
Abstract
Abstract
Background:
The Study for Monitoring Antimicrobial Resistance Trends (SMART) has tracked the in vitro activity of ertapenem and comparators against aerobic gram-negative bacteria from intra-abdominal infections since 2002. This report describes the epidemiology and susceptibility for clinical isolates associated with appendicitis, collected from 2008 to 2010.
Methods:
A total of 1,720 gram-negative bacilli were collected from patients with appendicitis in 122 hospitals in 39 countries worldwide; of these, 23% of isolates were from pediatric patients (≤17 years old). Minimum inhibitory concentrations (MICs) and extended-spectrum β-lactamase (ESBL) phenotypes were determined by broth microdilution and interpreted using Clinical and Laboratory Standards Institute guidelines.
Results:
The global ESBL-positive rate was 16.3%, ranging from 2.2% for Proteus mirabilis to 16.6% for Escherichia coli and 20.1% for Klebsiella pneumoniae. The ESBL-positive rates differed by age group (17.7% in adults vs. 11.4% in children) and by geographic region, with significantly higher rates in Asia/Pacific (28.0%) and significantly lower rates in North America (9.1%), Africa/Middle East (4.8%), and Europe (4.4%). Amikacin, imipenem-cilastatin, piperacillin-tazobactam, and ertapenem were the most active of the tested agents against aerobic gram-negative appendicitis pathogens across pediatric and adult age groups and across geographic regions, including ESBL-positive isolates. Cefepime and ceftazidime were active against ≥90% of global pediatric isolates. E. coli, by far the most frequently isolated species (68% in adults and 75% in pediatric patients), was significantly less susceptible in adults than in pediatric patients (p<0.05; Fisher exact test) to all tested agents except amikacin, ertapenem, imipenem-cilastatin, piperacillin-tazobactam, and ampicillin-sulbactam (with the latter showing low activity in both age groups).
Conclusions:
These in vitro data suggest that amikacin, imipenem-cilastatin, piperacillin-tazobactam, and ertapenem would perform well against aerobic gram-negative bacilli associated with appendicitis in both adults and children, especially in regions with high rates of ESBL-positive E. coli.
The Study for Monitoring Antimicrobial Resistance Trends (SMART) has been monitoring IAI for epidemiologic and antimicrobial susceptibility trends globally since 2002. This analysis of SMART data from 2008 to 2010 describes the occurrence of aerobic gram-negative bacilli, including extended-spectrum β-lactamase (ESBL) producers, in appendicitis-associated IAI and the susceptibility of these pathogens to ertapenem and common comparator agents.
Materials and Methods
Participating sites each collected as many as 100 consecutive aerobic or facultatively anaerobic gram-negative pathogens from IAI each year of the study. Only one isolate per species per patient was accepted. Of the 30,356 IAI isolates collected between 2008 and 2010, 1,720 were appendicitis-associated, collected from 122 hospitals in 39 countries (five sites in three countries in Africa/Middle East, 40 sites in 10 countries in the Asia/South Pacific region [including Australia and New Zealand], 35 sites in 13 countries in Europe, 20 sites in 11 countries in Latin America, and 22 sites in two countries in North America). Isolates from India were available only for 2008 and 2009.
Isolates were identified to the species level and sent to Laboratories International for Microbiology Studies (LIMS), a subsidiary of International Health Management Associates, Inc. (IHMA), Schaumburg, Illinois for susceptibility testing and confirmation of identification. Isolates from China collected in 2009–2010 were sent to the Peking Union Medical Center for susceptibility testing and confirmation of identification, using the same susceptibility testing panels as were employed at LIMS. Organism collection, transport, confirmation of organism identification, susceptibility testing, and development and management of a centralized database were coordinated by IHMA. Minimum inhibitory concentrations (MICs) were determined by the Clinical and Laboratory Standards Institute (CLSI)-recommended broth microdilution testing method using custom MicroScan panels (Siemens Medical Solutions Diagnostics, West Sacramento, CA) [6]. All antimicrobial agents were supplied by the panel manufacturer. The MIC interpretive criteria followed the January 2012 guidelines of the CLSI [7]. Quality controls (QCs) were performed on each day of testing using appropriate ATCC control strains, following CLSI and manufacturer guidelines. Results were included in the analysis only when corresponding QC results were within the acceptable ranges [7]. Escherichia coli, Klebsiella pneumoniae, K. oxytoca, and Proteus mirabilis isolates were classified as ESBL producers if there was at least an eight-fold reduction of the MIC for ceftazidime or cefotaxime tested in combination with clavulanic acid versus their MICs when tested alone [7].
The ESBL rates were analyzed by region, age group, and appendicitis versus non-appendicitis IAI. Confidence intervals were calculated using the adjusted Wald method. Differences in distribution and susceptibility of species between adult and pediatric patients, and in % ESBL-positive isolates between species and regions, were tested using the Fisher exact test, two-tailed. A p value<0.05 was considered statistically significant. Statistical analyses were performed with XLSTAT Version 2011.1.05 (Addinsoft, NewYork, NY).
Results
Of the 1,720 gram-negative bacilli collected from appendicitis specimens between 2008 and 2010, 387 (23%) were from pediatric patients. The ten most common species (n=1,671) made up 97% of all isolates, with the remaining 3% of isolates encompassing another 23 species. Table 1 shows the distribution of appendicitis-associated gram-negative bacilli in adult and pediatric patients. The distribution was generally similar in the two age groups, with statistically significant differences found only in the proportion of E. coli (higher in pediatric patients) and K. pneumoniae (higher in adults). Table 2 shows that the distribution of species differed somewhat by region as well, with Latin America and North America showing lower rates of E. coli, whereas Africa and North America had higher rates of Pseudomonas aeruginosa than the other regions.
Statistically significant difference in proportion of species in adult versus pediatric patients (Fisher exact test; p<0.05).
The ESBL rates are shown in Figures 1 and 2, as well as Table 3. Overall, 16.3% of E. coli, K. pneumoniae, K. oxytoca, and P. mirabilis were ESBL-positive, the rate ranging from 2.2% for P. mirabilis to 20.1% for K. pneumoniae. Rates generally were higher in adults than in pediatric patients, although this difference was statistically significant only in E. coli (18.2% vs. 11.6%, respectively), as well as overall because of the large proportion of isolates from this species (17.7% vs. 11.4%, respectively). Sample sizes were small for K. pneumoniae in pediatric patients and K. oxytoca and P. mirabilis in all patients, resulting in unstable point estimates and large confidence intervals (Fig. 1).
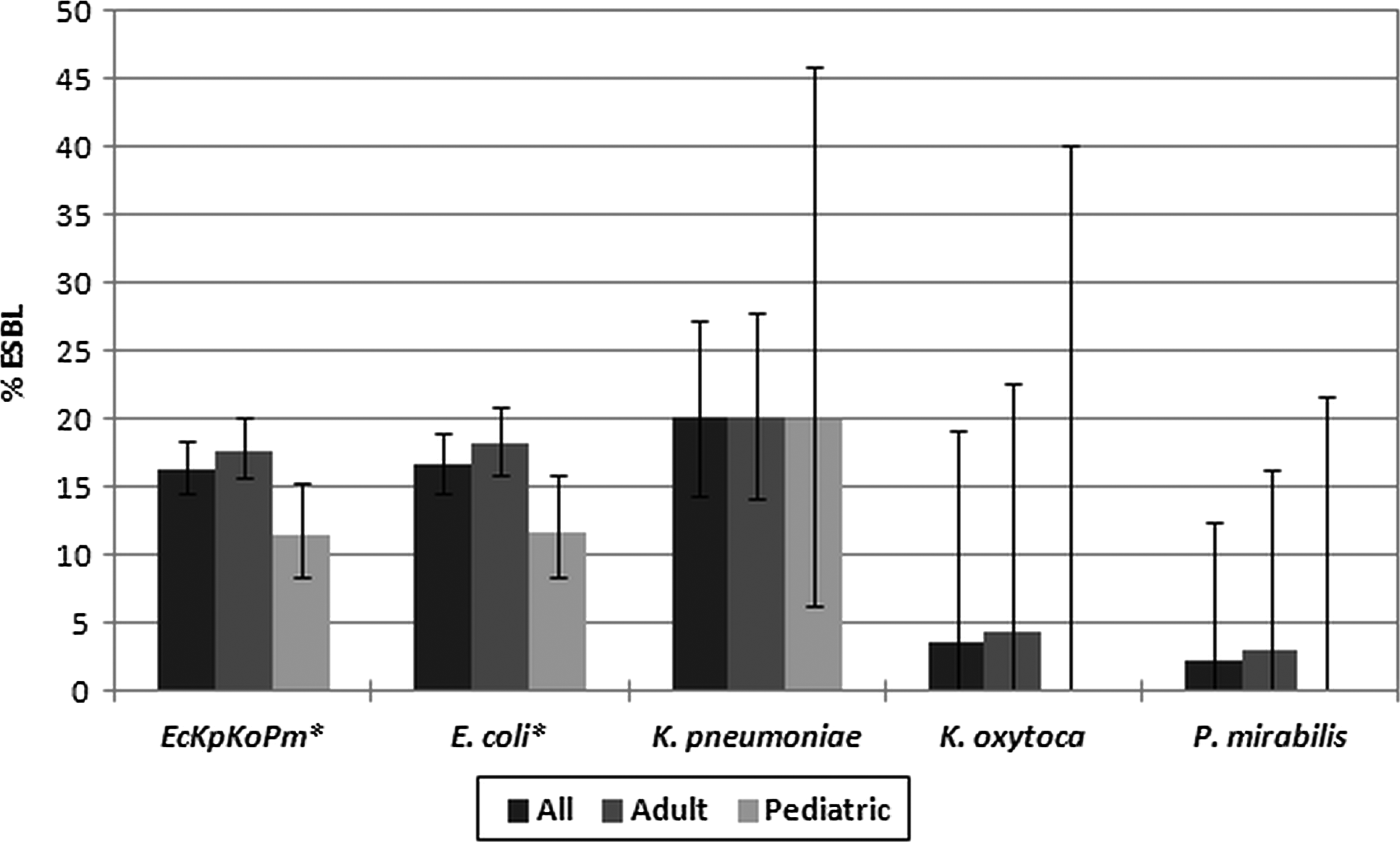
Proportion of extended-spectrum β-lactamase (ESBL)-positive isolates by bacterial species and patient age group with 95% confidence intervals. *Percent of ESBL-positive isolates significantly higher in adult than in pediatric patients (p<0.05; Fisher exact test). Sample sizes: all/adult/pediatric=1,425/1,101/324 (Escherichia coli, Klebsiella pneumoniae, Klebsiella oxytoca, Proteus mirabilis combined [EcKpKoPm]); 1,202/910/292 (E. coli); 149/134/15 (K. pneumoniae); 28/23/5 (K. oxytoca); 46/34/12 (P. mirabilis).
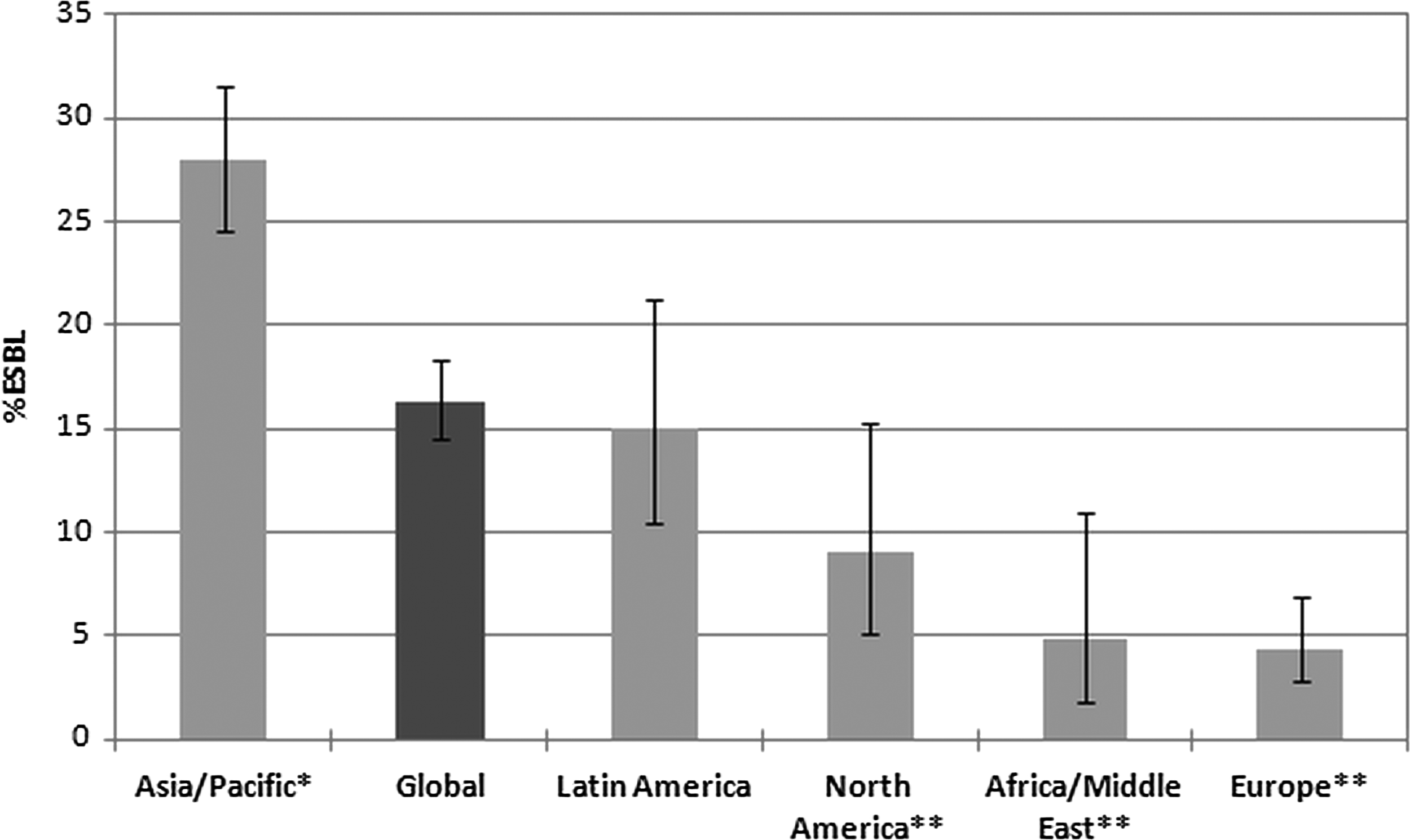
Proportion of extended-spectrum β-lactamase (ESBL)-positive isolates with 95% confidence intervals among Escherichia coli, Klebsiella pneumoniae, K. oxytoca, and Proteus mirabilis combined, by global region. *%ESBL-positive significantly higher than average of the other regions combined (p<0.05; Fisher exact test). **%ESBL-positive significantly lower than the average of the other regions combined (p<0.05; Fisher exact test). n=1,425 (global), 104 (Africa/Middle East), 615 (Asia/Pacific), 408 (Europe), 166 (Latin America), 132 (North America). Note: 2010 data for Asia/Pacific exclude India, from which isolates were not available.
Rates of ESBL-producing isolates also differed by geographic region, with Asia/Pacific showing a significantly higher rate (28.0% for E. coli, K. pneumoniae, K. oxytoca, and P. mirabilis combined) than all other regions combined, whereas North America (9.1%), Africa/Middle East (4.8%), and Europe (4.4%) showed significantly lower rates (Fig. 2).
Table 3 provides a more detailed analysis of ESBL rates by subgroup of the isolates, comparing them with isolates from non-appendicitis IAI. Despite wide confidence intervals in the appendicitis isolates, certain trends were apparent. Generally, the proportion of ESBL-positive isolates was lower in pediatric patients than in adults in all regions, as well as lower in appendicitis-related strains than in non-appendicitis IAI. Only in North America was the point estimate for % ESBL in adults higher in appendicitis than in non-appendicitis IAI (11.0% vs. 6.9%, respectively). However, the confidence intervals for this region were wide, ranging from 6.3% to 18.4%.
Table 4 describes the susceptibility for the 10 most commonly isolated species associated with appendicitis in adult and pediatric patients. Amikacin, imipenem-cilastatin piperacillin-tazobactam, and ertapenem were the most active of the tested agents against most of the aerobic gram-negative appendicitis pathogens, with the two carbapenems and the aminoglycoside performing particularly well against ESBL-positive isolates. These four agents were similarly active in vitro in adults and pediatric patients against E. coli, the most commonly isolated pathogen, whereas most other agents showed significantly lower activity in adults. Piperacillin-tazobactam demonstrated significantly lower activity against P. aeruginosa in adults than in pediatric patients. For all other species, the differences in susceptibility between adult and pediatric isolates were not statistically significant. Amikacin, cefepime, ceftazidime, and imipenem-cilastatin inhibited ≥90% of P. aeruginosa isolates in both adult and pediatric patients. The fluoroquinolones demonstrated activity ≥90% in the adult population only, whereas piperacillin-tazobactam showed 89% activity in adults and 100% in children. Results also are shown for the 10 most commonly isolated species combined, using species-specific breakpoints and assuming zero susceptibility if breakpoints are not defined. Again, amikacin, imipenem-cilastatin, piperacillin-tazobactam, and ertapenem showed the highest in vitro activity in both adult and pediatric patients. Cefepime and ceftazidime also performed well in vitro against pediatric isolates.
Percent susceptible according to Clinical and Laboratory Standards Institute M100-S22 breakpoints.
Percent susceptible significantly lower in adult than pediatric patients (p<0.05; Fisher exact test).
For n<10, n (susceptible)/n is shown instead of % susceptible.
Using species-specific breakpoints and assuming 0% susceptible if breakpoints are not defined.
Ak=amikacin; AS=ampicillin-sulbactam; Cax=ceftriaxone; Caz=ceftazidime; Cft=cefotaxime; Cfx=cefoxitin; Cp=ciprofloxacin; Cpe=cefepime; ESBL=extended-spectrum β-lactamase; Etp=ertapenem; Imp=imipenem-cilastatin; Lvx=levofloxacin; ND=breakpoint not defined; PT=piperacillin-tazobactam.
Susceptibility of the appendicitis-associated pathogens differed by global region. Table 5 shows regional percent susceptible for the 10 most common species for adult and pediatric patients combined. Isolates from Asia/Pacific showed susceptibilities around 10 percentage points lower than the global average for most of the studied cephalosporins, whereas Latin American isolates showed reduced susceptibility for cephalosporins (especially cefoxitin) and the fluoroquinolones. Isolates from Africa/Middle East and Europe, on the other hand, demonstrated markedly higher percent susceptibilities for some of the tested agents. Only amikacin, ertapenem, imipenem-cilastatin, and piperacillin-tazobactam did not differ by more than 10% in any of the global regions.
Percent susceptible according to Clinical and Laboratory Standards Institute M100-S22 breakpoints.
Using species-specific breakpoints and assuming 0% susceptible if breakpoints are not defined.
Ak=amikacin; AS=ampicillin-sulbactam; Cax=ceftriaxone; Caz=ceftazidime; Cft=cefotaxime; Cfx=cefoxitin; Cp=ciprofloxacin; Cpe=cefepime; Etp=ertapenem; Imp=imipenem-cilastatin; Lvx=levofloxacin; PT=piperacillin-tazobactam.
Discussion
Overall, the distribution of aerobic gram-negative bacilli in our study was similar to that reported by Goldstein and Snydman in a review article, with E. coli making up most of the isolates followed by K. pneumoniae, P. aeruginosa, and E. cloacae [8]. The distribution did not differ greatly between adult and pediatric patients or across regions, with E. coli comprising by far the most commonly isolated species, followed by K. pneumoniae and P. aeruginosa, which ranked a distant second or third depending on the age group and region.
Regional rates of ESBL-producing Enterobacteriaceae in IAI can differ widely, as reported in a recent poster presented by Badal et al. at the European Congress of Clinical Microbiology and Infectious Diseases [9]. Our data substantiate this view, showing rates ranging from 4% in Europe to 28% in Asia/Pacific. Comparing our appendicitis-only results with the overall IAI data presented by Badal et al., we found that ESBL rates in appendicitis generally were lower than in IAI overall in all regions except North America. Consequently, the regional ESBL rates were analyzed in more detail, comparing adult and pediatric rates in appendicitis-related infection as well as in all non-appendicitis-related IAI combined. These analyses suggested that lower ESBL rates in appendicitis were largely secondary to a higher proportion of isolates coming from pediatric patients (for whom ESBL rates were markedly lower), as well as to lower ESBL rates in adults with appendicitis compared with those having non-appendicitis IAI. This finding likely is attributable to the fact that appendicitis-associated pathogens generally come from normal bowel flora and therefore do not reflect the higher ESBL rates often found in healthcare-associated IAI [10].
Our in vitro data suggest that amikacin, imipenem-cilastatin piperacillin-tazobactam, and ertapenem would perform well against appendicitis-associated aerobic gram-negative bacilli, especially in regions with high rates of ESBL-positive E. coli. Percent susceptible values for these four agents were around 90% or higher for the 10 most common species combined. All of these, with the exception of amikacin, are included in the IDSA/SIS recommendations [4]. Although ertapenem is not active against P. aeruginosa, this organism accounted for only 7% of isolates from adult patients and 10% of pediatric strains. Cefepime and ceftazidime exhibited good in vitro activity against global pediatric isolates. Regional differences in susceptibility appeared to be driven at least partly by differences in ESBL rates. Asia/Pacific's lower susceptibility correlated with the high ESBL rates in this region, whereas Latin America's lower susceptibility probably is related to both the ESBL and P. aeruginosa rates being relatively high.
Surveillance data, such as those reported here, are important, as appendicitis-related antibiotic prophylaxis needs to be initiated before microbiological culture results are available. Furthermore, routine intra-operative culture swabs are questioned by many, and even regarded as a waste of resources, as several studies found that changes in antibiotic regime based on intra-operative culture results usually made little difference in clinical outcome [11–13]. This makes it all the more important for practicing physicians to be familiar with the general epidemiology of appendicitis-related infections, as well as with current regional and local susceptibility patterns to guide antibiotic choice in patients with appendicitis.
Footnotes
Acknowledgments and Author Disclosure Statement
The SMART program is funded by Merck Research Laboratories, Inc. The authors thank all the participants in the SMART program for their continuing contributions to its success.
Dr. Lob, Mr. Badal, Dr. Bouchillon, Dr. Hawser, Dr. Hackel, and Dr. Hoban are all employed by IHMA, Inc., which receives funding from Merck & Co., Inc., to manage and conduct the SMART program.