. As an additional limitation to our study, the serum trough concentrations of vancomycin used in the trial on which the study was based were lower than the concentrations recommended for treating severe MRSA infections [19]. Nevertheless, the average serum trough concentrations of vancomycin on both day 3 and day 7 exceeded the MIC of vancomycin of 1.0 mcg/mL for most of the pathogens in the two study treatment groups (83% of those in the vancomycin-treated patients and 82% of those in the linezolid-treated patients as measured by microtiter susceptibility testing). Moreover, the serum trough concentrations of vancomycin may reflect real clinical experience, because the vancomycin dosing in the original clinical trial was managed by an unblinded pharmacist who was permitted to adjust doses according to serum concentrations on the basis of the standards of care at the institutions involved in the trial.
In this study, patients who received linezolid for the management of a cSSSI had a lower probability than those treated with vancomycin of undergoing ≥2 SIs during the treatment period of days 4–14, which was the period during which steady-state drug concentrations are assumed to be reached. The type of antibiotic received was the only modifiable predictor of undergoing ≥2 SIs during the drug-treatment period of the study. In the study population of patients with cSSSIs caused by MRSA and who underwent at least one SI, a higher rate of clinical success at EOS, as well as a higher rate of microbiologic success rate at both EOT and EOS, was observed with linezolid as compared with vancomyin. The results of this study are thought provoking and warrant further prospective study.
Footnotes
Acknowledgments
Programming support for this study was provided by Diane Ruzzi of Pfizer Inc.
Author Disclosure Statement
This study was sponsored by Pfizer Inc. T.M.D. and M.J. were paid consultants to Pfizer in connection with the study and the development of this manuscript, and B.C., L.A.P., and P.B. are employees and shareholders of Pfizer Inc.