
Abstract
Abstract
Background:
The high prevalence of surgical site infection (SSI) in colon surgery, and the clinical and economic impacts of such infections, make its monitoring and prevention a priority.
Methods:
We conducted a prospective cohort study to estimate the rate of SSI in colon surgery and the degree of compliance with antibiotic prophylaxis and pre-operative preparation protocols. The study population comprised patients who underwent colon surgery at the University Hospital of the Alcorcon Foundation in Alcorcon, Spain, from October 2007 to December 2009. Risk factors, the observance of antibiotic prophylaxis, and compliance with pre-operative preparation protocols were monitored; and their influence on SSIs was followed for 30 days after surgery. The main outcome measure was comparisons of the rates of SSI in patients undergoing colon surgery in Madrid and across the whole of Spain and in the United States, as determined in accordance with the surveillance parameters of the National Nosocomial Infections Surveillance (NNIS) index.
Results:
Among a total of 132 patients, we found a 10.6% rate of SSI. The indirect standardization rate at our hospital was 1.75-fold for the United States and 0.64-fold and 0.61-fold, respectively, the rates for Madrid and all of Spain. The rates of compliance with antibiotic prophylaxis and pre-operative preparation protocols were 93.6% and 56.8%, respectively. No relation could be established between these data and the rate of infection. The risk factors for SSI found in a multivariable analysis were the degree of contamination in surgery and the presence of chronic obstructive pulmonary disease (COPD; p<0.05).
Conclusions:
The rate of SSI in our study population was below that for Madrid and Spain but higher than that for the United States. Thorough adherence to the monitoring system was essential for obtaining these results.
Diseases of the colon are common among the general population, and their treatment carries a high risk of SSI that increases both the morbidity and mortality rates of treatment [3]. The rate of SSI in colon surgery in the United States was 5.6%, according to figures published by the National Healthcare Safety Network (NHSN) for the period from January 2006 to December 2008 [4]. In comparison, the rate of SSI associated with colon surgery in Spain reached 17.4% in 2008 [5], and the rate in the Madrid community in 2009 was 16.7% [6].
Different factors influence the likelihood of a SSI. The three main factors are the degree of contamination during the operation, the general health of the patient, and the duration of the surgical intervention. These are the surveillance parameters used for the National Nosocomial Infection Surveillance (NNIS) index [7], which classifies patients according to their potential risk of infection. However, other risk factors must be taken into account; for example, the quality of the surgical technique, the adequacy of pre-operative preparation, ambient conditions in the surgical theater, adequate sterilization of all material used during surgery, and antibiotic prophylaxis [7,8].
The goal of this study was to estimate the SSI incidence in colon surgery in our area as well as to classify it according to the NNIS index. It also aimed to standardize this incidence rate in order to compare it with the figures of the region of Madrid as well as Spain and the United States. Furthermore, it attempted to assess the extent of observance of pre-operative preparation and antibiotic prophylaxis protocols with the application of a surveillance system, as well as to identify possible risk factors related to the high rate of SSIs among these patients. The benefits of the implementation of a monitoring program that estimates the incidence of SSI are to determine the frequency of NI, detect changes in patterns, identify the micro-organisms involved in SSI, and determine the risk factors for infection. It also provides real-time detection of a potential outbreak. Furthermore, it minimizes the frequency of NI by identifying high-risk patients, facilitating the implementation of specific measures, and ensuring that prevention and control measures are established properly in a cost-effective manner. It standardizes information, allowing its comparison with data from other centers. In addition, it evaluates quality of care programs, thus facilitating continuous improvement.
Patients and Methods
We carried out a prospective cohort study from October 2007 to December 2009 to determine the SSI incidence rate at the Hospital Universitario Fundación Alcorcón (HUFA). All patients in sanitary area VIII of the community of Madrid (reference population, 250,000 inhabitants) who, according to the national health distribution areas, attended HUFA (a medium-size hospital of 450 beds) and had colon surgery for benign or malignant and conditions, according to the terms established by the NNIS system in 2006, were included in the analysis. Among the codified registered procedures were incision, resection, and anastomosis of the large intestine, excluding rectum-related operations. A group of 126 patients were estimated, taking into account a confidence level of 90%, a precision level of 6%, an expected SSI incidence rate of 17.5%, and 10% losses.
The criteria used to define SSI were those of the CDC (Table 1). The Preventive Medicine Service carried out the data collection and the clinical monitoring process, from admission to discharge. Appearance of SSI was determined at least every two days. All data were collected from the patients' clinical records, the corresponding microbiologic cultures, and information obtained from medical personnel and the nurses in charge of the individual patients. Wherever SSI was diagnosed, it was monitored by medical personnel.
Patients were monitored for 30 d after the surgical intervention by regular visits while in the hospital and then by office visits, assessing the incision and the microbiologic cultures. Additionally, any emergency hospital visits were recorded. All data were stored using a monitoring application developed by the Spanish Programme for Clinical Indicators of Continuous Quality Improvement (INCLIMECC).
Pre-operative preparation, antibiotic prophylaxis, and mechanical preparation of the colon were carried out according to the hospital protocol. Measures such as oropharyngeal washes with chlorhexidine gluconate hexetidine 0.12% beginning the day before surgery to prevent early post-operative pneumonia, shower with chlorhexidine soap, and hair removal with clippers the day of surgery were employed to minimize SSI. Mechanical bowel preparation remains controversial, although currently, only patients with rectal disease usually are prepared in this way. During the period of the study, patient preparation was carried out using polyethylene glycol; the combination of 1 g each of erythromycin and neomycin, which were administrated orally at 1
The variables analyzed in the study were gender, age, patient characteristics, surgical procedure codes, elective or emergency surgery, duration of the intervention, surgical risk according to the American Society of Anesthesiologists (ASA) score, the degree of contamination of the surgery, the administration of prophylactic antibiotic, the adequacy of prophylaxis (start, choice, application method, dose, duration), the observance of pre-operative preparation (comprisive chlorhexidine body wash and antiseptic mouthwash 24 h before the operation), and the reasons its application sometimes was inadequate. Procedures were classified according to International Classification of Diseases (ICD)-9-CM categories and the SSI definition criteria, and location was named as defined by the CDC [9].
A descriptive study of the group of patients was carried out to establish their socio-demographic characteristics. Qualitative variables were described with their frequency distribution and compared using the Pearson χ2 test. Wherever the necessary conditions for this test were not present, the Fisher exact test was used instead. The quantitative variables were analyzed using the Student t-test when the figures followed a normal data distribution and the Mann-Whitney U test if not. For quantitative variables in more than two groups, analysis of variance (ANOVA) was used, and when test application conditions were not met, the non-parametric Kruskal–Wallis method was applied.
A multi-variable logistic regression analysis was carried out with the combination of the variables most useful for SSI prediction. The relation between the adequacy of prophylaxis and pre-operative preparation and the SSI rate were studied in terms of relative risk (RR). The program SPSS version 18 (SPSS, Inc., Chicago, IL), was used for statistical interpretation.
Both the global and the stratified infection rates were calculated according to the NNIS index, adding up the ASA classification score, the degree of contamination, and the duration of the intervention (Table 2). The average lengths of preoperative, post-operative, and total lengths of stay in the hospital also were calculated.
Additionally, a comparison with the data from the community of Madrid, as well as with Spanish and U.S. data, was carried out and sorted by risk indexes. For each procedure, the observed rate was computed, as well as the predicted rate, based on the latest figures published by NHSN [4], as well as those of the Spanish national health care-associated infection survillance (INCLIMECC) network [5] with the method of indirect standardization. The ratio between the observed and the predicted rates, the standardized infection ratio, (SIR) was interpreted as the RR. The indirect standardization was calculated with the epidemiologic program Epidat 3.1. (Consellería de Sanidade, Xunta de Galicia, Santiago de Compostela, Spain).
Results
A total of 132 patients were monitored, of which 63% were male and 37% female, with a mean age of 65 years (youngest patient, 15 year). The patient characteristics, diagnosis, and surgical procedures are included in Table 3. Twenty-two percent of patients were operated on for benign conditions.
A total of 16% of the patients (n=21) were admitted urgently. Surgery could be delayed for a few days in some of these patients, which meant that they could follow the protocol, whereas the others had to undergo surgery at the time of admission. Of this last group of patients, none completed the preparation protocol.
According to the ICD-9 classification, the most frequent surgical procedures were right hemicolectomy (31%) and sigmoidectomy (28%), followed by left hemicolectomy (11%) and colostomy closure (10%). Only 20% of the operations were carried out by laparoscopy.
Patients were classified using the infection risk index (NNIS): 6.1% (n=8) of patients were NNIS 0, 31.8% (n=42) NNIS 1, 48.5% (n=64) NNIS 2, and 13.6% (n=18) NNIS 3.
The globally accumulated SSI incidence was 10.6% (95% confidence interval [CI] 5.6–15.6; 14 infections) and the incidence density 0.0077 infections/patient/day. The rate of infection classified by depth was 4.6% (95% CI 0–10; 6 cases) superficial incisional, 3% (95% CI 0–9; 4 cases) deep incisional, and 3% (95% CI 0–9; 4 cases) organ/space. The SSI incidence increased in parallel with the NNIS index (Fig. 1).

Incidence of surgical site infection according to National Nosocomial Infection Surveillance (NNIS) risk index.
The infections were polymicrobial. The individual micro-organisms, in order of frequency, were Escherichia coli, Enterococcus faecium, E. faecalis, and Morganella morganii. Found less frequently were Bacteroides fragilis, Enterobacter cloacae, Proteus mirabilis, P. vulgaris, Pseudomonas aeruginosa, Staphylococcus aureus, S. epidermidis, and S. haemolyticus.
In nine of the 14 SSI cases, the surgical time was above the 75th percentile (180 min). There were 54 of 118 “no SSI” with surgical time higher than 75th percentile (Fig. 2). The univariable analysis showed that the contamination grade is an SSI risk factor (p<0.05). The other variables studied as potential SSI risk factors lacked any statistical relevance. The multi-variable analysis showed that the only predictive factors were chronic obstructive pulmonary disease (COPD) and the contamination grade of the surgical incision.

Surgical site infections in relation to duration of operation. Note: 180 minutes is the 75th percentile for colon surgery.
The rate for SSI in colon surgery at HUFA was 0.61 times lower than that of the INCLIMECC group and 0.64 lower than that in the community of Madrid. Compared with the data published by the NHSN monitoring system of the United States, the global infection rate was 1.75 times higher than expected.
The patients were admitted for bowel preparation 24–48 h before surgery. The average pre-operative hospital stay was 2.9 days. The average total length of stay for patients undergoing colon surgery was 15 days. Patients with SSI had an average length of stay 13.5 days longer than those with no SSI, this difference being related mainly to the post-operative stay (average of 10.8 days for patients with no SSI versus 24.3 days for patients with SSI). The length of stay increased in parallel with the NNIS index, regardless of whether SSIs were present (Table 4). An SSI occurred in 16.3% of patients with a greater than one day length of stay before surgery and in 7.2% of patients who were admitted the day of surgery (p=NS).
SSI=surgical site infection; Preop=pre-operative; Postop=postoperative.
Antibiotic prophylaxis was administered to 100% of monitored patients, although only 126 patients received oral and parenteral prophylaxis. The global adequacy of the antibiotic prophylaxis protocol was 94%, and the main form of inadequate adherence was the choice of antibiotic (n=5), followed by the duration (n=2) and time of initiation (n=2) of treatment.
Preoperative preparation was carried out in 85% of patients (n=112), and the percentage of correctly prepared patients was 56.8%. The most common type of inadequate preparation was omission of antiseptic mouthwash. Only a small percentage of patients did not have a shower with chlorhexidine soap 24 h before surgery, and in some cases, this was not reflected in the clinical records (Fig. 3). No connection between SSIs and either inadequate antibiotic prophylaxis (RR 1.01; 95% CI 0.15–6.86) or incorrect pre-operative preparation (RR 0.88; 95% CI 0.25–3.1) was found.
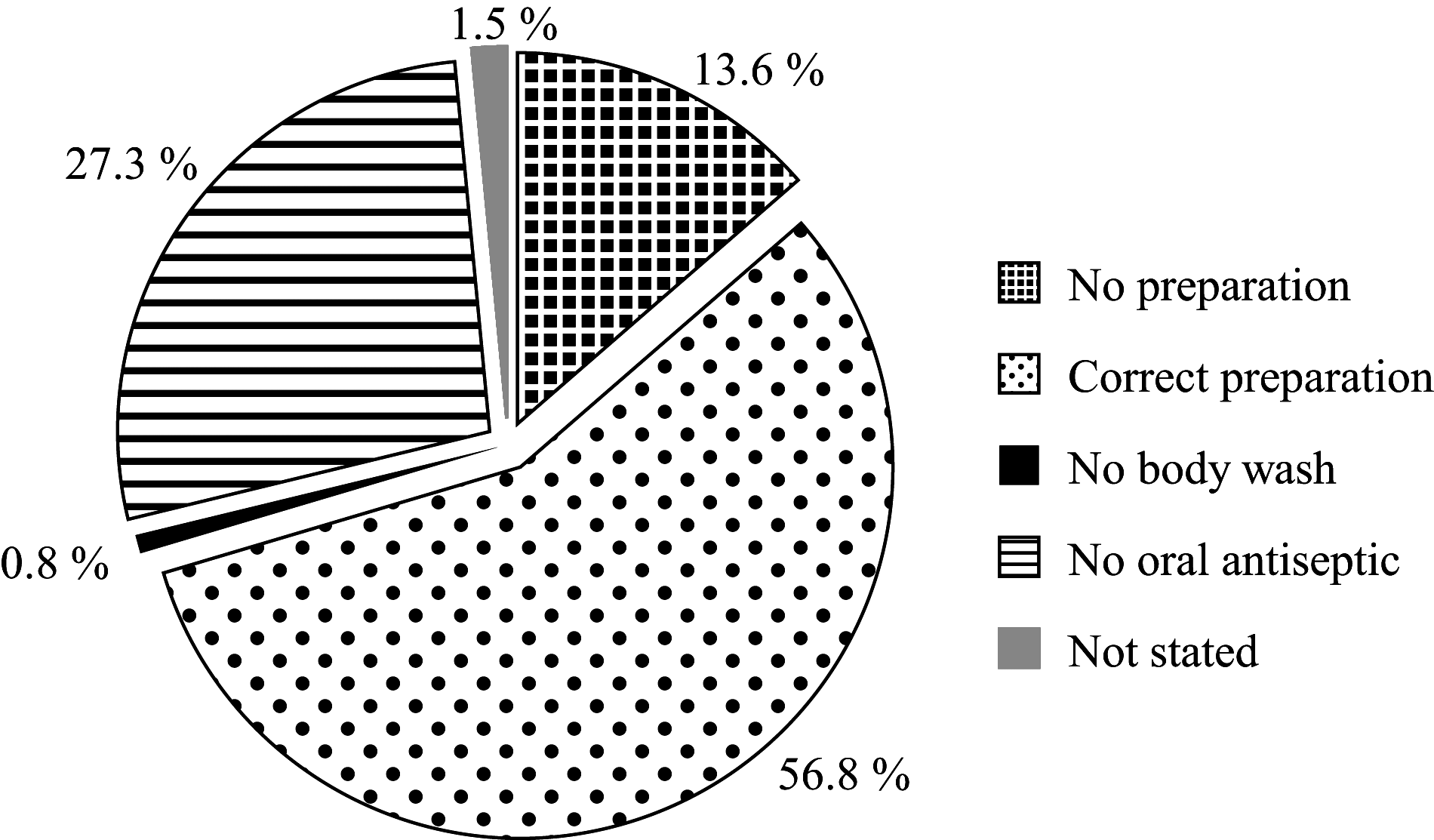
Degree of compliance with pre-operative preparation protocol.
Discussion
The SSI incidence rates in colon surgery at HUFA were within the lower ranges of published series (5%–26%) [10–12]. Using the indirect standardization and the SIR, we analyzed the expected rate, as well as the differences in the infection risk of an individual hospital and compared it with the hospitals of the Spanish INCLIMECC network [5,8], the hospital-acquired infection system of the community of Madrid [6], and the U.S. monitoring system [2,4]. The SSI incidence rate in colon surgery at HUFA for the observation period was 10.6% (n=14), a rate lower than the Spanish national average and also that of the community of Madrid, but higher than the U.S. figure. These results could be secondary to the high degree of observance of pre-operative preparation and chemoprophylactic measures, as well as the close monitoring of the patients. The higher SSI rate than in the NNIS categories was to be expected. The SSI rate in colon surgery of National Surgical Quality Improvement Project (NSQIP) is 9%, also lower than ours. These differences may be secondary to our longer average hospital stay, which leads to more monitoring and data collection on SSI within 30 days after surgery.
However, numerous publications from tertiary-care U.S. hospitals specializing in colorectal disease showed rates well above the NNIS index, even higher than the figures found in this study for HUFA. For example, Smith et al. published a significantly higher SSI figure for colorectal surgery (25.6%) in 2004. This result may be related to the fact that the study was done at a reference center for colorectal surgery, where they perform a large number of low anterior resections (36.9%), stoma creations (40.3%), surgical interventions for inflammatory intestinal disorders (19.9%), and oncologic colorectal operations (57.4%) [12]. Other studies from reputable institutions also published higher rates of SSI in colorectal surgery: 14.3% in the publication from the Cleveland Clinic in 2006 [10] and 19.3% in 491 consecutive patients operated on from April 2006 to July 2008 published by Pastor et al. [11].
The SSI incidence density has been low (0.0077 infections/patient/day) but higher than the rate published by the Preventive Medicine Service of Hospital Reina Sofia of Cordoba, which was 0.0057 infections/patient/day [13]. This difference might be attributable to the fact that in the Cordoba study, only those patients who were re-admitted after discharge or re-operated on were considered, with no data on follow-up of patients in the office after discharge or those who attended emergency services and were treated as outpatients for superficial SSIs. However, at HUFA, this kind of monitoring was carried out thoroughly so as not to underestimate SSI rates. The same is true for other studies that published much lower rates but recorded data only during the hospital stay [3,4]. The incidence of infection rates increased in parallel with the NNIS risk index, an observation that confirms the findings of Culver et al. [14]
The single most common micro-organism was E. coli (42.9%), followed by Enterococcus faecium (28.6%), E. faecalis (21.4%), and Morganella morganii (14.3%). These findings are similar to the results of other studies [15].
The average length of stay in the hospital in HUFA colon surgery patients was below that of the community of Madrid (15 vs. 19 days) [6]. In comparison with the results obtained from other studies in Madrid, pre-operative and post-operative hospital stays were shorter in the HUFA patients [6].
The longer average pre-operative hospital stay in the community of Madrid might well be one of the causes of the higher SSI rate in that group. A number of studies have confirmed that longer pre-operative stays are indeed a risk factor for SSI [16–18]. At the same time, a longer average post-operative stay might be a consequence of the larger number of patients with SSI. There is a direct correlation between patients becoming infected and prolonging their stay in the hospital.
The only intrinsic SSI risk factor was COPD. None of the other factors analyzed; for example, age, gender, body mass index, diabetes mellitus, immunodeficiency, neoplasia, cirrhosis, or renal dysfunction proved to be a risk factor. A variety of factors associated with COPD can influence SSIs, such as steroid treatment, deficient tissue oxygenation, cough, respiratory secretions, and smoking, which is a decisive factor for SSIs in various publications [19,20]. However, given the small sample size and the low incidence of COPD in the population analyzed, we cannot conclude that COPD is an independent risk factor for SSI. Further studies will be needed for this analysis.
Of the possible exogenous SSI risk factors, the only one that could be proved to be of importance was the degree of contamination during surgery. Many authors agree with this assessment. Garibaldi et al. proved that intra-operative contamination leads to a higher probability of SSIs [18]. Tang et al. demonstrated that surgical classification according to the contamination grade was an independent risk factor for the development of an infection and that “contaminated” procedures were associated with 3.8-fold more incisional SSIs than “clean-contaminated” procedures (95% CI 1.6–8.9; p<0.01) [21].
Surgical time exceeding the 75th percentile was more common among patients with SSIs, but this difference was not statistically significant by univariate analysis and could not be confirmed in logistic regression analysis (OR 2.6; 95% CI 0.74–9.10; p>0.05). Some studies have identified surgical duration as an independent variable related to SSI risk [10,14,17,18,22–24], whereas others were not able to prove this [12,21]. Other exogeneous factors such as the surgeon, surgical technique, the surgical theater, emergency surgery, type of surgical approach, preoperative preparation, or antibiotic prophylaxis were not risk factors in our patients.
The HUFA's monitoring system has proved to be adequate for its task. Adequacy of pre-operative preparation has been high for antiseptic showers and slightly worse for mouthwashing. The degree of adequacy was higher than in the community of Madrid [6]. In terms of improvement, it would be advisable to provide thorough information to patients by a specifically trained multi-disciplinary team to guarantee adequate understanding of the importance of pre-operative measures.
Observance of the antibiotic prophylaxis protocols has been excellent. All patients received chemoprophylaxis. The low percentage of patients in whom chemoprophylaxis was inadequate is attributable largely to the choice of antibiotics, followed by the procedural duration and start time. The lack of a statistical relation between inadequate antibiotic prophylaxis or lack of pre-operative preparation and SSI incidence rates might be secondary to the size of the trial group, which was computed primarily to estimate the infection rate.
Other factors that may prevent SSIs in colon surgery are not included in the current monitoring system, such as prevention of blood loss and transfusion, the patient's nutritional state, normoglycemia, normothermia, and peri-operative hyperoxygenation, according to the findings of various studies [10,17,23]. This could be seen as a shortcoming of our study.
In conclusion, the SSI incidence among patients undergoing colon surgery at HUFA lies within the lower limits of the published series and below the figures for the community of Madrid and for Spain as a whole. At the same time, it is higher than U.S. infection rates. We think that the implementation of a monitoring system is beneficial for those centers where it is not currently being carried out, as it does not add excessive cost and has a high probability of being beneficial for the prevention of SSI.
Footnotes
Acknowledgments
We thank the General Surgical and Preventive Medicine Departments of the University Hospital of the Alcorcon Foundation for their collaboration and valuable support for the duration of this project.
Author Disclosure Statement
No competing financial interests exist.