
Abstract

A 31-year-old female of Southeast Asian origin who had been living in the United Kingdom for the past three years presented to the emergency department with a soft tissue swelling on the dorsal ulnar side of her right hand. Two months prior, it had been diagnosed as a ganglion. The emergency department physician incised the swelling; culture of the pus revealed anaerobic growth only at 48 h. One week later, the patient returned to the emergency department with fever and was admitted for pyrexia of unknown origin. She had no medical history of relevance, took no medication, and had not traveled abroad for the prior three years. She denied cough, chest or abdominal pain, or urinary or gastrointestinal symptoms. Examination revealed a soft swelling on the dorsal ulnar aspect of the right wrist with an open incision that exposed a base of white fibrous tissue. The skin was not cellulitic and she had no functional deficit. The concentration was C-reactive protein 92mg/L and the erythrocyte sedimentation rate was 82 mm/h. Her chest radiograph was normal. A radiograph of the affected hand showed erosions at the base of the fourth and fifth metacarpals, with overlying soft tissue swelling (Fig. 1). Surgical exploration revealed a collection of characteristic rice bodies extending from the fourth extensor compartment to the distal carpal bones on the ulnar side of the hand. Histology showed caseating granulomas mixed with epitheliod histiocytes and multinucleated giant cells. The bone biopsy showed bony spicules and stromal tissue elements, as well as caseating granulomas. Ziehl-Nielson stains were negative. Microbiology revealed the presence of both acid- and alcohol-fast bacilli. The patient was started on a six-month course of anti-TB medication. Seven days later, a delayed primary closure was performed, which healed uneventfully.
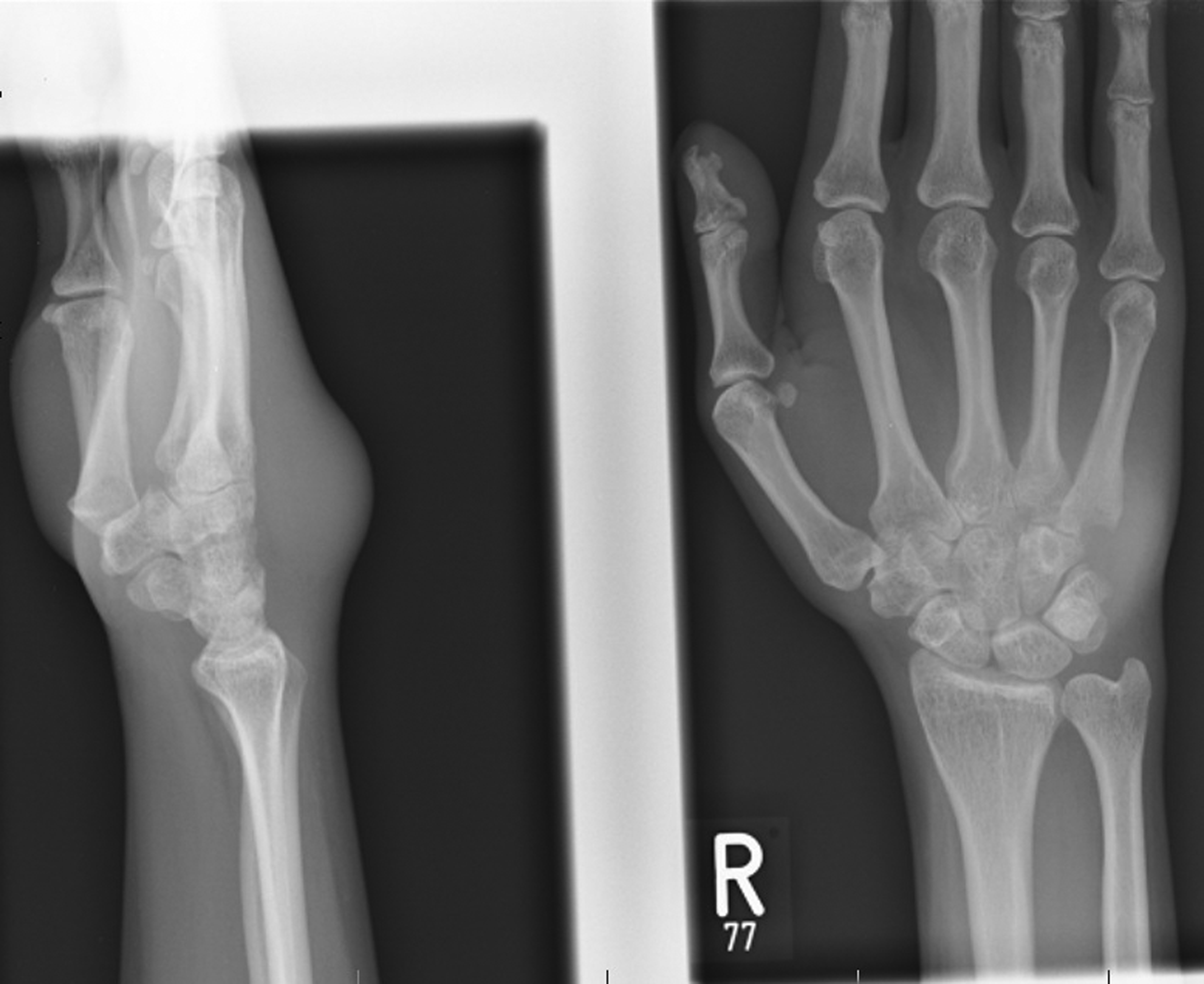
Antero-posterior and lateral pre-operative radiographs (right hand). Soft tissue collection with bony erosion at the base of the fourth and fifth metacarpals.
Extra-pulmonary TB currently accounts for 15 percent of TB presentations in the developed world but there is evidence that its incidence is on the increase [1]. Although diagnosis can be difficult, there are key typical features, that may be helpful: Most patients with skeletal TB report no history of pulmonary TB nor do they have classic pulmonary findings on chest radiography; patients tend to present in adulthood (ages 30–40 years); diagnosis is often delayed for months [2]; Ziehl-Nielson stains and cultures frequently are negative. The presence of a caseating granuloma with or without confirmed histopatholgic findings should warrant a therapeutic trial of anti-TB medication. Culture of pus by swab is insufficient; granulation tissue must be sent to both microbiology and histopathology, otherwise the diagnosis can be missed. The radiologic appearance of TB is variable. This case resembles one of six patterns of skeletal TB described by Al-Qattan et al.— bony destruction resembling septic osteoarthritis [3]. Other patterns include well-defined cystic lesions, honeycomb pattern, lytic/sclerotic lesions, and spina ventosa (Latin for “short bone filled with air”). Osteoarticular TB also can be difficult to differentiate from septic arthritis. However, an osteolytic focus with minimal surrounding sclerosis and preservation of joint space should favor the diagnosis of TB [4]. With the combination of surgical debridement and the correct anti-TB medications, the prognosis is good.[3]