
Abstract
Abstract
Background:
Although C-reactive protein (CRP) has proved useful in the assessment of post-operative infections, its value at those time points useful to assess organ-space surgical site infection (OSI) after open and laparoscopic colorectal surgery has not been clarified.
Methods:
We compared values of CRP on post-operative days two and five and percentage of change between those days (Δ%D2–5) in patients with and without OSI, after open (OPEN) and laparoscopic (LAP) colo-rectal surgery. Receiver-operating characteristic analysis was performed and indices of test performance of sensitivity, specificity, positive (PPV) and negative (NPV) predictive values, and likelihood ratios (LR+ and LR-) were assessed.
Results:
The best CRP predictive values for OSI were D5 >120 mg/L (area under the curve [AUC] 0.959; 95% confidence interval [CI] 0.890-0.990) and Δ%D2–5 <40% (AUC 0.968; 95% CI 0.901-0.994; p=0.0001) in OPEN and D5 >66 mg/L (AUC 0.921; 95% CI 0.841-0.969) and Δ%D2–5 <48% (AUC 0.894-95% CI 0.806-0.952; p=0.0001) in LAP. The best measure was NPV (100%; CI 93.6%-100% for D5 and Δ%D2–5 in OPEN and 98.4%, CI 91.3%-99.7% for D5 and 100%, CI 93.4%-100% for Δ%D2–5 in LAP).
Conclusions:
In patients with CRP <120.66 mg/L on post-operative day 5 or a decay from post-operative day two to five of >40%–48% in OPEN and LAP, respectively, OSI may be ruled out and the patient discharged safely. Careful workup is needed in those patients with higher postoperative CRP concentrations or lower apparent decay values.
The post-operative clinical course is assessed daily by physical examination and the main parameters of the systemic inflammatory response (SIRS) such as temperature, heart and respiratory rates, and white blood cell (WBC) count. However, the lack of expression of some SIRS parameters after major trauma [20] or surgery [21] may complicate the diagnosis of post-operative infectious complications, delaying appropriate treatment.
C-reactive protein (CRP) is an interleukin-6-dependent acute-phase protein produced by the liver. Major CRP responses have been observed in bacterial, viral, and fungal infections; inflammatory diseases; myocardial infarction; severe pancreatitis; trauma; and neoplastic disease. The serum CRP concentration is highly dependent on the synthesis rate [22] and the intensity and duration of the inflammatory stimulus.
The time to the peak CRP concentration has been correlated with the magnitude of primary elicited signal. The value peaks by post-operative day two after bone fracture [23] and spine [24] and abdominal surgery [3,10,12,14,25]. In more stressful conditions, the CRP concentration peaks later, by post-operative day three in pancreatic surgery [21] and day four in severe trauma [20]. After elective colorectal surgery, there is agreement that the CRP concentration peak is achieved by post-operative day 2 [10,12,14] even after laparoscopic procedures [3].
Although CRP has been assessed in the diagnosis of severe post-operative surgical site infections after orthopedic [24,26], pancreatic [21], and colo-rectal surgery [10,12,14,27], it has not been defined clearly at which time points the expression of CRP might be useful in the assessment of OSI. We conducted a prospective observational study to clarify the value of CRP on post-operative days two and five in patients submitted to elective colorectal surgery by open (OPEN) and laparoscopic (LAP) access.
Patients and Methods
Study subjects
Consecutive patients older than 18 years of age submitted to elective OPEN or LAP colorectal surgery involving intestinal anastomosis were included. Patients in whom no intestinal anastomosis was made or those patients with an active infection confirmed at operation were excluded.
Study design
To evaluate the usefulness of CRP in predicting OSI infections after elective OPEN or LAP colorectal surgery, we measured CRP before the operation and on post-operative days two and five. The CRP concentration was determined by immunoturbimetric assay (COBAS INTEGRA 400, Roche Diagnostics, Indianapolis, IN; reactants Tina-quant CRP N° 1 859 (Boehringer Mannheim, Ridgefield, CT). Normal values were defined as <5 mg/L.
On the day of the operation, we also recorded the American Society of Anesthesiologists score, Charlson co-morbidity index, duration of operation, main diagnosis, and access (OPEN or LAP). In patients with colorectal cancer, the Tumor–Nodes–Metastasis (TNM) stage also was recorded.
The primary outcome of interest was OSI within 30 d after operation. The research team assessed the clinical notes and the laboratory and microbiologic data for each patient daily. Specifically, SIRS parameters such heart rate, ventilatory rate, oral temperature, and WBC count were recorded at post-operative days two and five and tabulated as recommended elsewhere [28]. Also, the clinical course was discussed daily with the attending surgeon. Post-operative infections were recorded as defined by the U.S. Centers for Disease Control and Prevention [29]. We recorded the day of post-operative complication and if re-operation was done. Prospective data collection ended when the diagnosis and treatment of the post-operative complication was completed (complicated infection) or when patients were discharged from the hospital (no complication).
Sample size calculation
Estimated sample size has been calculated with a power of 0.8 and statistical significance at p<0.05 (one-tailed distribution). We estimated prospectively that the differences between patients without and with OSI regarding the CRP value by post-operative day five would be 0.8 times the standard error of the CRP determinations given a minimum of 20 patients with OSI. The initially estimated rate of OSI was 5%, meaning a sample size of 400 patients (380 without complications) would be needed. Nevertheless, as the interim analysis revealed a higher proportion of patients with complications, the necessary total sample size was reduced to 200 or more patients.
Analysis of data
The values of CRP were compared between the group of patients with OSI and the group with uneventful outcomes or in whom minor infections and non-infections post-operative complications were detected (Non-OSI). Statistical analysis was performed with Medcalc for Windows XP (ScqMed, Chicago, IL). For quantitative variables, the mean (±standard deviation [SD]) was used when the distribution was considered normal; otherwise, the median and range were used. Categorical variables are reported as absolute numbers and percentages. To analyze the data statistically for comparison of continuous variables in OSI and Non-OSI patients, the parametric Student t-test or repeated measurements analysis of variance were used. Analysis of nominal variables between groups was performed by applying the χ2 test. We also determined the optimal cutoff point, sensitivity, specificity, positive (PPV) and negative (NPV) predictive values, and likelihood positive (LR+) and negative (LR−) ratios of absolute CRP values on post-operative day two (D2) and D5, and the percentage of change between post-operative days two and five in absolute (ΔD2–5) and percentage values (Δ%D2–5) by performing the receiver operating characteristic (ROC) analysis. The results of the statistical test are given, whenever possible, with a confidence interval (CI) of 95% as recommended elsewhere [30]. A value of p<0.05 was considered statistically significant.
Results
From January 2007 to September 2009 (19 mo), 208 patients were enrolled. The main diagnosis leading to surgery was colo-rectal cancer (89.9% of patients). Fifty percent of operations were LAP. The most frequent TNM stages were I (17.6%), II (33.2%), and III (38%) (Table 1). In 98% of patients, adequate and on-time antibiotic prophylaxis was documented.
Values are given as n (%) or mean±standard deviation unless otherwise indicated.
ASA=American Society of Anesthesiologists.
Ninety-seven patients (46.6%) suffered at least one post-operative complication. Thirty-eight patients had OSIs (24 in the OPEN and 14 in the LAP group) (Table 2). The median (range) of day of diagnosis was 6 (2–28) days. In the group of patients with OSI diagnosed before post-operative day 5 (26.3%), at post-operative day two, only 44% had SIRS (10% with fever and 20% with WBC criteria). In those in whom OSI was diagnosed between post-operative days 5–10, at D5, only 52% had SIRS (16% with fever and 16.7% with WBC criteria).
A computed tomography (CT) scan in 30 and one ultrasonogram were performed in the patients with OSI diagnosed clinically in the remaining seven cases, three of them at the time of re-operation (Table 3). In four patients (8.3%), OSI was diagnosed clinically, two by spontaneous drainage by rectum and two because the surgeon suspected OSI. In those patients identified before post-operative day five and between post-operative days 5 and 10, a CT scan was ordered after a mean of 3.5±0.92 and 7.3±2.8 post-operative days, respectively. The diagnosis of deep incisional surgical site infection was made clinically for nine of 10 patients. The overall rate of re-operation was 10.1%.
There were three postoperative deaths because of early cardiorespiratory failure. At 30 days, no deaths related to OSI were detected, but one patient died on post-operative day 34.
Assessment of groups
We determined the values of CRP between patients having OSI and the group of those having an uneventful outcome or patients with infections and non-infections minor complications (Non-OSI). Nine patients who suffered clinically evident complications such as cardiorespiratory failure (five patients and three deaths before post-operative day five), two patients with pneumonia and one episode of catheter-related sepsis (both diagnosed before post-operative day five), and a single episode of lumbar puncture diskitis were excluded from the final analysis. In Table 4, we present the baseline parameters of the main study groups. Also, because of post-operative infectious complications requiring specific treatment, data from the point of study at which the treatment was started have not been included in the final analysis. Then, 10 patients found to have OSI before post-operative day five have not been included in the final analysis of the D5-based predictive model.
ASA=American Society of Anesthesiologists; CRP=C-reactive protein; LAP=laparoscopic surgery; OPEN=open surgery; SD=standard deviation.
CRP concentrations in patients with and without OSI
C-reactive protein concentration protein was determined at post-operative days zero, two, and five and Δ%D2–5 was calculated. Patients with OSI had higher concentrations of CRP on both D2 and D5 (Fig. 1 and Table 5). Also, OSI patients showed significantly higher CRP Δ%D2–5 patients without complications in both the OPEN and LAP patients (Table 5). A case-by-case plot of post-operative days two and five CRP values is shown in Figure 2 for the Non-OSI and OSI groups.
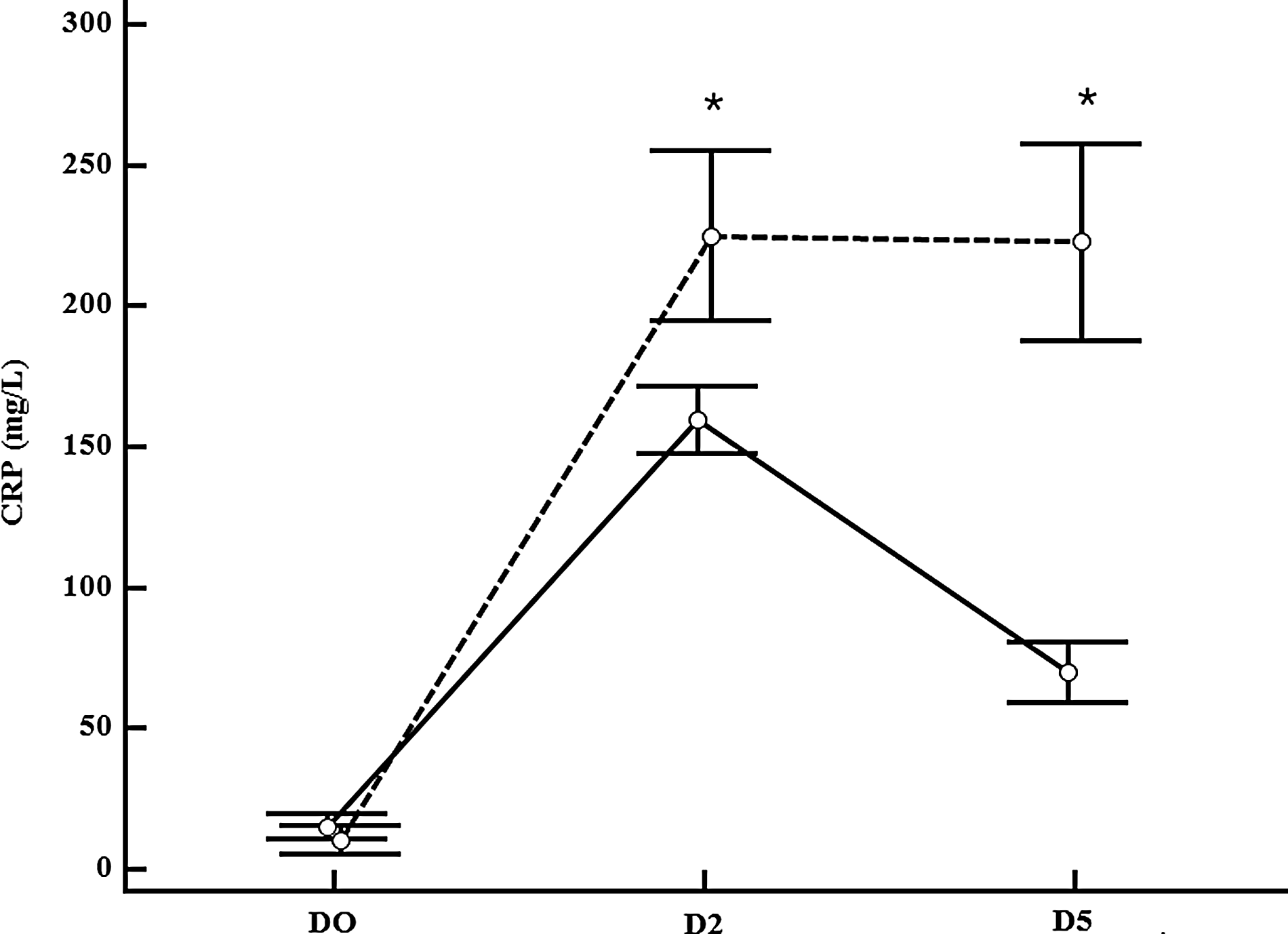
Mean C-reactive protein (CRP) concentrations (95% confidence intervals) at days zero, two, and five of post-operative period in patients with (----) and without (___) organ-space infection (OSI). Concentrations were higher both on D2 and D5 in patients with OSI. *P<0.001 with versus without OSI by analysis of variance.
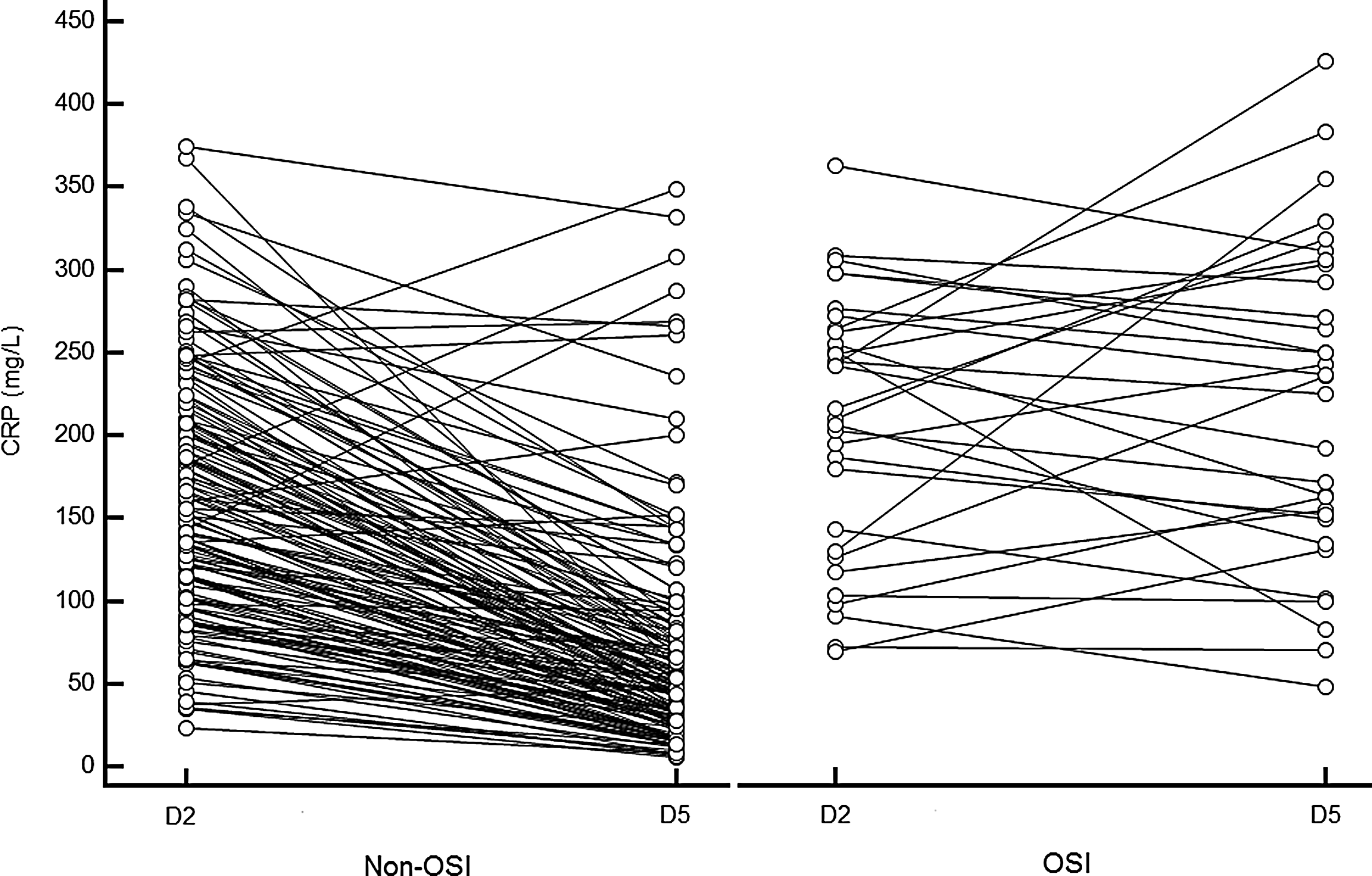
Side-by-side scatter plot, and connecting lines of each individual case showing C-reactive protein value changes from post-operative day two (D2) to day five (D5) in patients without (Non-OSI) and with organ-space infection (OSI).
P<0.01 vs. post-operative day 2 OPEN in Non-OSI.
P<0.0001 vs. post-operative day 5 OPEN Non-OSI.
P<0.0001 vs. post-operative day 2 OPEN.
P<0.05 vs. post-operative day 5 OPEN.
P<0.01 vs. post-operative day 2 LAP Non-OSI.
P<0.0001 vs. post-operative day 5 LAP Non-OSI.
P<0.0001 vs. OPEN Non-OSI.
P<0.0001 vs. LAP Non-OSI.
To assess the best cutoff point for the CRP concentration that better predicted OSI, we performed ROC analysis. Because CRP values at different time points were significantly different depending on the type of surgical access in patients without complications (164±70 and 130±66 on D2, p<0.05 and 53±34 and 41±30 on D5, p=0.05 in the OPEN and LAP groups, respectively), we analyzed OPEN and LAP patients separately. Also, because the AUC of Δ%D2–5 was more accurate than the absolute values of change (AUC 0.919; 95% CI 0.869-0.054 and 0.792-0.900 for Δ%D2–5 and ΔD2–5, respectively; p<0.05) we presented data only for the former.
The cutoff points of CRP that better predicted OSIs were CRP D5 >120 mg/L and Δ%D2–5 <40% decrease in OPEN. In LAP, better predictors were CRP of>66 mg/L on D5 and Δ%D2–5 <48% decrease (Table 6).
Δ%2–5 change in percentage from post-operative days 2–5.
P=0.0001.
P=0.008.
Discussion
CRP in patients with OSI
We have shown significantly higher CRP values on both D2 and D5 in those patients with OSI and a lesser decrease between those days. The early D2 increase in the CRP value in patients with OSI was similar to that in other groups with serious surgical site infections [10,12,14,15]. Nevertheless, we are not able to discriminate if such an early disproportionate CRP response might indicate greater post-operative stress and consequently a higher risk for OSI, or rather is signaling that a post-operative complication is in progress. Also, sustained higher concentrations of CRP on D5 have been observed in patients who ultimately were found to have OSI. Accordingly, the “natural” CRP decay (Δ%D2–5) documented in patients without complications (see Table 5) was positive in OSI patients. Then, because the diagnosis of OSI in a relevant proportion of patients usually is made after post-operative D5, ranging from D6 to D17 [5,6,10,12,14,15,18,31,32] (74% in the present study), the prediction model employing values of D5 or Δ%D2–5 might be helpful. Also, values of CRP during the post-operative period might be helpful in view of the fact that fewer than one-half of the patients with OSI expressed SIRS criteria.
ROC analysis and prediction capacity of post-operative CRP in OSI
To clarify the usefulness of CRP on post-operative days two and five and the concentrations change between these days (Δ%D2–5) we performed ROC analysis. Also, because the CRP response was significantly different depending on the type of access for surgery, OPEN and LAP patients were assessed separately.
The prediction model that includes data from D5 (CRP value of D5 or Δ%D2–5) was better than the model employing D2 data. After moderate trauma, the CRP concentration peaks at 48 h, the time in which we performed the first CRP determination. Then, when an early disproportionate CRP response is observed, it probably is signaling the magnitude of the surgical trauma along with the host`s capacity to produce CRP rather than a developing post-operative complication. Consequently, we are not able to discriminate the meaning of this high CRP cutoff value. Nevertheless, this early high CRP response might suggest that the patient is at risk for post-operative complications by eliciting others as poorly clarified risk factors. Additionally, we have observed that the predicted capacity Δ%D2–5 was superior to the absolute change values. Studies in the critical care area have demonstrated better predictive ability by employing the difference of CRP values from the peak level to the admission [33]. A plausible hypothesis is that a decrease of a given absolute value of CRP might have a different biological meaning when CRP is much higher on D2.
In this specific prediction model of post-operative OSI, the NPV was superior to the PPV. As the prevalence of the effect is relatively low, the PPV follows accordingly reinforcing the value of NPV [34]. Also, because this model has been constructed with a group of patients with Non-OSI that includes patients with no complications along with patients with other minor complications that are able to elicit a CRP response (Table 6), PPV may be underpowered by these less relevant but also inflammatory complications. Otherwise, NPV of all cutoff points tested was the better index of test performance, being higher than those constructed with D5 data. Then, almost 100% of patients with CRP concentrations <120 mg/L—or a higher decay from D2 than 40%—in OPEN and less than 66 mg/L—or higher decay than 48% from D2—in LAP, might be candidates for safe hospital discharge.
Also, this study gives some novel data regarding the different inflammatory response depending on the type of surgical access. Although there has been some work on the CRP response in post-operative complications after elective colo-rectal surgery, CRP data on the OSI-elicited response depending on the type of access for surgery is lacking. Although other factors might influence the host's CRP response, access surgery is a clearly demonstrated factor. Then, compared with the OPEN group, the cutoff point for predicting OSI has been set in LAP patients as <22.5% on D2 and 45% on D5. Less apparent differences were seen regarding the Δ%D2–5 and probably are related to the wider 95% CIs.
It is well known that a relevant number of OSIs begin with misleading findings such as post-operative ileus. In the present study, the average CRP on D5 in those patients with post-operative ileus was 68±60 mg/L, one-third that of those patients with OSI (data not presented). Also, the authors are aware that this CRP-derived predictive model of OSI complications might be useful only for this specific patient population with the same risk factor distribution. In a bivariable analysis in patients without complications and adjusted for the type of surgical access, we were not able to demonstrate a conclusive relation with risk factors such age, American Society of Anesthesiologists score, Charlson score, TNM, duration of surgery, or basal CRP.
Postoperative OSI
In the present study, we observed a 18.3% rate of OSI. Although these figures are higher than the desired rates published by national agencies [35] or those found in prospective [4] and retrospective [1–3,5,9,10,18,36] studies, a higher frequency of post-operative OSI after colo-rectal surgery has been found in prospective [14,15,37] or large epidemiologic studies [38]. Also, in the present study, OSI was diagnosed by applying only clinical criteria in some cases [29]. Thus, the application of such a strict protocol might have contributed to the documented high post-operative OSI rate. We have observed that OSIs correlate with Charlson score and the duration of the surgical procedure. OPEN surgery also has been correlated with surgical site infections. Nevertheless, this was a non-randomized study, and the LAP technique was introduced progressively and applied selectively. The patients operated by OPEN were older and sicker and had a more advanced colo-rectal tumor stage.
We did not observe the 30-day post-operative mortality for this study. An OSI is the main cause of death after colo-rectal surgery [31]. The post-operative mortality rate in the presence of OSI ranges from 1.3% to 37% [1,6,9,18,19,39]. Although a higher OSI-related mortality rate has been observed after rectal surgery [9,18], non-elective colorectal cases [6], and in the presence of post-operative diffuse peritonitis [19], prognostic factors after OSI have been studied to only a small degree. For instance, it has been observed that patients with OSI who were operated on again before post-operative day five displayed a significantly better prognosis [1]. In the present study, several factors might have contributed to the low mortality rate in patients with OSI. First, only two patients in the overall study were classified as having severe sepsis by the time the diagnosis of OSI was made (data not shown). Also, because this study was not blinded for the responsible surgical team, disproportionate high concentrations of CRP might have alerted the surgeons, precipitating closer post-operative observation. Consequently, the initial steps of treatment of intra-abdominal sepsis—intravenous fluids and empirical antibiotic treatment—were initiated more quickly. Although we did not include the 30-d post-operative mortality rate in the trial statistics, the time delay to re-operation was six days, in the range seen in previously published studies [13,14]. Then, although some authors have found a lower mortality rate in patients operated on again before D5 [1], we were not able to corroborate this finding. For instance, patients with OSI diagnosed before D5 were those with more clinically apparent sepsis (more SIRS criteria and higher CRP values). As a consequence, 70% of such patients with early complications required an expeditious focus control in contrast to patients with late complications, of whom only 30% underwent re-operation. We hypothesize that the prognosis of OSI probably is related more to the early diagnosis, prompt antibiotic treatment, and judicious and timely focus control.
Conclusions
Low post-operative CRP concentrations and more rapid decay from D2 to D5 are useful in predicting a post-operative course without OSI. Patients with elevated or insufficient CRP decay deserve close attention. Also, concentrations of CRP during the post-operative period should take into account the type of access for surgery.
Footnotes
Acknowledgments
The authors thank the members of the colorectal surgery unit of Hospital General de Granollers, Doctors A. Ibañez, J. Montero, A. Gaspar, D. Ribé, and R. Hernando, the nurses L. Molero and O. Silva, and the assistant nurses of the Department of Surgery and the Laboratory Department for the CRP analysis.
Author Disclosure Statement and Research Support
The authors declare no conflict of interest. No funding has been employed for this research.