
Abstract
Abstract
Background:
A high rate of surgical site infection (SSI) accompanies the repair of large ventral hernias in the presence of bacterial contamination. Recent clinical and laboratory studies suggest that negative-pressure therapy (NPT) applied to closed surgical incisions may reduce the risk of SSI in high-risk populations. We hypothesized that NPT would reduce the risk of SSI in patients undergoing the repair of contaminated ventral hernias.
Methods:
We reviewed retrospectively our prospectively collected database for patients undergoing repair of potentially contaminated and infected ventral hernias with or without NPT. All of the patients had primary wound closure. In the NPT group, a vacuum dressing was applied over the closed midline wound. The primary outcome measure was SSI at 30 d post-operatively.
Results:
We evaluated 119 patients (70 with a standard wound dressing (SWD) and 49 with NPT). The groups were similar in age, gender, body mass index (BMI), the prevalence of chronic obstructive pulmonary disease (COPD), diabetes mellitus (DM), and smoking; and the number of prior abdominal operations. The SWD group had a higher American Society of Anesthesiologists (ASA) score than did the NPT group (3.0 vs. 2.8; p=0.01). The two groups were similar in the sizes of their hernia defects and duration of surgery, and did not differ in their 30-d rates of SSI (25.8% SWD vs. 20.4% NPT; p=0.50) or in the distribution of major and minor SSIs (SWD: 6 major, 12 minor vs. NPT: 2 major, 8 minor; p=0.56). Factors associated with an increased risk of SSI included ASA score (p=0.02), BMI (p=0.05), defect area (p<0.01), DM (p=0.01), and duration of surgery, (p<0.01).
Conclusions:
This retrospective, non-randomized study found that NPT in the setting of a closed surgical incision after potentially contaminated or infected ventral hernia repair (VHR) did not reduce the incidence of SSI. Although prophylactic NPT has reduced wound morbidity in some surgical populations, it does not appear to offer the same reduction in wound morbidity in high-risk, contaminated, and potentially contaminated open VHR.
Negative-pressure therapy (NPT) has gained popularity rapidly among surgeons for the management of acute and chronic wounds, including dehisced surgical incisions [6,7], flaps and grafts [8,9], open abdominal wounds [10,11], traumatic orthopedic wounds [12,13], and decubitus [14] or diabetic foot ulcers [15,16]. In most of its clinical applications, NPT is applied to an open surgical wound to facilitate closure. More recently, a growing literature has suggested that prophylactic application of a negative-pressure dressing to a closed but at-risk incision reduces the incidence of infection and wound breakdown [17–19]. This so-called well-wound therapy has shown promise in a number of clinical settings. However, there is a paucity of literature discussing the use of NPT for closed abdominal incisions. We hypothesized that prophylactic NPT applied to closed skin incisions following the repair of contaminated ventral hernias would reduce the risk of SSI in this setting.
Patients and Methods
From August 2006 to December 2011, a prospectively collected database was analyzed to select patients with potentially contaminated or contaminated ventral hernias undergoing repair with and without NPT. The surgical repairs in all of the patients were done by one or another of us (M.J.R, Y.W.N.) at a single academic institution and with a similar surgical technique, discussed in the following sections. Exclusion criteria were enterocutaneous or colo-cutaneous fistulae, panniculectomy done simultaneously with hernia repair, and anterior components separation, the latter two of which were excluded from analysis because they have been reported to increase the incidence of SSI. The study was done with institutional review board approval [20].
Records were analyzed for patient demographics including sex, gender increased, comorbidities (smoking, diabetes mellitus [DM] chronic obstructive pulmonary disease [COPD], immunosuppression, steroid use, body mass index [BMI], number of prior abdominal operations, and number of prior ventral hernia repairs. Patients were identified as smokers if they had any history of smoking within the three months before surgery. No patient was smoking actively at the time of his or her operation. Perioperative data included American Society of Anesthesiologists (ASA) Physical Status Classification, defect size, surgical repair technique, and operating-room (OR) time.
Patients followed similar infection prevention protocols throughout their hospitalization, utilizing Surgical Care Improvement Project guidelines. Clippers were used to remove hair from the surgical site before skin preparation with a 2% chlorhexidine gluconate/70% isopropyl alcohol formulation. Weight-based dosing with cefazolin (or vancomycin, in the case of patients with cephalosporin allergy or known methicillin-resistant Staphylococcus aureus infection) was begun within 1 h before skin incision and was continued post-operatively with two further doses, unless an intra-abdominal abscess was identified, in which case the antibiotic treatment was continued for 5 d.
Our approach to open abdominal-wall reconstruction has been reported previously [21]. We prefer a retro-rectus addominis repair with macro-porous synthetic mesh in cases of clean surgical fields, and with non-cross–linked porcine dermis in contaminated fields. In patients with larger defects, we create additional myofascial advancement flaps. Although we utilized endoscopic release of the external oblique muscle previously [22], during the last two years of the study we used a technique of posterior-component separation that releases the transversus abdominis muscle [23,24]. Two closed-suction drains were used in all patients undergoing myofascial advancement. These drains were placed above the implanted mesh, and below the anterior fascial layer of the abdominal wall. The drains were left in position until their output was less than 30 mL over a 24-h period or, for all patients with synthetic mesh, until the time before hospital discharge (typically on post-operative day 7).
Following herniorrhaphy, the skin was closed with staples or an absorbable subcuticular closure. Patients were then given either a standard wound dressing (SWD) or NPT. The SWD was a dry gauze adhesive dressing applied under sterile conditions in the OR. The SWDs were removed on post-operative day 2. The dressings for NPT were also applied under sterile conditions in the OR. These consisted of knitted cellulose impregnated with a petrolatum emulsion (Adaptic; Johnson & Johnson, Piscataway, NJ) and applied over the patient's surgical incision to protect the skin from a strip of reticulated open-cell polyurethane black foam (Granufoam; KCI Licensing, San Antonio, TX) that was secured with adhesive dressings (Fig. 1). Negative-pressure therapy was applied at a continuous pressure of −75 mm Hg for seven days or until the day of the patient's discharge from the hospital. Dressings for NPT that had a high rate of leakage were reinforced or replaced at the bedside.
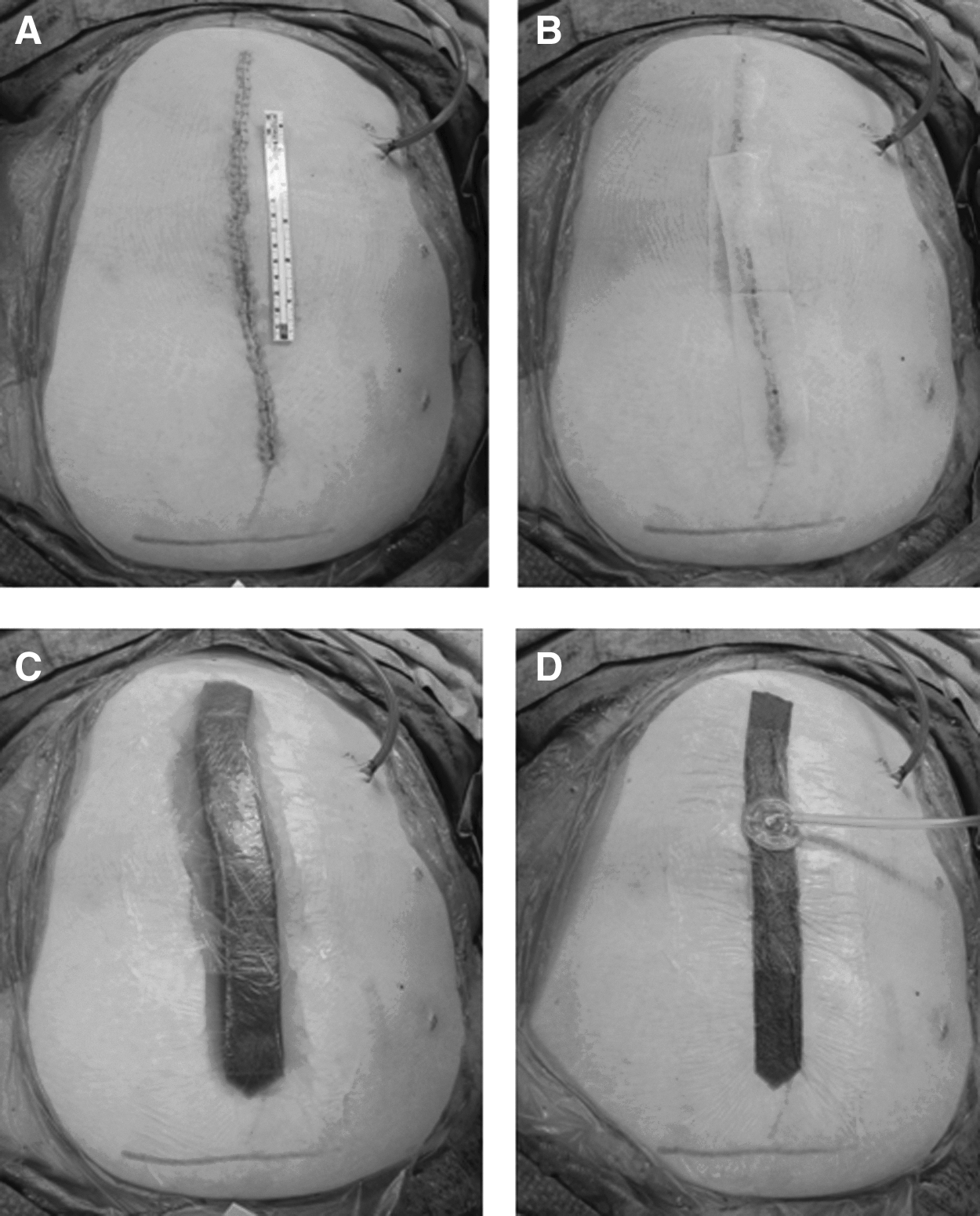
Placement of NPT on a closed incision.
The primary outcome variable of the study was the 30-d incidence of SSI in the midline wound. Surgical site infection was defined as the need for an antibiotic for wound erythema, the post-operative opening of an incision, percutaneous drainage, or the need for surgical debridement. Infections were divided further into the categories of major or minor SSI. Minor SSIs were defined as those requiring an antibiotic or local debridement at the bedside or in the office, or by the opening of the incision. Major SSIs were defined as any wound complication requiring re-operation, re-admission, or interventional radiology for management.
Data analysis was done with R statistical software (R Foundation for Statistical Computing, Vienna, Austria). The Student t-test, chi-square test, and regression analysis were used where appropriate. A value of p≤0.05 was considered statistically significant.
Results
During the study period, 188 open repairs of ventral hernias were done on high-risk patients. A total of 69 patients were excluded because of an anterior-component separation (30 patients), a concomitant panniculectomy (21 patients), or an active fistula (18 patients). The data for a total of 119 patients (70 of whom had SWDs and 49 of whom had NPT) with potentially contaminated or infected ventral hernia repairs were analyzed subsequently. The output from NPT dressings was nominal in all patients (less than 10 mL for the duration of therapy).
Univariate analysis showed that patients treated with an SWD and those treated with NPT were similar in age, gender, BMI, medical co-morbidities (smoking, DM, COPD, immunosuppression, and steroid use), number of prior abdominal operations, number of prior hernia repairs, abdominal wall defect size, and OR time (Table 1). The SWD group had a significantly lower mean ASA Physical Status Classification than did the NPT group (3.0±0.5 vs. 2.8±0.4; p<0.01). The NPT group had significantly more component separations (endoscopic and posterior) than did the SWD group (52.9% vs. 69.4%; p<0.01)
ASA=American Society of Anesthesiologists Physical Status Classification; BMI=body mass index; COPD=chronic obstructive pulmonary disease; DM=diabetes mellitus; OR=operating room.
In total, 28 (23.5%) patients developed a SSI within 30 d after surgery. Prophylactic NPT did not prevent SSI within 30 d after surgery to a greater extent than did a standard SWD (25.8% SWD vs. 20.4% NPT; p=0.50). The two groups showed no difference with respect to minor or major complications (SWD: 12 minor, six major; NPT: eight minor, two major; p=0.45). Examination of the rate of SSI out to one year after surgery, to evaluate any difference in delayed wound complications between the two groups, identified wound complications in 36 (30.3%) patients, without a difference in the SWD and NPT groups (31.4% SWD vs. 28.6% NPT; p=0.74). Seventy-three (61.3%) patients were identified as having had a previous surgical site infection. Neither NPT or an SWD had an effect on the development of an SSI in patients who had had a previous SSI (NPT: p=0.61; SWD: p=0.92).
Multiple factors were associated with an increased risk of developing a SSI within 30 d post-operatively, including ASA Physical Status Classification (p=0.02), BMI (p=0.05), defect area (p<0.01), DM (p=0.01), number of prior abdominal operations (p=0.01), number of prior hernia repairs (p<0.01), or OR time (p<0.01) (Table 2).
ASA=American Society of Anesthesiologists Physical Status Classification; BMI=body mass index; COPD=chronic obstructive pulmonary disease; DM=diabetes mellitus; OR=operating room.
Discussion
The present study evaluated the effect of NPT on closed, high-risk incisions following the open repair of ventral hernia. Although we hypothesized that NPT would reduce the risk of SSI in potentially contaminated and infected patients, we found that these patients had the same incidence of SSI as patients receiving a SWD after herniorrhaphy. Although the study was not randomized, it is one of the first to review prophylactic NPT prospectively for closed abdominal incisions.
Negative-pressure wound therapy was first introduced in the 1990s [6–11]. Its use for acute, chronic, and traumatic wounds has been an effective means of managing complex wounds. Prophylactic NPT has also become popular after operations with a high risk of surgical site infection. For patients undergoing median sternotomy, NPT reduces the rate of sternal deep incisional infection in patients with diabetes, obesity, smoking, those undergoing bilateral harvesting of internal mammary arteries, and other risk factors [17,25,26], and has shown a similar benefit when used on high-risk limb incisions, including those following trauma or orthopedic and vascular procedures [24,27–31]. Because of the high risk of SSI (27%–41%) in patients with potentially contaminated and contaminated ventral hernias [2–4], new methods for reducing wound morbidity are sought. The use of NPT described in the cardiac and orthopedic literature suggested it as an exciting option for high-risk VHR, and was the foundation for our investigation of it in this setting.
The hypothesized mechanisms by which NPT influences wound morbidity include reduced lateral tissue stress, increased appositional forces on incisions, and improved wound perfusion [32,33]. Others have shown that hematoma and seroma formation under a closed incision is reduced with the application of NPT [27,28,34]. These effects are clearly advantageous in the population in which NPT was investigated in the present study. Lateral wound stress induced by obesity, impaired wound perfusion as a result of prior incisions, and large wound dead spaces for seroma/hematoma formation were all present in the patients undergoing VHR in our study. Despite this, we were unable to document a benefit for NPT over SWD.
Our study has some limitations. First, the patient population, as in many studies of open VHR, was non-homogeneous. For the individual patient, differences in pre-operative risk factors, medical co-morbidities, and details of hernia repair (hernia size, type of mesh used in repair, OR time) make each hernia repair a unique situation. Second, a variety of techniques for hernia repair (retromuscular repair alone, retromuscular repair with endoscopic component separation, retromuscular repair with posterior component separation) were used during the study period. Knowing that open incisions with anterior components separation are at a greater risk of SSI than are incisions with either endoscopic or posterior components separation, we chose to exclude from our analysis patients with these incisions, making our patient population a more homogeneous group [22,23]. Despite this, there were significantly more component separations in the NPT group than in the SWD group. This occurred because we changed our technique over the course of time, performing fewer hernia repairs with endoscopic components separation and more with open posterior components separation during the last two years of the study. During this same period we began using NPT for high-risk wounds, on the basis of the available cardiac and orthopedic literature. Because the treatments used in the study were not determined by randomization, NPT was used in more patients undergoing posterior component separations than was SWD.
Despite these limitations, the results of this study warrant consideration. Prior investigations showed a benefit of NPT in high-risk cardiac and orthopedic incisions. Only two cases in the literature describe its use on abdominal incisions. Stannard et al. reported on the results with NPT used for closed midline incisions following total abdominal hysterectomy in two morbidly obese women who had DM and ostomies as additional risk factors for surgical site infection [25]. No surgical site infections were noted in these patients with 4 d of NPT, although one of the patients had a partial wound separation on day 14 when her staples were removed. However, it is impossible to reach any conclusions on the basis of this limited experience with only two patients, therefore making our study the first to evaluate the use of NPT with at-risk abdominal incisions in a large cohort. Given the retrospective, non-randomized nature of our study, our findings should ideally be confirmed with a prospective, randomized study in this challenging patient population.
The use of NPT for closed surgical incisions after the repair of potentially contaminated or infected large ventral hernias did not reduce the 30-d incidence of SSI in our study of 119 patients. Although prophylactic NPT has reduced wound morbidity in some surgical populations, it does not appear to offer the same improvement in wound morbidity in the open repair of ventral hernias at high risk for contamination and potential contamination.
Footnotes
Author Disclosure Statement
Yuri Novitsky serves as a speaker for Lifecell, Inc. (Branchburg, NJ), and Davol, Inc. (Warwick, RI), and as a consultant for Davol and for Kensey-Nash, Inc. (Exton, PA). Michael Rosen serves as a speaker for Lifecell, Inc., and receives research support from Lifecell, Inc., Davol, Inc., W.L. Gore, Inc. (Newark, DE), and the Cook Group, Inc. (Bloomington, IN). None of the other authors have relationships to disclose.