
Abstract

Two months after surgery the patient developed intermittent fever and a new cavitating lesion of the right lung (Fig. 1). Computed tomography (CT) revealed an abscess in the right upper lobe (Fig. 2). Image-guided percutaneous drainage of the abscess yielded P. aeruginosa and S. marcescens, which accorded with the pathogens from the patient's previously treated VAP, but failed to resolve the lesion in his lung, leading to thoracotomy and resection. Pathologic examination revealed a chronic lung abscess with extensive scarring and osseous metaplasia. The patient recovered from the thoracotomy but died 3 mos later from multiple organ dysfunction syndrome.
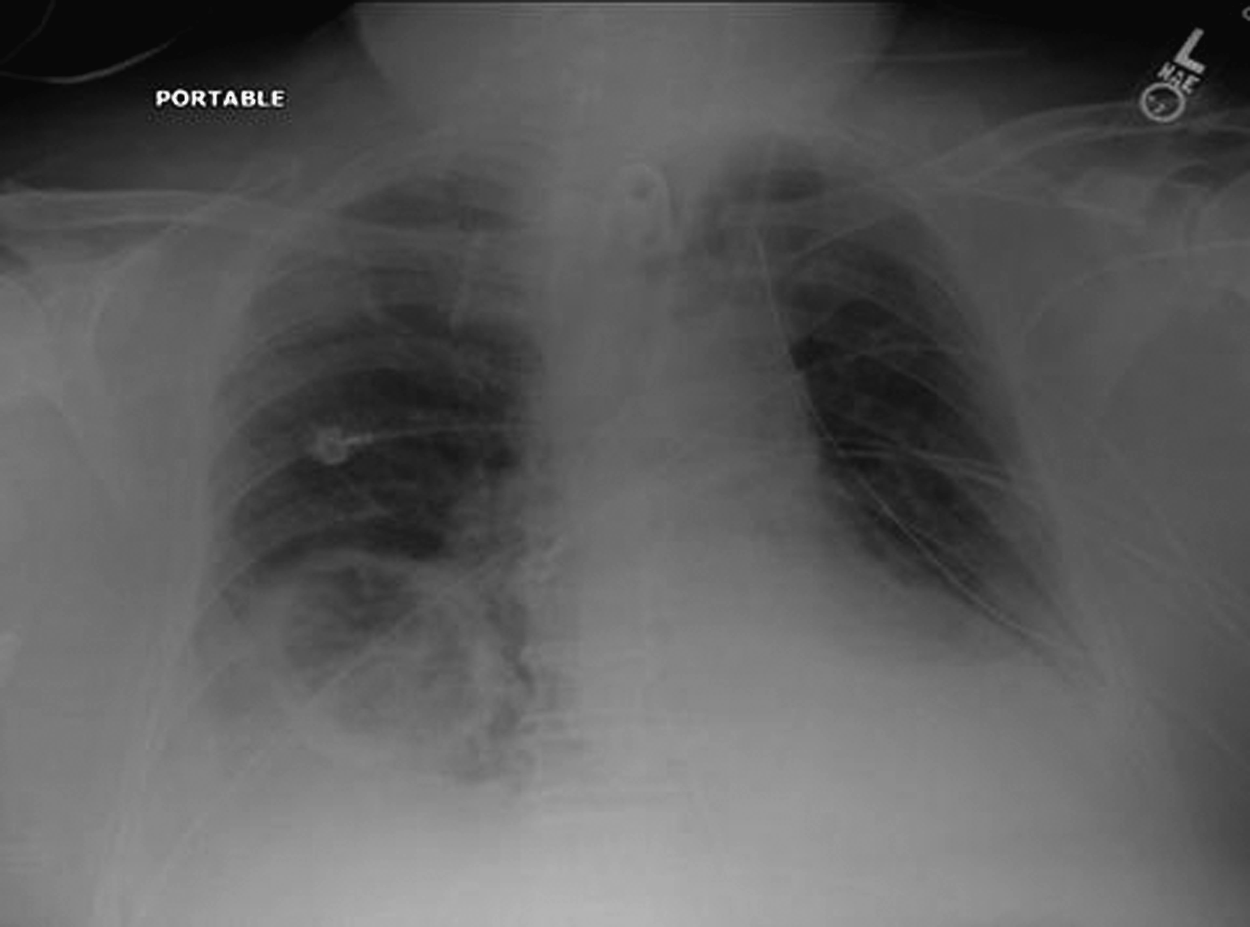
Chest radiograph showing a cavitary lesion of the right lung. 127×94 mm (96×96 dpi).
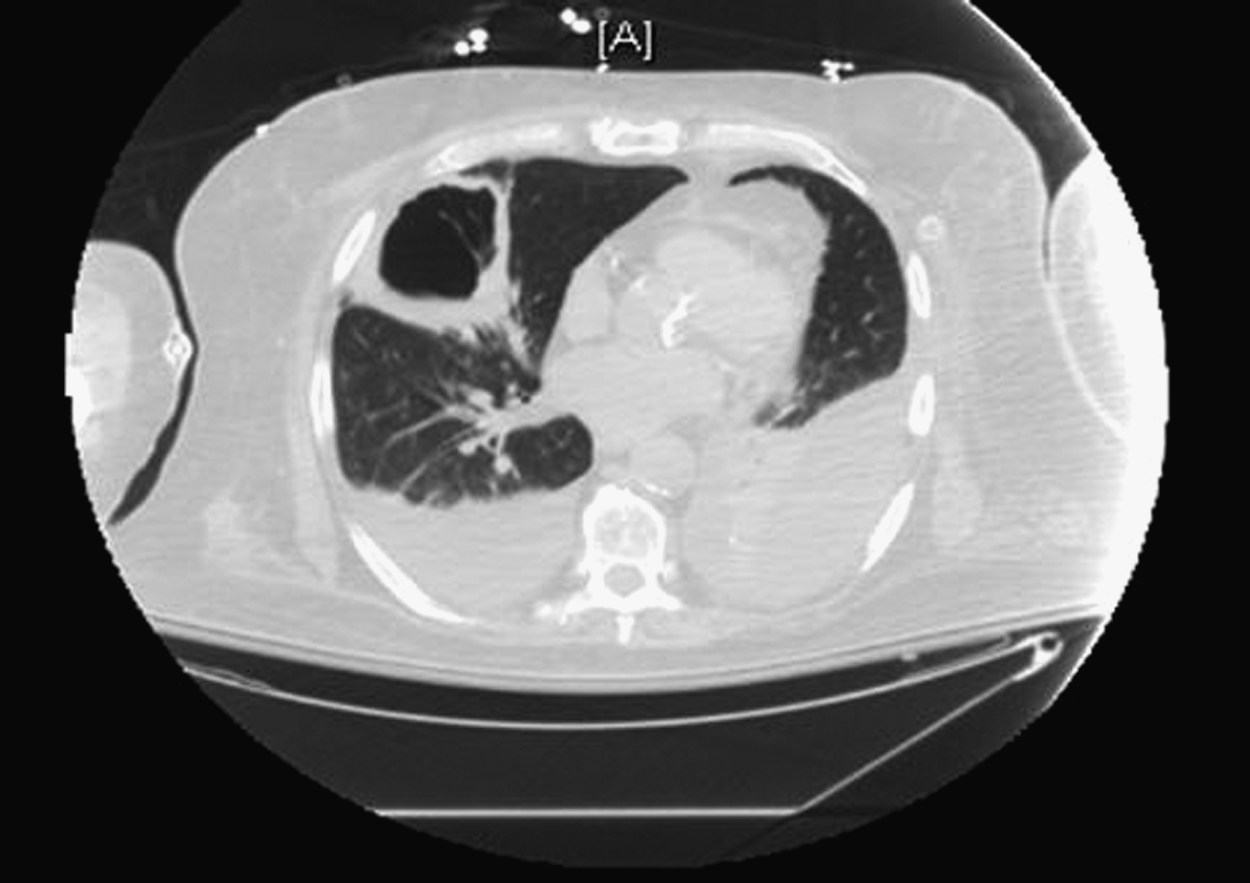
Computed tomogram of the chest clearly showing the patient's abscess and large bilateral pleural effusions. Empyema was excluded. 127×89 mm (96×96 dpi).
A circumscribed collection of pus within lung parenchyma, lung abscess is caused most commonly by the aspiration of oropharyngeal flora. Other recognized mechanisms of its causation include trans-diaphragmatic spread from subphrenic collections of pus and hematogenous seeding from remote infection. Lung abscess falls within a spectrum of lung infection that includes lung gangrene and necrotizing pneumonia, which are usually defined by the presence of multiple abscesses [1].
In the early twentieth century (1909–1923), the rate of mortality from lung abscess in a series of patients at the Massachusetts General Hospital (MGH) was 75% [2]. Open drainage of lung abscesses decreased mortality from these lesions to 20%–35%; however, the true therapeutic advance against these lesions occurred with the discovery of antibiotics, which decreased the mortality from lung abscess to 8.7% in another series at the MGH (1943–1956) [2]. At the same time, improvements in dental hygiene helped decrease the incidence of lung abscess. Currently, aspiration remains the principal cause of lung abscesses; accordingly, the main risk factors for lung abscess formation are a patient's inability to control the airway, an altered sensorium, and poor dentition. In the pre-antibiotic era, lung abscess was usually to the result of infection with a single anaerobic pathogen; currently, it is more likely to be caused by polymicrobial infections [1].
CT of the chest reveals the precise location and size of the lesion, most commonly in the right lung. By CT, a lung abscess may appear as a fluid-filled structure or as an air-filled cavity in the setting of spontaneous drainage into a bronchus. The differential diagnosis of these lung lesions includes infectious, inflammatory, and neoplastic processes. Among non-bacterial infectious causes of cavitary lung lesions are fungal and mycobacterial infections (including tuberculosis), echinococcal cysts, and Pneumocystis pneumonia. Congenital and inflammatory lesions are rare, and include bronchogenic cysts and ischemic necrosis. Neoplasia can lead to cavitary lesions secondary to internal cyst formation, internal liquefaction, or treatment-related necrosis.
Antibiotic therapy directed at anaerobic and aerobic bacteria is the first line of treatment for a lung abscess. Patients with lung abscesses were treated historically with clindamycin for 6–12 wks or until resolution. More recent series have shown that beta-lactamase inhibitor combinations are equally effective [3]. Patients who do not respond to antibiotic therapy may be treated with percutaneous drainage, for which the rate of success in a recent series of 40 patients was 83% [4]. Patients in whom antibiotic therapy and drainage fail and who can tolerate a thoracotomy or thoracoscopy should have an abscess resected. Despite these advances, the prognosis remains guarded, with mortality associated with lung abscess reportedly ranging from 10% to 20% [1]. Large abscesses, a low serum albumin concentration, anemia, and specific pathogens (e.g., Staphylococcus aureus, Klebsiella pneumoniae, P. aeruginosa) have been associated with poor prognosis [5].